
Abstract
Engaging communities is a key strategy to increase COVID-19 vaccination. The Centers for Disease Control and Prevention (CDC) COVID-19 Vaccine Confidence Rapid Community Assessment Guide was developed for community partners to obtain insights about barriers to COVID-19 vaccine uptake and to engage community partners in designing interventions to build vaccine confidence. In spring 2021, 3 CDC teams were deployed to Alabama and Georgia to conduct a rapid community assessment in selected jurisdictions. Data collection included interviews, listening sessions, observations, and street intercept surveys. We identified 3 facilitators and barriers to vaccine uptake: (1) planning and coordination, (2) capacity and implementation, and (3) attitudes and beliefs. We found that the use of the rapid community assessment in Alabama and Georgia was feasible to implement, useful in eliciting unique community concerns and dispelling assumptions, and useful in informing intervention strategies. Our results underscore the importance of community engagement in COVID-19 mitigation strategies.
After recommendations in December 2020 from the Advisory Committee on Immunization Practices to use the initial COVID-19 vaccines, US public health efforts have centered on facilitating equitable vaccine distribution and on building vaccine confidence.1,2 Studies conducted in 2020 indicated that 20% to 40% of US adults expressed vaccine hesitancy.3,4 Vaccine-related variables (eg, origin, protection duration, adverse events), political affiliation, and sociodemographic characteristics predicted hesitancy.3-5 Engaging communities and individuals in a collaborative, equitable, and sustainable fashion is fundamental to building vaccine confidence. 6
To assess and address community concerns about vaccines, the Centers for Disease Control and Prevention (CDC) developed the COVID-19 Vaccine Confidence Rapid Community Assessment Guide 7 (RCA) for health departments, health systems and clinics, community-based organizations, and other interested groups with connections to priority populations. The RCA, which was partially developed in 2020 and published in February 2021, can identify factors associated with low vaccination uptake, barriers and facilitators to vaccine confidence and uptake, and opportunities for intervention. 7 Given the urgency of the pandemic, the suggested RCA implementation time frame is 3 weeks: week 1 involves planning and buy-in (eg, identification of communities of focus), week 2 involves implementation and analysis (eg, data collection), and week 3 involves synthesizing and reporting findings (eg, presentations to communities). The RCA includes data collection tools (eg, vaccine rollout learning template, key informant interview templates, listening session tools), templates for analysis and interpretation (eg, observation forms), and synthesis tools for reporting. The guide is intended to be customized, allowing for flexibility relative to local context.
Purpose
In early spring 2021, CDC was invited to conduct RCAs in selected jurisdictions in Alabama and Georgia. The original SARS-CoV-2 virus was the predominant strain, and vaccine rollout for 3 vaccines (Pfizer-BioNTech, Moderna, and Janssen) was underway. By the time of the Alabama RCA (early March 2021), initial vaccinations prioritized health care personnel and residents of long-term care facilities (phase 1a); people aged ≥75 years and frontline essential workers (phase 1b); and people aged 65-74 years, people aged 16-64 years with medical conditions that put them at high risk of infection, and other essential workers (phase 1c), with later expansion to selected groups.8,9 By the time of the Georgia RCA (mid-April 2021), vaccinations had been expanded to all Georgians aged ≥16 years. 10 This case study documents implementation of the COVID-19 RCA in Sumter and Macon counties, Alabama, and in Bacon and Dougherty counties, Georgia, in spring 2021.
Methods
RCA Community Context
The Alabama Department of Public Health, in collaboration with the Alabama Governor’s Office of Minority Affairs, selected Sumter and Macon counties for its RCAs. Both counties had a high index for social and pandemic vulnerability (eg, higher than average levels of poverty/high rates of COVID-19 infection) and are in the rural, south-central Black Belt region (areas deeply rooted in racism and injustice that have left a legacy of poverty and other health disparities).11-16 Sumter County had a population of about 12 400, of which 71% were non-Hispanic Black. 12 Macon County had a population of about 18 000, of which 80% were non-Hispanic Black. 11 Macon County is home to Tuskegee University, a historically Black university, and the site of the US Public Health Service Syphilis Study, in which the US government unethically withheld medical treatment from Black men with syphilis without their consent, from 1932 to 1972. 17
The Georgia Department of Public Health (GDPH) selected Bacon and Dougherty counties for its RCAs. Both counties had a high index for social and pandemic vulnerability but differed in their racial and ethnic composition.18-22 Bacon County, in southeast Georgia, had a population of about 11 164, of which 73% were non-Hispanic White. 19 Bacon County, which leads the state in blueberry farming, 23 included 3000-4000 migrant farmworkers (R. Parks, MD, GDPH Southeast Health District, personal communication, April 12, 2021). In response to a COVID-19 outbreak that occurred among migrant farmworkers in May 2020, farmers and local leaders formed a COVID-19 roundtable composed of multisectoral representation to plan for mitigation. 24 Dougherty County, in southwest Georgia, had a population of about 86 000, of which 71% were non-Hispanic Black. 18 The area is characterized as urban and has a substantial manufacturing base. 25 At the beginning of the COVID-19 outbreak in 2020, Dougherty County had the fourth highest rate of COVID-19 infections in the country, averaging more than 1000 cases and 75 deaths per 100 000 population. 22
This study was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy for the protection of human subjects in research. The research was authorized under the COVID-19 Public Health Emergency waiver.
RCA Planning
For week 1 activities, we facilitated initial interviews between CDC staff and state public health officials, which were used to select counties, communities of focus, the implementation time frame, and members of the assessment teams. Priority RCA data collection methods included key informant interviews, listening sessions (guided discussions with a small group of participants chosen based on their role in the community), and observations. 7 To facilitate these discussions, we adapted questions from the RCA key informant interview/listening session template. CDC deployed 1 team to Alabama from March 8 through 25, 2021, and 2 teams to Georgia from April 11 through 16, 2021. We jointly selected these time frames to accommodate local preferences, geographic logistics, and expected opportunities to engage with community members at planned community events.
RCA Implementation: Data Collection and Analysis
For week 2 activities, teams first talked with leadership in each county (eg, district public health officers, mayors, county commissioners) and then asked for initial referrals to community members and organizations. We used a snowball sampling approach, in which participants provided referrals for other potential participants to recruit for interviews and listening sessions. We continued the snowball sampling approach until saturation was reached in each location, meaning responses from participants became redundant and no longer elicited new information. Depending on interview type and geographic location of the community members, 1 or sometimes 2 or more CDC team members conducted interviews and listening sessions. Listening sessions typically involved group interviews with members of a selected group (eg, faith community, school staff, nurses in a health care system) in a single setting.
Our teams began key informant interviews and listening sessions with an overview of the objectives, which were conducted in a conversational manner. We informed participants that no identifying information would be reported. Teams also conducted community observations (eg, signage for vaccination locations) and driving tours to observe facilities providing COVID-19 vaccinations and to obtain staff perspectives on facilitators and barriers to COVID-19 vaccine uptake specific to local vaccine delivery systems. Lastly, teams used street intercept surveys, where residents were recruited from public spaces (eg, parks, restaurants) and asked about their feelings about COVID-19 vaccinations.
The Alabama team completed 21 key informant interviews, 6 listening sessions with an average of 10 participants, 5 community observations (eg, vaccine clinics, pharmacies), 2 driving tours, and 9 intercept surveys. Participants included business owners, community-based organizations (CBOs), county governance, faith-based leaders, first responders, public and private health care providers, university staff, school administrators, and residents. The 2 Georgia teams completed 54 key informant interviews, 13 listening sessions with an average of 6 participants, 7 driving tours, 10 street intercept surveys, and 6 community observations (eg, observing vaccination wait lines in pharmacies). Participants included business owners, CBOs, county governance, extension services, farmers, public and private health care providers, members of the media, school staff (teachers, school bus drivers, and school board members), and residents.
CDC team members took notes during or after each interview or listening session. At the end of each day, team members individually or collectively summarized notes using RCA templates. Teams met and reached consensus on key themes and recommendations for action.
Outcomes
Findings and Plan for Action
We identified the following facilitators and barriers associated with vaccine uptake across all sites: (1) planning and coordination, (2) capacity and implementation, and (3) attitudes and beliefs (Table 1 and Table 2). Some facilitators (eg, mobilized county leadership) and barriers (eg, lack of community outreach) were common across all sites, and others, described hereinafter, were unique to each site.
Selected facilitators and barriers associated with COVID-19 vaccine uptake based on the COVID-19 Rapid Community Assessment, a Alabama, March 2021

A rapid community assessment was undertaken using the Centers for Disease Control and Prevention COVID-19 Vaccine Confidence Rapid Community Assessment Guide 7 to obtain actionable insights about barriers to COVID-19 vaccine uptake and to engage community partners in designing intervention strategies to build COVID-19 vaccine confidence.
Selected facilitators and barriers associated with COVID-19 vaccine uptake based on the COVID-19 Rapid Community Assessment, a Georgia, April 2021

A rapid community assessment was undertaken using the Centers for Disease Control and Prevention COVID-19 Vaccine Confidence Rapid Community Assessment Guide 7 to obtain actionable insights about barriers to COVID-19 vaccine uptake and to engage community partners in designing intervention strategies to build COVID-19 vaccine confidence.
Alabama
Respondents in Alabama reported limited vaccine supply and vaccination sites, especially outside of public health agency settings, distant vaccination sites, and limited appointment schedules as barriers to vaccine uptake, particularly for people without access to personal or public transportation. These access barriers contributed to a feeling of neglect in outlying communities. Many residents, including older people and people without broadband internet access, found online scheduling and registration to be a barrier to vaccination. We observed that most vaccination clinics were open only during weekday mornings, and this time slot was especially difficult for people who had work and childcare commitments. The sense of urgency about ending the pandemic was widespread in both counties, based on the personal experiences of illness and loss.
We found some differences between the counties. For example, mistrust of government was more prominent in Macon County than in Sumter County. Macon County participants perceived that vaccine distribution in Alabama reinforced preexisting racial disparities. They also expressed frustration with long-standing government neglect of broader health issues in their community, such as chronic disease and health care infrastructure. In Sumter County, public health officials were pleased with the rollout of COVID-19 testing and were interested in offering vaccines at the same sites used for testing.
We presented the recommendations informed by these findings to the Sumter and Macon County health departments, the Alabama Department of Public Health, and the Governor’s Office of Minority Affairs, as well as jointly to all nongovernmental and governmental organizations engaged with the RCA (Table 3). We also submitted our findings in a report to the Alabama Department of Public Health (CDC, unpublished report, May 2021).
Selected recommendations based on the COVID-19 Rapid Community Assessment a in Alabama and Georgia jurisdictions, March and April 2021
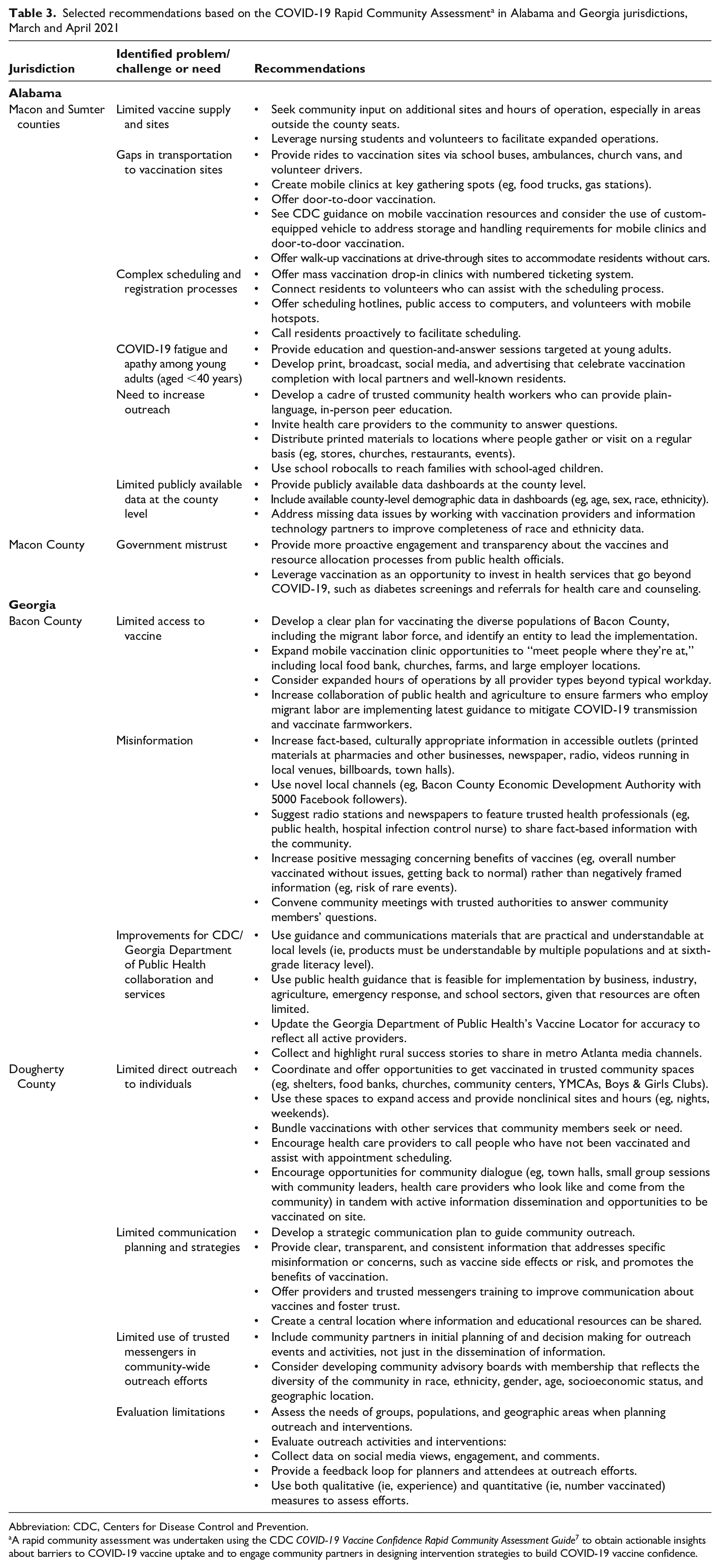
Abbreviation: CDC, Centers for Disease Control and Prevention.
A rapid community assessment was undertaken using the CDC COVID-19 Vaccine Confidence Rapid Community Assessment Guide 7 to obtain actionable insights about barriers to COVID-19 vaccine uptake and to engage community partners in designing intervention strategies to build COVID-19 vaccine confidence.
Bacon County, Georgia
In Bacon County, because of its agricultural base, the COVID-19 Roundtable initially sought guidance from the Georgia Department of Agriculture rather than from the public health sector. The Georgia Department of Agriculture played a major role early in the pandemic in facilitating testing capacity and communication about COVID-19 mitigation, especially among farmers and their workers. To reach farmworkers, the GDPH Southeast Health District office facilitated on-site vaccinations, and a federally qualified health center offered vaccinations during the evening and on Saturdays to accommodate farmworkers’ schedules. Another federally qualified health center called patients to register them for an appointment. The area agency on aging was instrumental in facilitating vaccinations for older adults. Members of the local media were used sparsely for outreach, although an emergency management official provided COVID-19 vaccination information on a local radio show. To meet widespread staffing shortages, the public health district shifted county health department staff to neighboring county health departments several days per week to provide vaccinations in these counties, thereby limiting drop-in vaccination opportunities at the health department facility. Mistrust of government increased when it was established that the outbreak reported in March 2021, which garnered national media coverage for Bacon County as a COVID-19 “hot spot,” was the result of a CDC error that misclassified cases from May 2020 to 2021.24,26 (CDC staff apologized for this error on behalf of the agency and confirmed it would be brought to the attention of appropriate individuals at CDC.) Skepticism toward federal guidance increased after the perceived impracticality of selected guidance (eg, quarantine protocols for exposed first responders when only a handful were available countywide). In addition, residents stated that CDC COVID-19 communication materials (eg, toolkits) did not resonate with them because the material did not reflect rural life.
CDC deployers expedited analysis and report preparation while in the field, allowing us to present the RCA findings and recommendations to members of the COVID-19 Roundtable and GDPH in an already scheduled Roundtable meeting (April 16, 2021; Table 3). Three team members presented findings and addressed community members’ questions and concerns. We also submitted our findings in a report to GDPH (CDC, unpublished report, June 2021).
Dougherty County, Georgia
Mass communication efforts (eg, weekly press conferences, public service announcements, Facebook Live events, a weekly radio program) increased awareness of COVID-19 vaccines and their availability in Dougherty County. A Vaccine Equity Unit established within the Dougherty County Health Department facilitated vaccination uptake. A mass influenza vaccination simulation conducted in fall 2020 prepared health systems to deploy COVID-19 vaccines in 2021. Health department staff hosted 2 events in the student center at Albany State University to answer questions about the COVID-19 vaccine. Despite mass communication efforts, many respondents discussed the inability to find trusted, transparent, and easy-to-understand information about vaccines. Based on respondents’ comments, the Dougherty County team determined that information was characterized as “trusted, transparent, and easy to understand” if it was free from a political agenda, stated the benefits and risks of vaccination, included what is known and not known about short- and long-term side effects of the vaccine, and was communicated in plain language.
The limited trust that residents already harbored for public health and government was further hindered during the pandemic. Respondents linked this mistrust to historical and current policies and practices that harmed Black people’s well-being (eg, efforts to reduce voting rights and access, the state not adopting Medicaid expansion, disproportionate rates of chronic and mental illness without corresponding equitable access to care). This mistrust powered beliefs about vaccines being used to disproportionately harm Black people.
Separately, but related to trauma and emotions concerning the pandemic, a few respondents discussed how some Black community members, particularly faith-based leaders, felt blamed and stigmatized for the spread of COVID-19 in the community. Dougherty County received national and international media coverage at the beginning of the pandemic when 2 funerals of Black community members were labeled as superspreader events that drove the outbreak in Albany in late March 2020. 27 Some respondents were confused by the lack of public discourse potentially linking the SNICKERS Marathon, a major event that brought thousands of national and international tourists to the area weeks prior to the funerals, as a possible origin of the local outbreak. 28 Some respondents believed that the Black faith-based community was unfairly scapegoated, further entrenching feelings of mistrust of larger systems (Table 2).
We presented the recommendations informed by these findings to the Dougherty County Health Department, health care providers at Phoebe Putney Memorial Hospital, and GDPH (Table 3). We also submitted our findings in a report to GDPH (CDC, unpublished report, May 2021).
Lessons Learned
We found that the use of the RCA in Alabama and Georgia was feasible to implement and of value to health departments and community partners in obtaining information on barriers to COVID-19 vaccination. Our study also showed the value of listening to communities’ perspectives. RCAs can help to dispel assumptions about communities that might share general characteristics, such as rurality, but differ because of unique local factors. The insights gained from meeting with community members directly to dispel assumptions are especially worthwhile in settings with a high index for social vulnerability and historical trauma. For example, in Alabama, the Alabama Department of Public Health initially requested us to investigate vaccine hesitancy; however, when implementing the RCA, we found that the main concerns were associated with inequitable access to vaccines. This information led the public health department to adjust its strategies and priorities. In Bacon County, some community leaders who criticized the Bacon County Health Department’s vaccination services were unaware that the limited vaccination capacity at the county facility was the result of district-wide staffing shortages until we presented the results of the RCA. We also found it useful to hear about the community’s dissatisfaction with CDC’s coding error that brought unwanted national attention to the county.
RCAs can be used as a source of information for the development of practical recommendations to improve vaccine confidence, especially for health departments that are considering conducting RCAs to recognize rather than simply describe the state of vaccine confidence in a community. To support this objective, health departments or sponsoring organizations should consider how resources will be leveraged to implement recommendations before they conduct an RCA. Health departments should also clarify the roles of their own staff, the sponsoring organization, and community partners in the implementation process and consider impact evaluation. To avoid bias, we suggest that team members who collect data come from outside the community that is being assessed. While CBOs and leaders have deep personal and professional knowledge of the issues affecting residents, they do not need special tools to articulate this knowledge to themselves. Rather, RCAs serve as a mechanism for communities to elevate their concerns to policy makers and funding bodies.
Our case study had at least 4 limitations. First, although we used the same topical areas of focus to guide all data collection, we did not use standardized questions across sites or interviews, thereby limiting comparisons across jurisdictions. Second, we may not be able to generalize our findings to the entire population in each jurisdiction or to populations with similar demographic characteristics in other jurisdictions. Third, social desirability bias may have caused some respondents to conceal or minimize vaccine hesitancy from health authorities. Finally, additional study is needed to assess the extent to which recommendations were implemented by community partners and whether practices were changed.
Engaging communities is critical to understanding barriers to and enabling factors for vaccine confidence and uptake. This case study demonstrates the value of community engagement in COVID-19 mitigation. Use of the CDC COVID-19 RCA can be an important tool to elicit intervention strategies for COVID-19 vaccination.
Footnotes
Acknowledgements
The authors thank the following from Sumter County, Alabama, for their participation: the Alabama Department of Public Health, the Alabama Governor’s Office of Minority Affairs, the West Central Health District, the mayors of Livingston and York, the Sumter County Commissioner, the Sumter County Council, the Sumter County School District, the Rural Alabama Prevention Center, the Theo Ratliff Activity Center, Health and Wellness Education Center, Shiloh Zion Baptist Church, Livingston Fire and Rescue, Coleman Center for the Arts, and local business owners and residents.
The authors thank the following from Macon County, Alabama, for their participation: the Alabama Department of Public Health, the Alabama Governor’s Office of Minority Affairs, the East Central Health District, the mayor of Tuskegee, the Alabama Emergency Management Agency, the Macon County Health Department, the Macon County Courthouse, the Macon County Board of Education, Tuskegee University, the National Center for Bioethics in Research and Health Care, the Notasulga Town Hall, Macon Cares, Alpha Phi Alpha Fraternity, Incorporated—Gamma Phi Chapter, community advocates, local business owners, and residents
The authors thank the following from Bacon County, Georgia, for their participation: the Georgia Department of Public Health, the Bacon County Health Department—Southeast Health District, the mayor and manager of Alma City, the Bacon County COVID-19 Roundtable, the Bacon County Emergency Management Agency, Bacon County Hospital and Health System, Alma/Bacon Fire and EMS, Bacon County Sheriff’s Office, the Bacon County Board of Education, the Bacon County UGA Extension Office and members of the farm bureau, the McKinney Medical Center (South Central Primary Care Center), faith-based leaders, local media (Alma Times, local radio station), and business owners and residents of Alma.
The authors thank the following from Dougherty County, Georgia, for their participation: the Georgia Department of Public Health, the Dougherty County Health Department—Southwest Health District, the Dougherty County COVID-19 Task Force, the mayor of Albany, the district chairman of Albany, the Marine Corps Logistics Base Albany, the coroner for Dougherty County, Albany State University, the Albany African American Ministerial Alliance, the Dougherty County School System, the Albany Housing Authority, the Phoebe Putney Health System, the local media, and business owners and residents of Albany.
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.