
Abstract
Objectives:
High rates of hospitalization and death disproportionately affected Black, Latino, and Asian residents of New York City at the beginning of the COVID-19 pandemic. To suppress COVID-19 transmission, New York City implemented a workforce of community engagement specialists (CESs) to conduct home-based contact tracing when telephone numbers were lacking or telephone-based efforts were unsuccessful and to disseminate COVID-19 information and sanitary supplies.
Materials and Methods:
We describe the recruitment, training, and deployment of a multilingual CES workforce with diverse sociodemographic backgrounds during July–December 2020 in New York City. We developed standard operating procedures for infection control and safety measures, procured supplies and means of transportation, and developed protocols and algorithms to efficiently distribute workload.
Results:
From July through December 2020, 519 CESs were trained to conduct in-person contact tracing and activities in community settings, including homes, schools, and businesses, where they disseminated educational materials, face masks, hand sanitizer, and home-based specimen collection kits. During the study period, 94 704 records of people with COVID-19 and 61 246 contacts not reached by telephone-based contact tracers were referred to CESs. CESs attempted home visits or telephone calls with 84 230 people with COVID-19 and 49 303 contacts, reaching approximately 55 592 (66%) and 35 005 (71%), respectively. Other CES activities included monitoring recently arrived travelers under quarantine, eliciting contacts at point-of-care testing sites, and advising schools on school-based COVID-19 mitigation strategies.
Practice Implications:
This diverse CES workforce allowed for safe, in-person implementation of contact tracing and other prevention services for individuals and communities impacted by COVID-19. This approach prioritized equitable delivery of community-based support services and resources.
During the first wave of the COVID-19 pandemic in April 2020, New York City was one of the world’s hardest-hit metropolitan areas. High rates of hospitalization and death disproportionately affected Black, Latino, and Asian residents. 1 On May 6, 2020, the City of New York established the Test & Trace Corps (hereinafter, Corps), a comprehensive initiative to suppress COVID-19 transmission. 2
The Corps used a 3-pronged approach to rapidly expand COVID-19 testing (Test), interview people with COVID-19 and elicit their contacts (Trace), and provide resources (eg, hotel, food, other supplies) to support safe isolation and quarantine (Take Care). The Corps was administered by staff from the Health + Hospitals Corporation, the New York City public health care system, in collaboration with the New York City Department of Health and Mental Hygiene and other government agencies.
Initially, Corps staff worked exclusively from home to conduct telephone-based contact tracing. 3 However, to better reach people in New York City who were unwilling to interact with contact tracers via telephone, had limited telephone service, or had inaccurate telephone numbers,3-7 the Corps implemented a workforce known as community engagement specialists (CESs) in July 2020. CESs made home visits to people who could not be reached by telephone-based contact tracers, and they conducted other community-based health promotion activities as needs arose.8,9
To our knowledge, data are lacking on in-person efforts covering a large metropolitan area for a combination of COVID-19–related contact tracing, dissemination of information and personal protective equipment (PPE), specimen collection, and policy implementation. Here, we describe the recruitment, training, and deployment of our CES workforce and activities in the first 6 months of operation.
Materials and Methods
CES Recruitment
We retained a hiring firm to facilitate the recruitment of applicants with at least a high school diploma and community health experience. We also consulted an existing community advisory board whose membership includes community and religious leaders from across the 5 New York City boroughs. Board members helped recruit a pool of Corps applicants from communities heavily impacted by COVID-19 and with language skills beyond English. Other desirable qualifications included backgrounds in medicine, nursing, epidemiology, community health, or case management.
After Corps candidates completed a prerequisite 6-hour online course on COVID-19 contact tracing, 10 those with experience and background (ie, medicine, nursing, epidemiology, community health, or case management) suitable for in-person interactions, including home visits and community-based work, received written or telephone explanation of the CES role. Those expressing reluctance in having face-to-face interaction with people with COVID-19 were considered for a telephone-based role. CESs received about 10% higher salaries than telephone-based contact tracers because their role required travel throughout New York City and in-person interactions during a pandemic.
CES Training
Because of COVID-19–era restrictions on in-person gatherings, all training, except the use of PPE, was conducted via online platforms.11,12 Self-paced courses via the employee intranet website covered topics such as sexual harassment, confidentiality, diversity and inclusion, and conflicts of interest. CESs also underwent a 5-day Corps orientation on New York City’s contact tracing standard operating procedures, telecommunication and database systems, and language interpretation services. Emails at least 3 times weekly provided continuing education; all materials were accessible via the employee intranet website. During routine web-based staff meetings, subject matter experts provided ongoing refresher trainings on updated standard operating procedures, database functionalities, and infection control and safety. Before each community-based activity (eg, visits to schools or travelers under quarantine), team leads worked with supervisors and CESs on protocols.
Infection Control and Safety
Strict infection control and safety measures were important in protecting CESs and community members.13,14 After an online infection control course, CESs underwent in-person training on infection control practices that included the proper donning and doffing of PPE. CESs were also required to conduct interviews at a distance ≥6 ft. A supervisor accompanied CESs on home visits at least once weekly to observe adherence to infection control measures and work processes.
CESs received instructions on self-monitoring for COVID-19 symptoms and reporting of potential infection to occupational health services. CESs with suspected or confirmed COVID-19 received free testing and paid time off to isolate. When COVID-19 vaccines became available, CESs were prioritized for vaccination.
CESs received general safety training covering environmental awareness, avoidance, and de-escalation of conflicts. With supervisor approval, CESs worked in pairs but still had to complete all home visits to which they had been individually assigned. CESs were instructed to immediately remove themselves from potentially harmful situations and to call their supervisors to report safety-related issues. Corps leadership received a daily summary report of safety issues; these issues were assigned to appropriate staff for follow-up. Corps leadership held open monthly forums to discuss CES experiences, challenges, and strategies in addressing safety issues.
Supplies and Transportation
All CESs received an iPad, mobile phone, rolling backpack, pens, clipboard, and client educational materials in multiple languages. Upon completion of infection control training, CESs received a 1-month supply of PPE, including surgical and N95 face masks, gloves, goggles, face shields, sanitizer wipes, hand sanitizer, and brown paper bags to hold waste. For monitored people (ie, people with COVID-19 and their contacts) who lacked telephone service, CESs provided mobile phones good for a 30-day period.
To enable multiple home visits per day, CESs were issued passes for unlimited access to the New York City public transportation system. CESs also had access to a taxi service through an iPad application if a home visit was >1 mile from the nearest public bus or train stop (this distance was reduced to a half mile during extreme weather) or a trip would require >2 bus or train rides.
Distribution of Workload
To determine the 50 neighborhood cohorts for community-based contact tracing, we examined the number and geocoded locations of new COVID-19 cases reported to the New York City Department of Health and Mental Hygiene in May–June 2020 and how they corresponded to public transportation hubs. Fifty nested clusters of New York City zip codes were assigned to 50 CES supervisors. Each supervisor oversaw approximately 10 CESs.
Logic built into the contact tracing database, Salesforce (Salesforce), a cloud-based customer relationship management software, triaged to the CESs any records of people missing telephone numbers or not responding to ≥3 calls from telephone-based contact tracers. CES supervisors then sorted those records by zip code, address, and (if applicable) telephone number; they attempted to assign people in the same geographic area or with the same telephone number to the same CES. Each day, after supervisors ascertained the number of CESs available to make home visits (ie, not assigned to schools, travelers, or other community-based activities), they prioritized activities in the following order: (1) initial investigation of case patients, (2) initial investigation of contacts, (3) case patients who missed daily symptom monitoring, and (4) contacts who missed daily symptom monitoring.
At the start of a workday, CESs used their work iPads and secure 2-factor authentication to log into the contact tracing database and plan their outreach to clients. CESs first attempted telephone calls if numbers were available and then made home visits to people who could not be reached by telephone. Once clients were reached, CESs completed the necessary data fields and made any referrals for supportive services from the Take Care team, who received those referrals in real time to fulfill the referrals. Through the community advisory board, we also identified periods of religious observance in which to pause or modify our operations.
Results
When the CES operation launched with 519 CESs and 50 supervisors on July 6, 2020, the CESs included 119 (23%) Hispanic or Latino, 212 (41%) Black, 131 (25%) White, 54 (10%) Asian/Pacific Islander, and 3 (1%) Native American people. Overall, 58% spoke ≥1 language in addition to English, including Spanish, French, Haitian Creole, Russian, Hebrew, Yiddish, Dutch, Bengali, Arabic, and Urdu.
CESs performed a range of activities during July 6–December 31, 2020 (Table), some of which were ongoing as of January 2022 (eg, contact tracing at home, point-of-care testing sites, outreach to private schools, New York City Department of Education Situation Room). The primary activity of CESs was home visits to people recently diagnosed with COVID-19 and their contacts. The first visit to elicit information about contacts or to notify contacts about exposures was categorized as initial investigation. CESs also provided information about safe isolation and quarantine practices and how to receive supportive services. Any subsequent interaction to assess symptoms and ascertain adherence to isolation or quarantine was categorized as monitoring.
COVID-19 contact tracing activities conducted by community engagement specialists (CESs) in New York City, 2020-2021
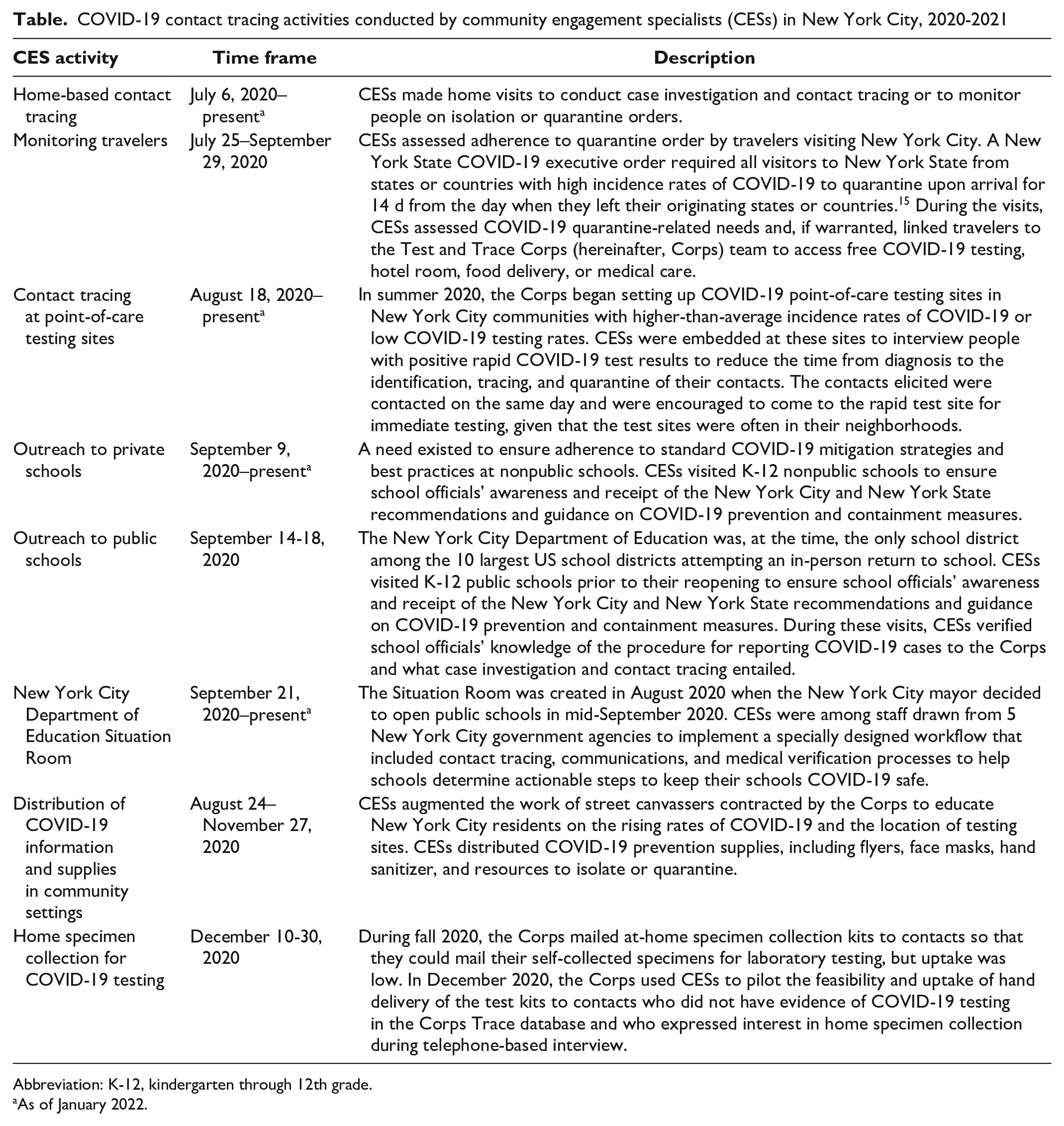
Abbreviation: K-12, kindergarten through 12th grade.
As of January 2022.
During July–December 2020, 7% (155 950 of 2 183 039) of records in the contact tracing database were referred to CESs. These records included 94 704 people with COVID-19 and 61 246 contacts not reached by telephone-based contact tracers. CESs attempted home visits or telephone calls with 84 230 people with COVID-19 and 49 303 contacts, reaching approximately 55 592 (66%) and 35 005 (71%), respectively.
Beginning in August 2020, CESs were also integrated into their neighborhood Corps point-of-care COVID-19 testing sites, which accelerated initial investigations for new case patients and their contacts. As businesses and schools reopened, CESs also frequently deployed to these settings to provide education about COVID-19 mitigation strategies, including case investigation and contact tracing, and to distribute information on free COVID-19 services.
Discussion
Door-to-door visits are a core contact tracing strategy to reach people who are unable or unwilling to respond to telephone calls and to deliver community-level disease prevention activities for other infectious diseases. 16 To our knowledge, our study is among the first to describe a large-scale mobilization of public health workers to perform in-person case investigation and contact tracing and COVID-19 prevention activities in community settings. In developing the CES workforce, we aimed to promote health equity and inclusion by recruiting staff with diverse backgrounds and language skills, providing standard training, instituting infection control and safety measures, procuring supplies and means of transportation, and developing protocols and algorithms to efficiently distribute the workload.
As in many public health jurisdictions, New York City initially conducted COVID-19 contact tracing primarily through a telephone-based operation,3-7 because this approach was safe, logistically less complicated, and more economical than traditional, in-person contact tracing. Some jurisdictions also incorporated smartphone-based digital technology, such as exposure notification applications.17-20 However, our experience in New York City demonstrates that not all people with COVID-19 and their contacts are accessible by telephone, thus curtailing the reach of an exclusively technology-based contact tracing operation. Furthermore, our effort to recruit a CES workforce with multilingual skills and diverse sociodemographic backgrounds similar to those of New Yorkers heavily impacted by COVID-19 arguably enhanced the delivery of services and linkage of clients to supportive services. 21
This study had at least 2 limitations. First, we did not report data showing the extent to which CES efforts directed toward clients who were not reached through telephone calls enhanced the yields of the overall Trace contact tracing program. A report on CES contributions to overall Trace outcomes is needed. Second, although cost analysis was beyond the scope of our study, our program relied on an established and well-resourced infrastructure and generous funding. Therefore, our methods are not generalizable to community-based contact tracing workforces that lack existing institutions and funds to support a relatively large number of personnel, equipment, supplies, and incentives for clients.
Practice Implications
We found value in establishing a community-based workforce to conduct in-person contact tracing and support other COVID-19 interventions to stem ongoing disease transmission. Our methods show the feasibility of implementing these services while protecting the health and safety of community health workers. With appropriate planning and support, in-person delivery of contact tracing and associated resources can supplement telephone-based efforts and enhance a health department’s reach and community impact.
Footnotes
Acknowledgements
The authors thank community engagement specialists and supervisors for their hard work and dedication; the many people at the New York City government agencies who provided operational support for this work; and Hannah Helmy, PhD, MPH, and Julian Watkins, MD, for substantive comments on the draft article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.