
Abstract
Objectives:
We evaluated 2 innovative approaches that supported COVID-19 case investigation and contact tracing (CI/CT) in Chicago communities: (1) early engagement of people diagnosed with COVID-19 by leveraging the existing Healthcare Alert Network to send automated telephone calls and text messages and (2) establishment of a network of on-site case investigators and contact tracers within partner health care facilities (HCFs) and community-based organizations (CBOs).
Methods:
The Chicago Department of Public Health used Healthcare Alert Network data to calculate the proportion of people with confirmed COVID-19 who successfully received an automated telephone call or text message during December 27, 2020–April 24, 2021. The department also used CI/CT data to calculate the proportion of cases successfully interviewed and named contacts successfully notified, as well as the time to successful case interview and to successful contact notification.
Results:
Of 67 882 people with COVID-19, 94.3% (n = 64 011) received an automated telephone call and 91.7% (n = 62 239) received a text message. Of the 65 470 COVID-19 cases pulled from CI/CT data, 24 450 (37.3%) interviews were completed, including 6212 (61.3%) of the 10 126 cases diagnosed in HCFs. The median time from testing to successful case interview was 3 days for Chicago Department of Public Health investigators and 4 days for HCF investigators. Overall, 34 083 contacts were named; 13 117 (38.5%) were successfully notified, including 9068 (36.6%) of the 24 761 contacts assigned to CBOs. The median time from contact elicitation to completed notification by CBOs was <24 hours.
Conclusions:
Partnerships with HCFs and CBOs helped deliver timely CI/CT during the COVID-19 pandemic, suggesting a potential benefit of engaging non–public health institutions in CI/CT for existing and emerging diseases.
Case investigation and contact tracing (CI/CT) are core public health strategies used to control and prevent the spread of disease. 1 The rapid rise in the number of people diagnosed with COVID-19 required public health departments to quickly scale up response efforts, including CI/CT. For some jurisdictions, this scaling up meant leveraging partnerships with other in-state health departments, universities, and private companies to assist with staffing and training, public health messaging, and technology support. 2
As a central component of its CI/CT response, the Chicago Department of Public Health (CDPH) established a health equity–focused, multisector COVID-19 CI/CT program, a novel approach that had not been previously implemented in Chicago. The program prioritized 3 overarching goals: disrupting SARS-CoV-2 transmission, promoting health equity and economic recovery in Chicago communities, and building a sustainable community-based public health workforce.
During March 1, 2020–April 24, 2021, a total of 273 454 COVID-19 cases were confirmed in Chicago. 3 During this time, Hispanic and non-Hispanic Black people composed 59% of diagnosed COVID-19 cases and 72% of deaths attributed to COVID-19. 3 Compared with non-Hispanic White people in Chicago, Hispanic and non-Hispanic Black people in Chicago had a higher prevalence of underlying chronic health conditions, such as obesity and diabetes, which can lead to severe COVID-19–related illness. 4 Hispanic and non-Hispanic Black people in Chicago also have institutional and systemic disparities that can precipitate poor health outcomes, including reduced access to resources (health, education), healthy environments (food security, safety), and wealth-generating opportunities (home ownership, stable employment). 4 Recognizing COVID-19 in this context, the CDPH CI/CT program took inspiration from Healthy Chicago 2025, the city’s public health improvement plan, which is grounded in health equity. 4
CDPH implemented a number of innovative approaches to CI/CT in Chicago. These included automated telephone calls and texts to people diagnosed with COVID-19 to provide self-isolation and support information, funding for partner health care facilities (HCFs) to provide on-site CI/CT to their patient populations, and partnering with community-based organizations (CBOs) to deliver contact notification to contacts elicited by CDPH case investigators.
While developing the partnerships for this unified response model, CDPH intentionally focused on organizations located in or serving communities that were experiencing high levels of economic hardship. The economic hardship index includes 6 indicators: crowded housing, poverty, unemployment, education, dependency, and income. Most HCFs are federally qualified health centers that provide primary care and other services in medically underserved areas. We funded the HCFs to implement CI/CT services for their patient populations and their named contacts. CDPH also prioritized contracting CBOs located in or serving communities experiencing high levels of economic hardship and asked CBOs to primarily hire residents from these same communities. Approximately 80% of HCF CI/CT employees and approximately 97% of CBO contact tracers were non-Hispanic Black people or other people of color (internal data, CDPH, COVID Response Bureau, 2021). Investing in these organizations and individuals ensured that residents in these communities were provided CI/CT services from local, trusted entities and that substantial financial resources were directed to areas of the city experiencing economic hardship and disproportionate COVID-19 morbidity and mortality. 3
CI/CT response to the COVID-19 pandemic across other US jurisdictions has varied.5-8 The literature primarily presents CI/CT programs implemented by public health departments that have not partnered with health care and community-based entities.9-14 We examined the success of this multisector CI/CT model grounded in health equity and the development of a stable, sustainable, diversified, and integrated public health workforce.
Methods
Case Reporting and Automated Notification of People With COVID-19
Illinois-based health care providers and testing facilities are required to report all probable and confirmed COVID-19 cases through the Illinois National Electronic Disease Surveillance System. Data on cases occurring in Chicago are then imported into CDPH’s Chicago CARES, a centralized database (Salesforce application) used by CDPH and funded partners.
Beginning on December 12, 2020, all people in Chicago who were reported as having a positive SARS-CoV-2 test result and who provided accurate contact information at the time of testing received an automated telephone call, text message, or both through the CDPH Healthcare Alert Network (HAN). These automated calls and text messages were sent daily, allowing CDPH to provide timely notification and guidance related to self-isolation and information about where to seek medical attention if severe symptoms developed. People were also linked to an online survey to request wraparound services (food, medications, housing, infection prevention supplies) to support self-isolation. These automated notifications occurred independently of the subsequent in-person CI/CT process. Using HAN data, the CDPH team tracked the number of telephone calls and text messages that were successfully received and calculated the proportion of people with confirmed COVID-19 who successfully received a telephone call or text message among the total number of people reported as having confirmed COVID-19.
Partnerships for CI/CT
CDPH partnered with HCFs and CBOs to develop a team of approximately 800 case investigators and contact tracers citywide. In August 2020, CDPH established a 2-year, $54-million contract with the Chicago Cook Workforce Partnership to manage the Resource Coordination Hub, which connected people with wraparound services, and to establish a network of 500 contact tracers and supervisors across 31 subcontracted CBOs (ie, nonclinical organizations located in or serving communities in Chicago with high economic hardship). Although the main function of the CBOs was to handle contact tracing, CBOs assisted with case investigation under some circumstances. CDPH also provided $14 million in funding to 19 Chicago-based federally qualified health centers, 8 hospitals, and 9 primary care clinics to implement CI/CT services for their patient populations. In addition to case investigations, these HCF-based CI/CT teams monitored symptoms, notified contacts, and either provided internal resource coordination services (eg, housing placement, medication assistance, mental health services) or referred people to the Resource Coordination Hub.
Analysis Datasets
CDPH’s Chicago CARES was the data source for CI/CT data analysis. Chicago CARES allows CDPH, HCFs, and CBOs to initiate and track case investigations, to create named contact records, and to notify contacts. The database records the institutional affiliation of each user (case investigator or contact tracer) who interacts with a case or contact record over time, allowing us to classify CI/CT staff by organization type (ie, CDPH, HCF, or CBO).
We extracted CI/CT data for cases with Chicago addresses and specimen collection dates recorded from December 27, 2020, through April 24, 2021 (ie, after the HCFs were integrated into CDPH CI/CT efforts in December 2020). For this CI/CT analysis, we used 2 datasets to calculate the proportion of completed case interviews and contact notifications and the timeliness of CI/CT work. The user information database classified each case investigator or contact tracer handling a record by organization type: CDPH, HCF, or CBO. The time point dataset included the various time points associated with the CI/CT workflow and outcomes. The 2 datasets were merged by a unique interaction identifier, allowing for comparisons of completeness and timeliness by organization type.
CI/CT Completeness Measures
Our primary performance measures were the proportions of (1) reported cases with successfully completed interviews and (2) named contacts with successfully completed notifications. We calculated these performance measures overall and by organization type. We divided the number of case records documented as having a successful, partially successful, or unsuccessful outcome by the total number of reported case records pulled from Chicago CARES. Similarly, we divided the number of contact records with each outcome by the total number of named contact records.
We defined case interviews and contact notifications that resulted in complete information for all required fields in the data collection instrument as a “successfully interviewed case” or a “successfully notified contact,” respectively. We classified incomplete case interviews and contact notifications with at least 1 section of the survey tool completed as “partially interviewed cases” or “partially notified contacts.” Several telephone call outcomes for partially interviewed cases/contacts or for cases/contacts not interviewed are documented in Chicago CARES. We invoked the “administratively closed” category after 3 unsuccessful call attempts (ie, left voicemails, reached a disconnected number, or scheduled a time to call back) or >4 days from specimen collection date during COVID-19 surge periods and after 5 unsuccessful call attempts or >7 days from specimen collection date during non–surge periods. Additional call outcomes documented in Chicago CARES include refusal to complete the interview/notification, deceased, or hospitalized. CI/CT staff members also documented people who were unreachable because of incorrect contact information.
CI/CT Timeliness Measures
To assess case investigation timeliness, we measured the median number of days from specimen collection date to date of a completed interview. To assess contact notification timeliness, we measured the median number of days from the case interview in which the contact was named (ie, contact record created) to successful contact notification. Public health surveillance data presented in this article did not require CDPH Institutional Review Board review.
Results
Of 67 882 confirmed COVID-19 cases reported to CDPH from December 27, 2020, through April 24, 2021, 94.3% (n = 64 011) received an automated telephone call from the Healthcare Alert Network, and 91.7% (n = 62 239) received a text message with diagnosis and self-isolation instructions from the Healthcare Alert Network. Call and text messages with no receipt confirmation were the result of incorrect contact information collected at the time of testing or individuals not answering a call or checking a text message from an unknown number. After the automated telephone calls and texts were made, case investigators attempted to interview 37 422 (57.2%) of 65 470 cases pulled from Chicago CARES, and contact tracers attempted to notify 22 240 (65.2%) of 34 083 named contacts (Figure). Because of technical difficulties, a subset of cases with specimen collection dates of February 14-20, 2021, were unable to be pulled from Chicago CARES, resulting in the lower number of cases in the CI/CT analysis than in the Healthcare Alert Network data.
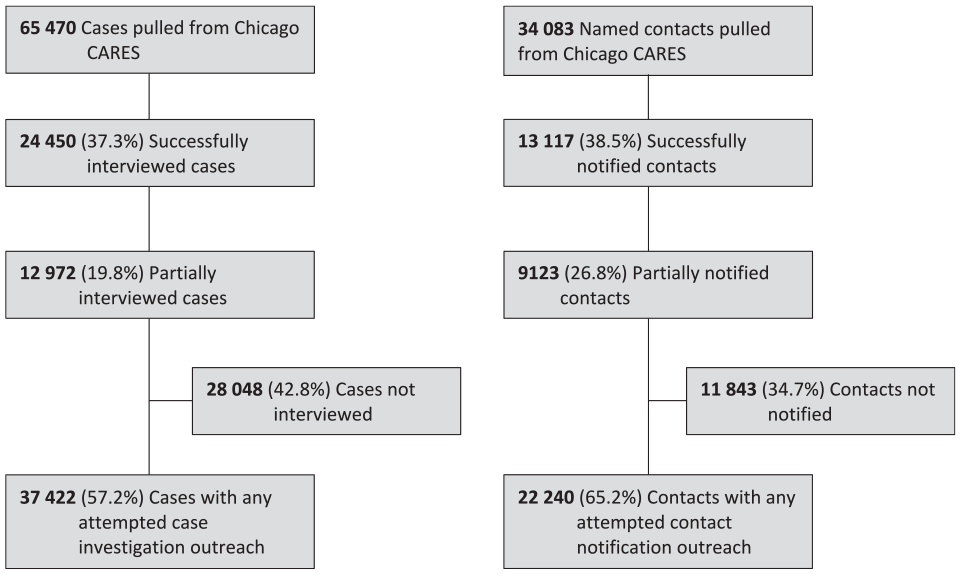
Case investigation and contact notification call outcomes during the COVID-19 pandemic, Chicago, December 27, 2020–April 24, 2021. Data source: Chicago CARES Salesforce case investigation and contact tracing (CI/CT) records. Because of technical difficulties, a subset of cases with specimen collection dates of February 14-20, 2021, was unable to be pulled from Chicago CARES and was excluded from analysis. This resulted in a lower number of cases pulled from Chicago CARES compared with the total number of cases present in the Healthcare Alert Network data. Cases that had responses to all required fields in the Salesforce case interview tool were classified as “successfully interviewed,” and contacts that had responses to all required fields in the Salesforce contact notification interview tool were classified as “successfully notified.” Cases and named contacts that completed only a portion of the Salesforce data collection tool were classified as “partially interviewed cases” or “partially notified contacts.” Cases and names that were administratively closed or that were unreachable because of incorrect contact information were classified as “cases not interviewed” or “contacts not notified.”
Overall, 37.3% (n = 24 450) of case investigations resulted in successfully interviewed cases and 19.8% (n = 12 972) in partially interviewed cases; 35.6% (n = 23 319) of cases were not interviewed because they were administratively closed; and 7.2% (n = 4729) of cases were unreachable because of incorrect contact information. HCFs managed 10 126 (15.5%) of 65 470 case investigations, successfully interviewing 61.3% (6212 of 10 126) of cases. CBO contact tracers successfully interviewed 65.7% (301 of 458) of their assigned cases. In comparison, CDPH staff successfully interviewed 32.7% (17 932 of 54 804) of their assigned cases (Table).
Completeness and timeliness measures of Chicago CARES Salesforce CI/CT during the COVID-19 pandemic, by organization type, Chicago, December 27, 2020–April 24, 2021 a
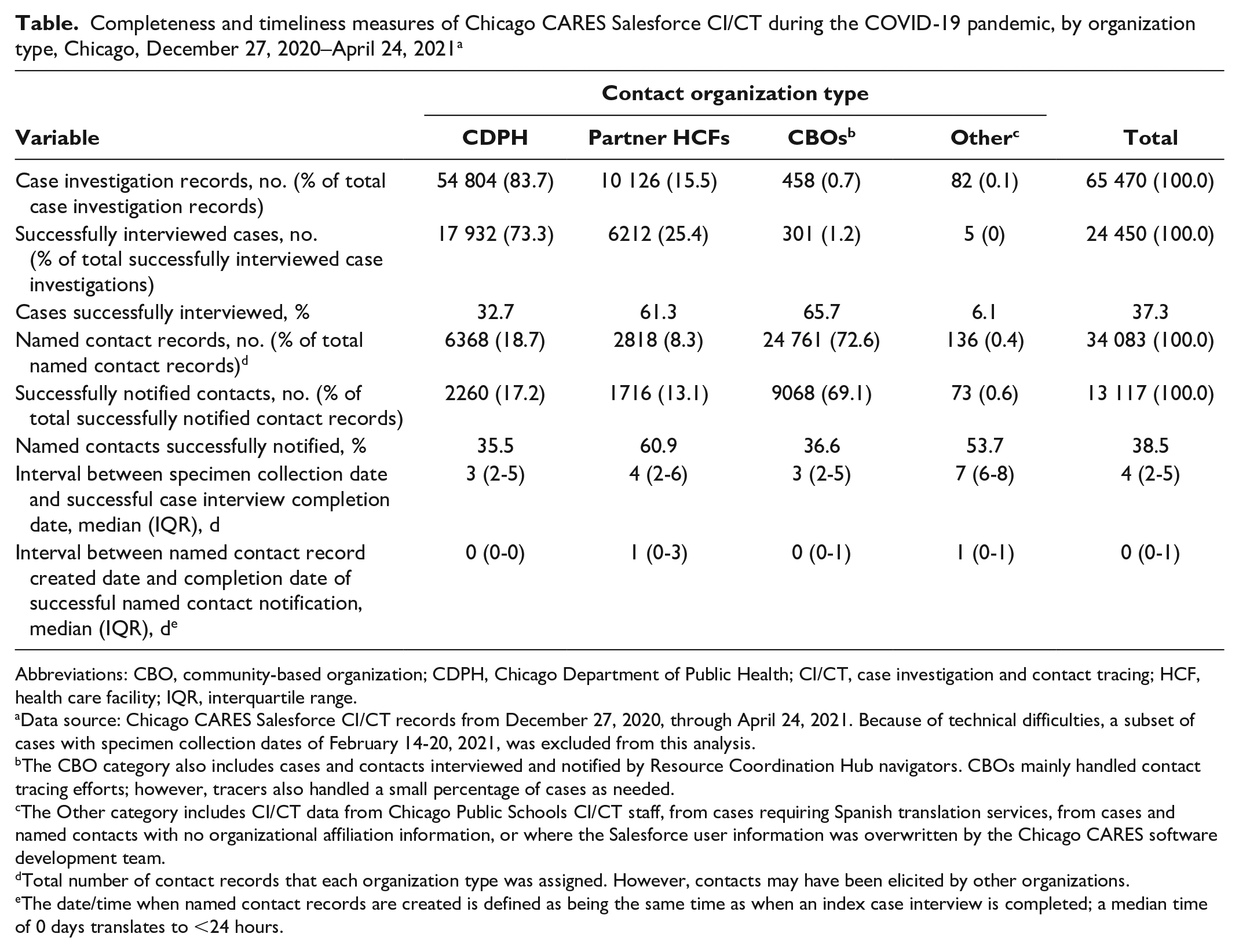
Abbreviations: CBO, community-based organization; CDPH, Chicago Department of Public Health; CI/CT, case investigation and contact tracing; HCF, health care facility; IQR, interquartile range.
Data source: Chicago CARES Salesforce CI/CT records from December 27, 2020, through April 24, 2021. Because of technical difficulties, a subset of cases with specimen collection dates of February 14-20, 2021, was excluded from this analysis.
The CBO category also includes cases and contacts interviewed and notified by Resource Coordination Hub navigators. CBOs mainly handled contact tracing efforts; however, tracers also handled a small percentage of cases as needed.
The Other category includes CI/CT data from Chicago Public Schools CI/CT staff, from cases requiring Spanish translation services, from cases and named contacts with no organizational affiliation information, or where the Salesforce user information was overwritten by the Chicago CARES software development team.
Total number of contact records that each organization type was assigned. However, contacts may have been elicited by other organizations.
The date/time when named contact records are created is defined as being the same time as when an index case interview is completed; a median time of 0 days translates to <24 hours.
CDPH, HCFs, and CBOs successfully notified 35.5%, 60.9%, and 36.6% of the named contacts assigned to their workflows, respectively. Of the 34 083 named contacts in Chicago during these 4 months, 38.5% (n = 13 117) were successfully notified, 26.8% (n = 9123) were partially notified, 18.9% (n = 6437) were not notified because they were administratively closed, and 15.9% (n = 5406) were unreachable because of incorrect contact information.
In January 2021, case interview timeliness was approximately the same for all 3 organization types (ie, median of 4-6 days after specimen collection). By the end of March 2021 and consistently through the end of April 2021, HCF case interviews occurred a median 3 of days after specimen collection, while CDPH case interviews continued to occur a median of 4-5 days later. By mid-January 2021, the median time after interview (ie, contact record creation) to successful contact notification was consistently ≤24 hours across all organization types.
Discussion
CI/CT Completeness
Just before the early 2021 COVID-19 case surge in Chicago, CDPH expanded public health capacity for CI/CT by partnering with HCFs and CBOs to deliver CI/CT and to provide related support services. HCFs performed demonstrably better than CDPH in case investigations (61.3% vs 32.7% successfully interviewed) and CBOs in contact notification (60.9% vs 36.6% successfully notified), suggesting that CI/CT delivered through diagnosing HCFs can be an effective strategy to supplement CI/CT delivered through traditional public health departments. In addition, automated systems put in place by CDPH ensured that >90% of people in Chicago reported as having a positive SARS-CoV-2 test result received an automated telephone call or text message with guidance on self-isolation and links to wraparound services to support successful isolation, even before in-person CI/CT efforts reached them. Automated engagement of diagnosed people increased the percentage of people provided with public health guidance and access to needed resources and allowed for timely outreach, even during surge periods, which can lead to a backlog of case interviews for CI/CT staff. These innovative CI/CT systems remain in place.
Overall, our 37.3% successful case interview and 38.5% successful contact notification performance measures are lower than published measures from other jurisdictions at earlier time points.9-11 Possible reasons for the lower success rates include the period of this assessment, the COVID-19 surge experienced during this period, the timing of HCF integration into the overall Chicago CI/CT effort, and reassignment of some CDPH CI/CT staff to work on vaccine distribution starting in December 2020, which reduced the CI/CT workforce in early 2021.
These proportions do not fully describe the performance of our CI/CT response. In fact, 57.2% (n = 24 450 successful interviews and n = 12 972 partial interviews) of cases pulled from Chicago CARES (n = 65 470) and 65.2% (n = 13 117 successful notifications and n = 9123 partial notifications) of named contacts (n = 34 083) had some degree of engagement with CI/CT staff.
CI/CT Timeliness
Effective disruption of SARS-CoV-2 transmission requires completing case interviews and contact notifications in a timely manner. Our timeliness measures were similar to measures previously reported and initially similar between CDPH and its HCF and CBO partners. 10 However, after 3 months, the timeliness of HCF case interviews surpassed that of CDPH case interviews (3 vs 4-5 days).
Unanticipated Return on Investment
CDPH initially invested in HCFs and CBOs to supplement its CI/CT response. Beyond this scope of work, HCFs routinely provided additional services, including care coordination and navigation, to people diagnosed with or exposed to SARS-CoV-2. As a result of their participation in CI/CT, many HCFs are interested in adapting their CI/CT workflows to managing other infectious diseases, including HIV.
Like HCFs, CBO contract tracers worked beyond their initial scope. Teams of contact tracers—most of whom reside in community areas experiencing high levels of economic hardship and disproportionate COVID-19 morbidity and mortality—staff Chicago’s citywide vaccination call center. As of February 2022, the call center had managed >350 000 in-bound calls and >95 000 outbound calls (internal data, CDPH, COVID Response Bureau, 2021). Contact tracers also provided door-to-door community engagement to >19 000 homes to promote vaccine uptake in Chicago’s most affected community areas (internal data, CDPH, COVID Response Bureau, 2021).
Limitations
Our CI/CT program had several implementation challenges, consistent with the findings of articles on other US contact tracing programs.15,16 First, the time and resources needed to train HCF case investigators and CBO contact tracers were important but might have resulted in missed opportunities for timely CI/CT during the initial part of the analysis period. Second, while the number of COVID-19 cases was increasing, CI/CT program staff at the various organizations were conducting investigations and recording data while the Chicago CARES database was still being developed and modified. Third, CDPH CI/CT program managers had to focus on solving technical issues that arose with HCF and CBO integration into the Chicago CARES system, which hindered internal CDPH CI/CT efforts. Finally, when comparing performance measures across organization types, one should take into account that CI/CT baseline knowledge, public health experience, and training varied across and within the organization types. Specifically, CDPH staff had established experience in COVID-19 CI/CT work before December 2020, when HCFs and CBOs were still training new CI/CT staff.
Conclusions
HCF and CBO case investigators and contact tracers performed at least as well as their CDPH-based counterparts in executing timely and complete interviews and notifications. These data suggest that HCFs and CBOs can successfully supplement core public health functions, such as CI/CT. Additionally, HCF and CBO workforces can augment other needed public health responses, creating unanticipated returns on investment. Furthermore, by hiring and training individuals who reside in communities with high levels of economic hardship, public health investments can assist in economic recovery and build a foundation for a coordinated and sustainable community-based public health workforce for the future. Our health-equity approach to a public health threat can serve as a model for other public health responses in Chicago and beyond.
Footnotes
Acknowledgements
The authors thank Melanie Taylor, MD, MPH, and Dawn Broussard, DrPH, for encouraging us to describe our experience and submit an article for this supplemental issue, and Ashley Becht, MPH, and Carla Barrios for providing clarification on certain CI/CT protocols.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.