
Abstract
Objectives:
Financial hardships, job losses, and social isolation during the COVID-19 pandemic have increased food insecurity. We examined associations between food insecurity–related interventions and mental health among US adults aged ≥18 years from April 2020 through August 2021.
Methods:
We pooled data from the Household Pulse Survey from April 2020 through August 2021 (N = 2 253 567 adults). To estimate associations between mental health and food insecurity, we examined the following interventions: the Supplemental Nutrition Assistance Program (SNAP), Economic Impact Payments (stimulus funds), unemployment insurance, and free meals. We calculated psychological distress index (PDI) scores (Cronbach α = 0.91) through principal components analysis using 4 mental health variables: depression, anxiety, worry, and lack of interest (with a standardized mean score [SD] = 100 [20]). We conducted multivariable linear regression to estimate the interactive effects of the intervention and food insecurity on psychological distress, controlling for sociodemographic characteristics.
Results:
During the study period, adults with food insecurity had higher mean PDI scores than adults without food insecurity. Food insecurity was associated with increased PDI scores after controlling for sociodemographic characteristics. In stratified models, negative associations between food insecurity and mental health (as shown by reductions in PDI scores) were mitigated by SNAP (−4.5), stimulus fund (−4.1), unemployment insurance (−4.4), and free meal (−4.4) interventions. The mitigation effects of interventions on PDI were greater for non-Hispanic White adults than for non-Hispanic Black or Asian adults.
Conclusions:
Future research on food insecurity and mental health should include investigations on programs and policies that could be of most benefit to racial and ethnic minority groups.
Since the COVID-19 pandemic began in early 2020, the US unemployment rate peaked at 14.8% in April 2020 and declined to 5.2% in August 2021, still remaining above the level prior to the pandemic. 1 Moreover, more than 108 million or 55.5% of US adults experienced household income loss from March 2020 through December 2020. 2 The economic recession during the pandemic has increased food insecurity, meaning the inability of households to acquire adequate food because of insufficient resources for food.3-6 As reported in 2019, food insecurity rates were higher among non-Hispanic Black (19.1%) and Hispanic (15.6%) people than among non-Hispanic White people (7.9%). 4 In 2020, the estimated food insecurity rate for the overall US population was 13.9% (ie, approximately 45 million people), which was higher than the rate of 10.5% to 10.9% in the US population in 2019.4,7
Food insecurity during the pandemic, in conjunction with job and income losses and a stressed health care system, has had a negative effect on people’s physical and mental health.6,8-10 African American adults (59.4%), Hispanic adults (60.2%), and adults of other or multiple races (58.0%) were more likely than non-Hispanic White adults (53.3%) to experience job-related income losses in 2020. 2 Adults in racial and ethnic minority groups were more likely than non-Hispanic White adults to experience depression or anxiety,11-16 which might have resulted from disproportionately higher job loss, mortality, or racism and anti-Asian sentiment during the pandemic.2,17-19 One study found a higher increase in anxiety disorders during the pandemic among non-Hispanic Black, Hispanic, and Asian adults than among non-Hispanic White adults, with Asian adults showing the largest increase in anxiety disorders. 19 US adults with greater food insecurity were more likely than adults with food security to feel anxious, worried, or depressed or show little interest in participating in activities.9,20,21
After the start of the COVID-19 pandemic, both existing and new government programs and private responses addressed food insecurity for the overall population. The Supplemental Nutrition Assistance Program (SNAP) provides benefits to families in need of supplementary funds for their food budget. 22 Most households with incomes below a certain threshold are categorically eligible for SNAP, although the gross income limit varies across states, ranging from 130% to 200% of federal poverty guidelines as of July 2019. 23 Since the pandemic began, under the Families First Coronavirus Response Act, which was passed in March 2020, SNAP payments were raised to the maximum benefit level, a $165 increase in monthly benefits. 24 The number of people participating in SNAP increased from 39.9 million in fiscal year 2020 to 41.5 million in fiscal year 2021. 25 Government spending on SNAP benefits also increased, from $7.6 billion to $9.6 billion, during the same period. 25 In April 2021, average monthly benefits were $227 per person and $433 per household. 25 A previous study found that the additional SNAP benefit during the pandemic reduced food insecurity and that recipients of existing SNAP benefits were more likely than recipients of the additional SNAP benefits to have experienced food insecurity. 26
The distribution of economic impact payments in 2020 and 2021 may have helped to address food insecurity during the COVID-19 pandemic. In the first round of payments, as authorized by the Coronavirus Aid, Relief, and Economic Security (CARES) Act in March 2020, individuals received up to $1200, with $500 for each qualifying child aged <17 years.27,28 In the second round, as authorized by the 2021 Coronavirus Response and Relief Supplemental Appropriations Act in December 2020, individuals received $600, with $600 also provided to each qualifying child aged <17 years.27,29 Payments in the third round were up to $1400 per individual and $1400 for each qualifying dependent of any age, as authorized by the American Rescue Plan of 2021 in March 2021.27,30 One study found that receipt of stimulus funds was associated with a decrease in food insecurity only among non-Hispanic White adults but not among non-Hispanic Black and Hispanic adults. 26
Receipt of unemployment insurance could also alleviate food insecurity. As a joint state–federal program, unemployment insurance provides eligible unemployed workers with cash benefits for a maximum of 26 weeks in most states. 31 Generally, benefits are based on a percentage of an individual’s earnings during a recent 52-week period up to a state maximum amount. 31 Under the CARES Act, which was passed in March 2020, unemployment insurance was expanded to include a $600 per week supplement to weekly state unemployment benefits until August 2021, a 13-week extension of benefits, with expanded eligibility requirements.24,32,33 Total unemployment benefits paid were $22.1 billion in June 2020, which decreased to $3.98 billion in June 2021. 34 Unemployed adults who received the unemployment insurance benefit from April through November 2020 had a 4.3% decrease in food insecurity. 32 Adults with job or income loss who received the unemployment insurance from March through May 2020 also reported a decrease in worries about meeting basic needs. 35
Free meals, which also address food insecurity, are provided by charitable food providers, including food pantries, food banks, nongovernmental organizations, and churches.36,37 Feeding America, which directs the largest network of US food banks and food rescue organizations, distributed 6.1 billion meals during 2020, a 44% increase from 2019. 38 In May 2020, the US Department of Agriculture (USDA) launched the Farmers to Families Food Box program, in which the USDA purchased produce, dairy, and meats from farmers and delivered 173.6 million food boxes to families negatively affected by the COVID-19 pandemic. 39
Given that food insecurity negatively affects mental health and that public and private interventions reduce food insecurity, 3 we investigated the interactive effects of food insecurity–related interventions on mental health. Specifically, we examined the association between 4 food insecurity–related interventions (SNAP, stimulus funds, unemployment insurance, and free meals) and their effects on the mental health of US adults aged ≥18 years during the COVID-19 pandemic.
Methods
Data
We obtained data from the Household Pulse Survey (HPS), a nationally representative online survey developed by the US Census Bureau in cooperation with 13 other federal agencies to measure the impact of COVID-19 on US households.40,41 The HPS includes various measures, such as food security, physical and mental health, access to health care, housing, employment status, spending patterns, and educational disruption. 40 The HPS has a short turnaround time. In phase 1 of the HPS, surveys were conducted weekly with 3 rounds of interviews for the same household. In phase 2 and phase 3.2, surveys were conducted biweekly in cross-sectional datasets of the HPS. 40 For this study, we pooled HPS data from April 2020 through August 2021 that were available at the time of this study (N = 2 253 567). Institutional review board approval was not required for this study, which was based on the secondary analysis of a public-use survey database.
Sample
The study sample comprised adults aged ≥18 years who participated in the HPS from April 2020 through August 2021 (survey wave: week 1 through week 35). The final sample size varied by the intervention measures, ranging from 344 510 to 2 253 567 because of restrictions and data availability, although the pooled sample size was 2 882 158. We eliminated the repeated cases (interviews) from phase 1 for the same individual (an average 23.5% of the sample) for each survey week from weeks 1 through 12 (April 2020 through July 2020). We created missing covariate categories to prevent listwise deletion of many observations from the analysis for annual household income (7.9%), housing tenure (3.2%), marital status (0.5%), employment status (0.1%), and health insurance status (1.8%).
Outcome Measurement
We used a composite psychological distress index (PDI) measure as the dependent variable. We created a continuous variable of the composite PDI, given that interaction effects in nonlinear models cannot be straightforward, including the magnitude of the interaction effect, its sign, and its significance. 42 For this study, we constructed the composite PDI from the principal components analysis of 4 mental health variables available in HPS, which were gathered from the Patient Health Questionnaire-2 43 (having little interest and feeling down) and the Generalized Anxiety Disorder-2 44 (feeling anxious and worrying), based on previous studies.15,45,46 For these questionnaires in the HPS, respondents had been asked to review how often, during the last 7 days, they experienced (1) having little interest or pleasure in doing things; (2) feeling down, depressed, or hopeless; (3) feeling nervous, anxious, or on edge; and (4) an inability to stop or control worrying. For each of these 4 symptoms of mental health status, we used a 4-category ordinal scale, where 1 = not at all, 2 = several days, 3 = more than half the days, and 4 = nearly every day. Principal components analysis yielded the following factor loadings (ie, relative weights) for the PDI items: 0.870 for no interest, 0.885 for anxiety, 0.899 for depression, and 0.902 for worry, indicating high correlations of the items with the PDI. We found that the PDI had a high reliability coefficient (Cronbach α = 0.91), and the proportion of total variance explained by the factor was 0.79. We constructed PDI as a standardized index through principal components analysis to have a mean score of 100 and an SD of 20. Higher scores on the PDI indicated higher levels of psychological distress.
Food Insecurity
We defined food insecurity as the response to whether their household had enough food to eat in the last 7 days, with 1 indicating sometimes or often not enough food to eat and 0 indicating enough or enough but not always enough to eat.
Intervention
We gathered information on the 4 intervention variables related to food insecurity (SNAP, stimulus funds, unemployment insurance, or free meals) from responses in the HPS. Respondents were asked whether anyone in the household received (1) SNAP or food stamp program benefits, (2) a stimulus payment (ie, a COVID-19–related Economic Impact Payment from the federal government in the last 7 days), (3) unemployment insurance benefits since March 13, 2020, or (4) free groceries or a free meal during the last 7 days. Data on intervention variables were not available during the full 35-week period, April 2020 through August 2021, except for free meals. SNAP responses were available from weeks 13 through 35 (August 2020 through August 2021), and stimulus fund responses were available from weeks 7 through 12 (June 2020 through July 2020) and weeks 22 through 33 (January 2021 through July 2021). We used weeks 28 through 33 (April 2021 through July 2021) for unemployment insurance because of data availability and missing values.
Covariates
Based on previous literature and data availability, we selected the following covariates for model estimation: age, sex, race and ethnicity, education, annual household income, total number of people in household, marital status, employment status, health insurance, housing tenure, and state and week of data-fixed effects.47-50
Analytic Approach
We used multivariable linear regression to estimate the interactive effects of intervention and food insecurity on mental health, controlling for age, sex, race and ethnicity, education, annual household income, household size, marital status, housing tenure, employment status, health insurance, and state and weekly fixed effects. Interaction terms between food insecurity and each intervention (SNAP, stimulus fund, unemployment insurance, or free meals) were used to separately estimate the association between mental health and each intervention. We also estimated the differential effect by race and ethnicity and tested significance by using a Hausman test after the seemingly unrelated estimation (suest) to combine estimations from all subgroups to be pooled together. 51 We used complex survey design procedures to account for nonresponse, occupancy of the housing unit counts (person or group of people living in the unit at the time of the interview), the number of adults in the housing unit, and disproportionate sampling of demographic characteristics. 40 We adjusted sample weights by dividing by the number of pooling weeks (35 weeks). For all analyses, we used Stata version 17 (StataCorp LLC).
Results
From April 2020 through August 2021, the mean PDI score was higher among adults with food insecurity (119.5) than among those without food insecurity (99.8) (Table 1). Younger adults; adults with large household size; women; adults with less than high school, high school, or some college education; adults with annual household income <$25 000; divorced or separated adults or never-married adults; renters; unemployed adults; and uninsured adults had higher levels of food insecurity than their counterfactual groups. A higher percentage of non-Hispanic Black adults (18.9%), Hispanic adults (17.3%), and non-Hispanic adults of other race (16.3%) experienced food insecurity than non-Hispanic White (7.2%) or non-Hispanic Asian (5.8%) adults. Differences between characteristics in the food security and food insecurity group were significant at P < .001, using the Pearson χ2 test.
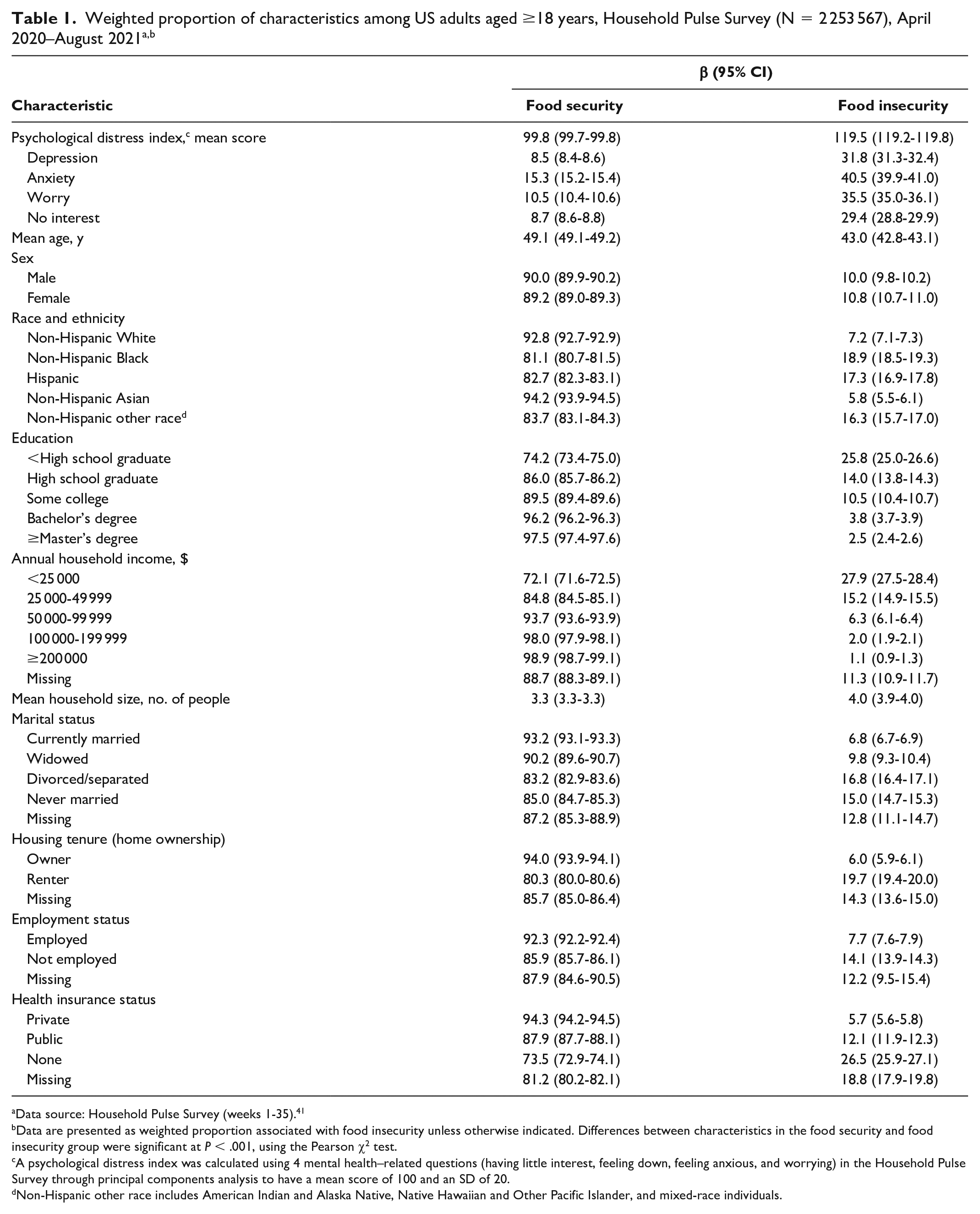
Data source: Household Pulse Survey (weeks 1-35). 41
bData are presented as weighted proportion associated with food insecurity unless otherwise indicated. Differences between characteristics in the food security and food insecurity group were significant at P < .001, using the Pearson χ2 test.
A psychological distress index was calculated using 4 mental health–related questions (having little interest, feeling down, feeling anxious, and worrying) in the Household Pulse Survey through principal components analysis to have a mean score of 100 and an SD of 20.
Non-Hispanic other race includes American Indian and Alaska Native, Native Hawaiian and Other Pacific Islander, and mixed-race individuals.
The food insecurity rate fluctuated but increased until July 2020 (12.5%), then decreased in August 2020 (10.1%), increased until December 2020 (13.5%), and displayed a decreasing trend in 2021 (Figure A). Similarly, the mean PDI score increased until July 2020 (104.8), decreased in August 2020 (101.5), increased until December 2020 (105.0), and decreased in 2021 (Figure B). The correlation between the 2 trends was 0.84 (P < .001).
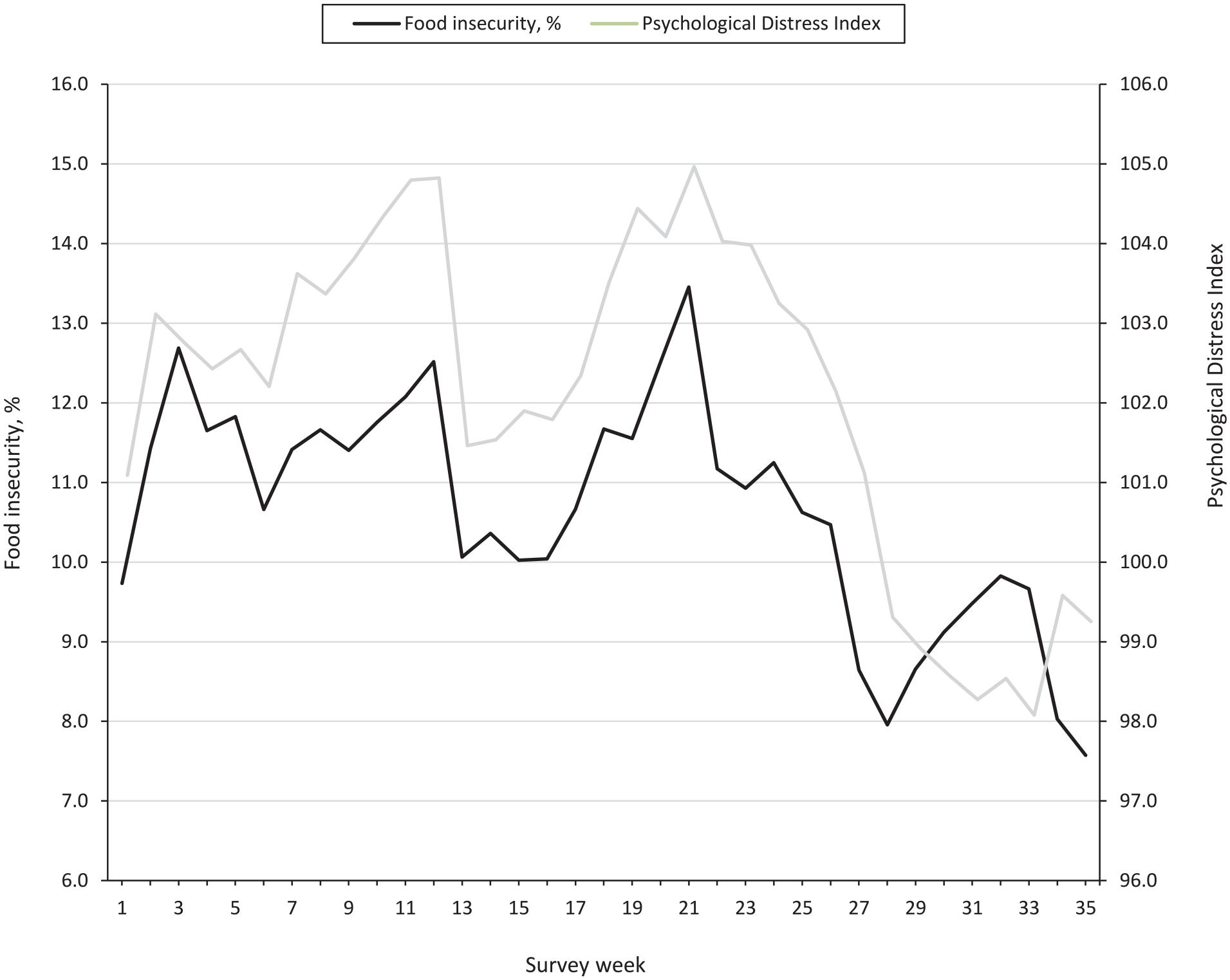
Trends in weighted prevalence of food insecurity and mean psychological distress index score during the COVID-19 pandemic among US adults aged ≥18 years, Household Pulse Survey (N = 2 253 567), April 2020–August 2021.
Association Between Food-Related Interventions and Mental Health
Food insecurity was associated with an increase of 16.0 to 17.5 points in mean PDI scores after controlling for sociodemographic characteristics in the absence of interventions (Table 2). In Model 1, food insecurity was associated with a 16.9-point increase in PDI after controlling for sociodemographic characteristics in the absence of interventions. Respondents who received SNAP had a 4.5-point reduced food insecurity–related psychological distress score. In Model 2, receiving stimulus funds mitigated the effect of food insecurity on psychological distress by 4.1 points. In Model 3, receiving unemployment insurance mitigated the effect of food insecurity on psychological distress by 4.4 points. In Model 4, receiving free meals reduced the effect of food insecurity on psychological distress by 4.4 points.
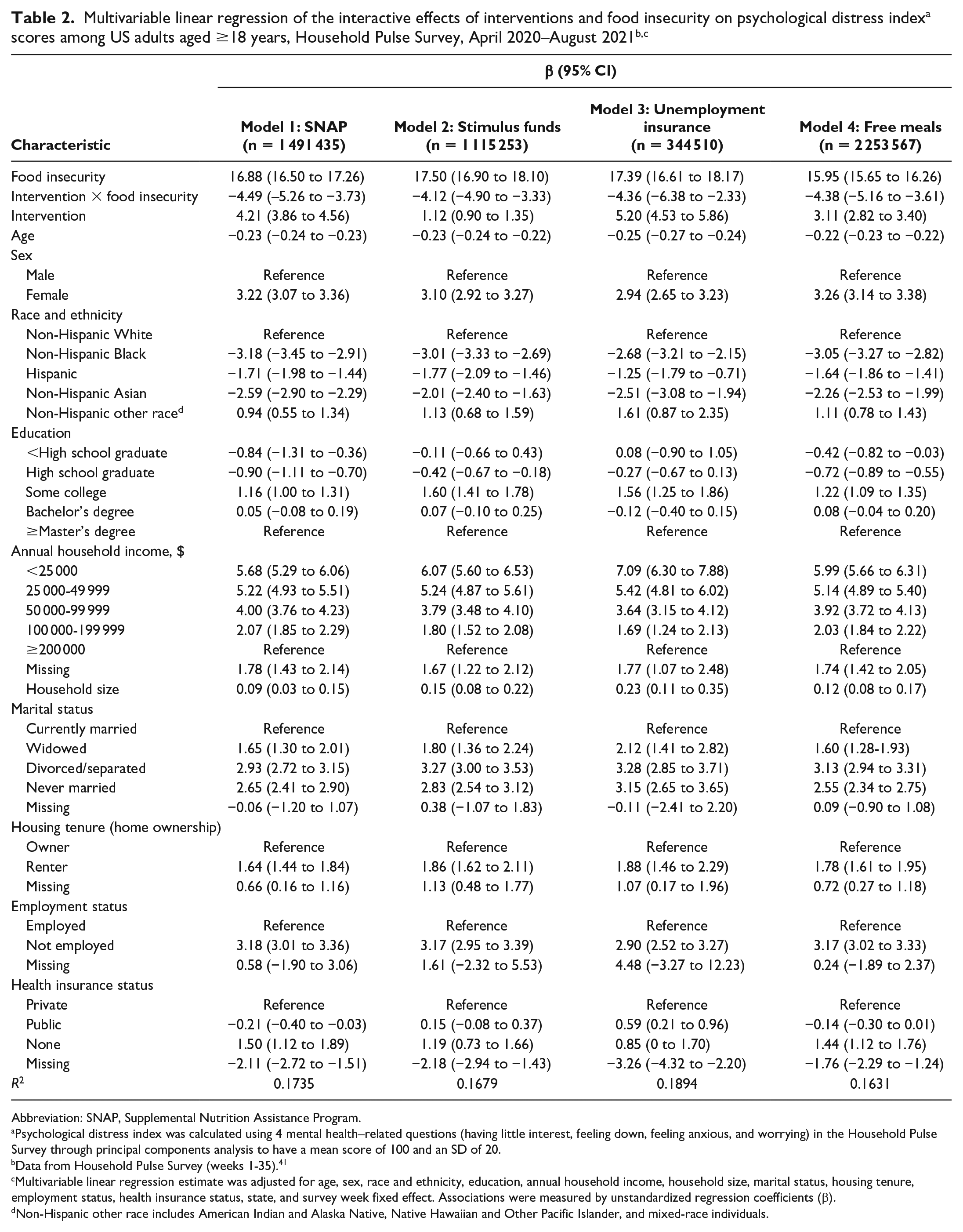
Abbreviation: SNAP, Supplemental Nutrition Assistance Program.
Psychological distress index was calculated using 4 mental health–related questions (having little interest, feeling down, feeling anxious, and worrying) in the Household Pulse Survey through principal components analysis to have a mean score of 100 and an SD of 20.
Data from Household Pulse Survey (weeks 1-35). 41
Multivariable linear regression estimate was adjusted for age, sex, race and ethnicity, education, annual household income, household size, marital status, housing tenure, employment status, health insurance status, state, and survey week fixed effect. Associations were measured by unstandardized regression coefficients (β).
Non-Hispanic other race includes American Indian and Alaska Native, Native Hawaiian and Other Pacific Islander, and mixed-race individuals.
Among non-Hispanic White adults, all 4 interventions reduced the effects of food insecurity on psychological distress; the food insecurity–related baseline in PDI scores ranged from 17.7 to 20.1 points before the interventions (Table 3). Among non-Hispanic White adults, receiving unemployment insurance and SNAP mitigated the effects of food insecurity on psychological distress by 6.8 and 6.1 points, respectively. Food insecurity greatly affected non-Hispanic Black adults, who had food insecurity–related changes in PDI scores that ranged from 13.4 to 14.9. Among non-Hispanic Black adults, receiving stimulus funds, free meals, and SNAP reduced the effects of food insecurity on psychological distress by 2.9, 2.3, and 1.8 points, respectively. The interactive effects of unemployment insurance were not significant among racial and ethnic minority groups. Hispanic adults were also greatly affected by food insecurity, with food insecurity–related changes in PDI scores that ranged from 14.5 to 15.4. Psychological distress scores among Hispanic adults were mitigated by receiving free meals, stimulus funds, and SNAP by 4.2, 3.3, and 2.6 points, respectively. Among non-Hispanic Asian adults, changes in food insecurity–related psychological distress scores ranged from 13.5 to 15.0. However, among non-Hispanic Asian adults, none of the 4 interventions greatly reduced the food insecurity–related psychological distress scores. Among non-Hispanic adults of other races, receiving SNAP, stimulus funds, and unemployment insurance reduced the negative effects of food insecurity on psychological distress scores by 5.1, 4.7, and 6.1 points, respectively.
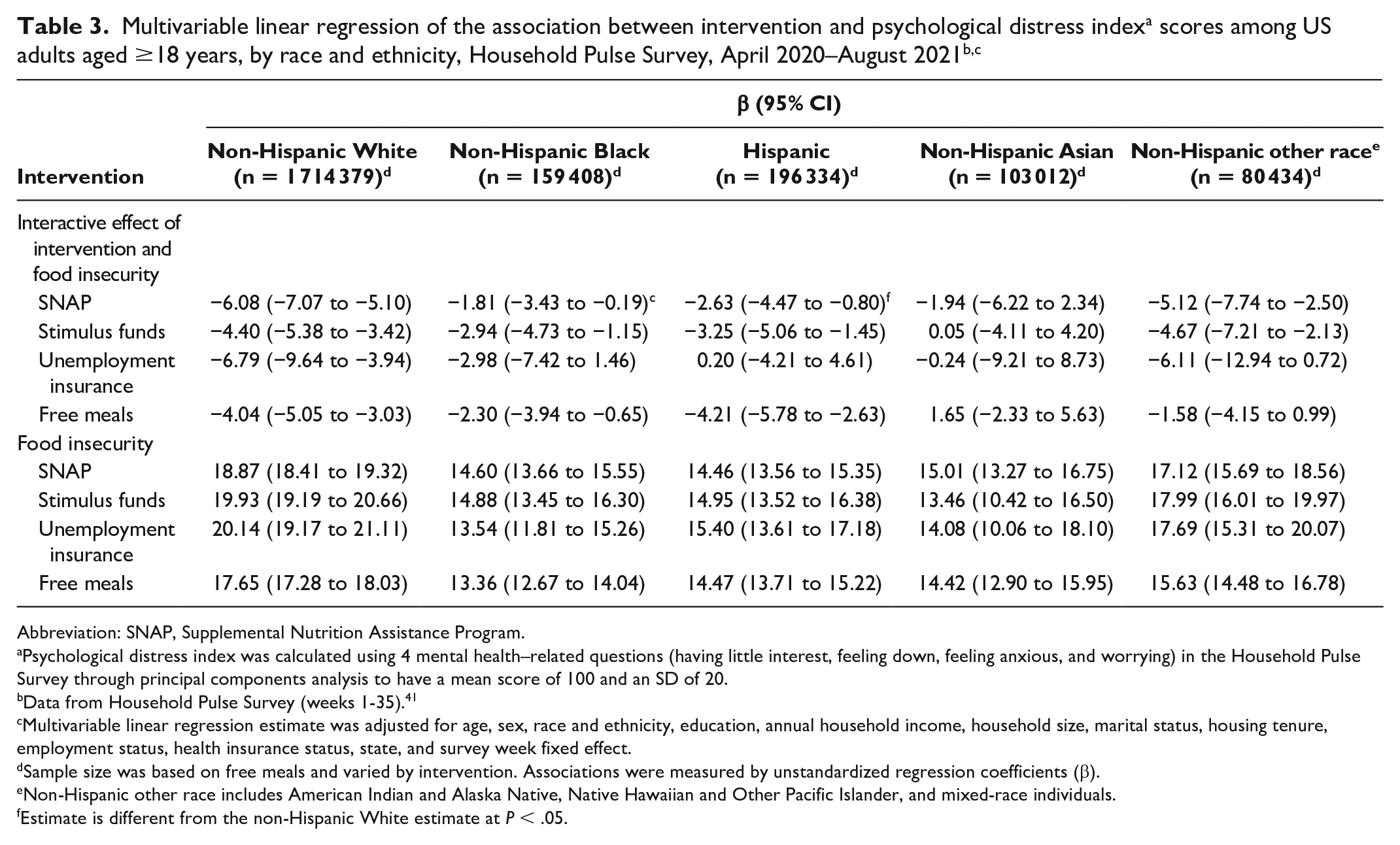
Abbreviation: SNAP, Supplemental Nutrition Assistance Program.
Psychological distress index was calculated using 4 mental health–related questions (having little interest, feeling down, feeling anxious, and worrying) in the Household Pulse Survey through principal components analysis to have a mean score of 100 and an SD of 20.
Data from Household Pulse Survey (weeks 1-35). 41
Multivariable linear regression estimate was adjusted for age, sex, race and ethnicity, education, annual household income, household size, marital status, housing tenure, employment status, health insurance status, state, and survey week fixed effect.
Sample size was based on free meals and varied by intervention. Associations were measured by unstandardized regression coefficients (β).
Non-Hispanic other race includes American Indian and Alaska Native, Native Hawaiian and Other Pacific Islander, and mixed-race individuals.
Estimate is different from the non-Hispanic White estimate at P < .05.
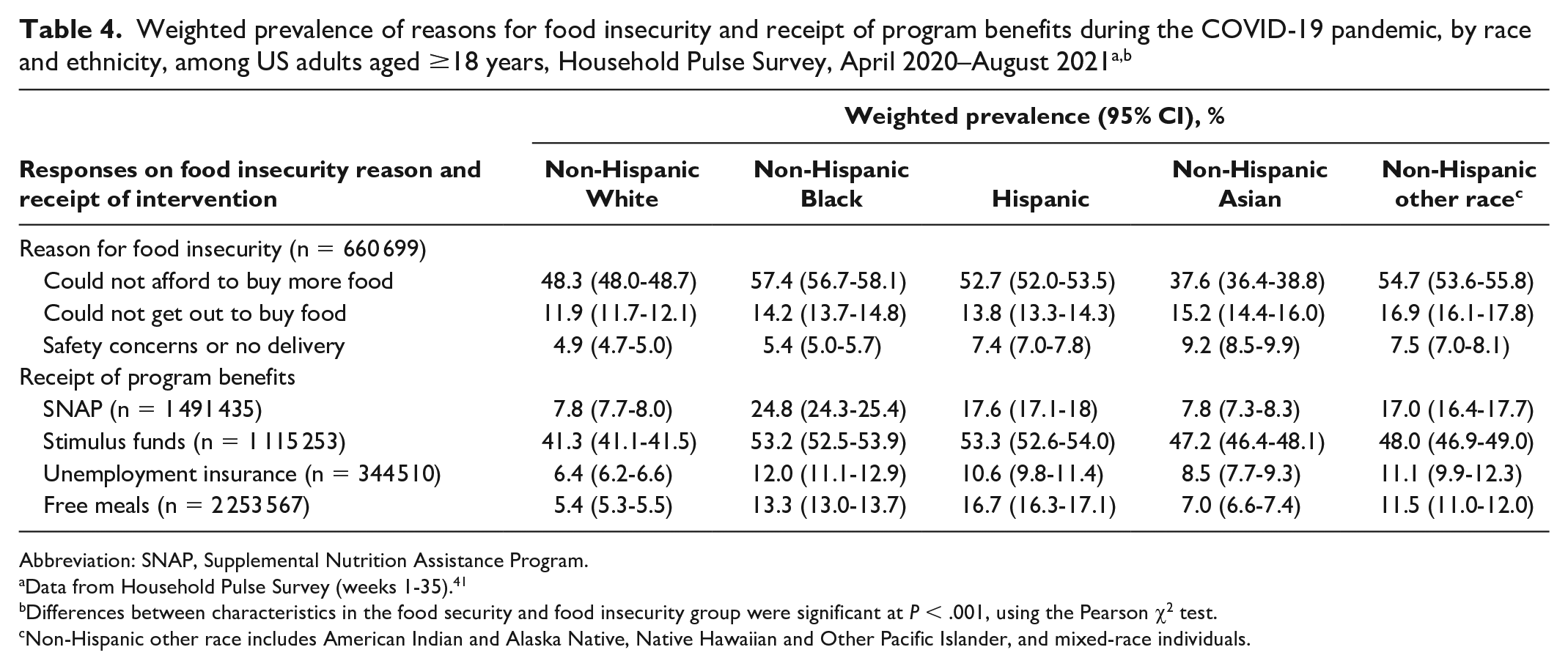
The most common reason for food insecurity was not being able to afford to buy more food for all racial and ethnic groups, and the inability to get out to buy food and safety concerns or no delivery were also cited as reasons for food insecurity (Table 4). The percentage of adults who reported that their food insecurity came from their inability to afford to buy food was higher among non-Hispanic Black (57.4%) than among non-Hispanic White (48.3%), Hispanic (52.7%), non-Hispanic Asian (37.6%), and non-Hispanic other race (54.7%) adults. A higher percentage of non-Hispanic Black and Hispanic adults than non-Hispanic White or non-Hispanic Asian adults received SNAP, stimulus funds, unemployment insurance, and free meals.
Abbreviation: SNAP, Supplemental Nutrition Assistance Program.
Data from Household Pulse Survey (weeks 1-35). 41
Differences between characteristics in the food security and food insecurity group were significant at P < .001, using the Pearson χ2 test.
Non-Hispanic other race includes American Indian and Alaska Native, Native Hawaiian and Other Pacific Islander, and mixed-race individuals.
Discussion
This study adds to the growing literature on the association between food insecurity and mental health during the COVID-19 pandemic6,8,9,20,21 and on the relationship between public or private interventions and food insecurity.32,37 Specifically, this study contributed to the existing literature by estimating the interactive effect of various interventions on the association between food insecurity and mental health as measured by a composite PDI that used data pooled from a nationally representative survey (HPS) that covered a pandemic period from April 2020 through August 2021 (total sample size of 2 253 567 adults). We found that all 4 interventions mitigated the negative effects of food insecurity on psychological distress among US adults who participated in the survey.
Non-Hispanic White adults experienced greater mitigation effects of the interventions on psychological distress from food insecurity than non-Hispanic Black or Asian adults. However, among all examined racial and ethnic groups, only non-Hispanic White adults experienced a significant interactive effect from unemployment insurance on psychological distress from food insecurity. Given that the amount of unemployment insurance benefits is based on a percentage of an individual’s earnings during a recent 52-week period, 31 and considering racial and ethnic income inequality, inequalities may have occurred in the amount of unemployment insurance benefits received by HPS respondents.
In our study, non-Hispanic Black adults experienced smaller reductions than did non-Hispanic White or Hispanic adults in psychological distress related to food insecurity after the receipt of benefits from various programs during the pandemic. Although not being able to afford to buy more food was the most common reason for food insecurity cited by non-Hispanic Black adults, with 57.4% choosing this survey response option, the mitigation of psychological distress by stimulus funds, SNAP, or free meals was not as large as among other racial and ethnic groups. The lack of mitigation of psychological distress among non-Hispanic Black adults versus adults in other racial and ethnic groups in our study may have been because of the reported high levels of resilience to psychological stressors among non-Hispanic Black adults during the pandemic,52,53 which could have mitigated the negative effect of food insecurity on mental health, thus resulting in a decreased positive effect from interventions on food insecurity. Our findings on psychological distress among non-Hispanic Black adults could have also included psychological distress arising from other factors, such as structural racism or fear of COVID-19 instead of food insecurity.17,54,55 Future research on food insecurity and mental health should include investigations on programs and policies that could be of most benefit to racial and ethnic minority groups.
Non-Hispanic Asian adults experienced little effect from the 4 food insecurity–related interventions, which may be explained in part by their reasons for being food insecure. A greater percentage of non-Hispanic Asian adults than adults in other racial and ethnic minority groups (except non-Hispanic other race) reported that their food insecurity came from their inability to get out to buy food (15.2%) or safety concerns or no delivery (9.2%), whereas a smaller percentage of non-Hispanic Asian adults (37.6%) than adults in other racial and ethnic minority groups reported that their food insecurity stemmed from their not being able to buy more food. With the recent White House Memorandum that recognized the role of the federal government to prevent racism and xenophobia against Asian American and Pacific Islander people, 56 the increase in negative sentiments against Asian people, 18 and the negative effects of these sentiments on depression and anxiety, 17 policy makers should also consider programs to mitigate psychological distress from xenophobia or anti-Asian sentiments. Because non-Hispanic Asian people consist of multiple heterogeneous subgroups, variations in the source of food insecurity among Asian subgroups should also be considered. One study found that, since the beginning of COVID-19, Filipino and Vietnamese adults were more likely than other Asian American adults to report not having enough money to buy food, while Asian Indian adults were more likely than other Asian American adults to report not having a way to get to the food store. 57
Limitations
Our study had several limitations. First, the study design did not show a causal relationship between policy programs and psychological distress because of the endogeneity and omitted variable bias. We suggest that longitudinal data, discontinuity design, or strong instrumental variables could be used in future studies to examine the average treatment effect of policy changes on the association between food insecurity and mental health. Second, we stratified models by each intervention as an independent program. However, programs might jointly affect food insecurity and mental health for those who are eligible for multiple programs. However, each intervention occurred during different periods, and the week of data availability varied by intervention. To avoid listwise deletion of data and to use valid survey weights, we decided to estimate separate models for each intervention. We suggest the examination of the cumulative impact of the mitigation strategies for people who received multiple food insecurity–related interventions. Finally, bias may have occurred from the single-item measurement of food insecurity, which was the only available measurement in the HPS. We suggest that the 10-item and 18-item measurements of food security used by the USDA, 58 if data are available, could be used in future investigations.
Conclusions
Food insecurity–related interventions, including SNAP, stimulus funds, unemployment insurance, and free meals, mitigated the negative effects of food insecurity on mental health in the overall population, with effects varying across racial and ethnic groups. To reduce racial and ethnic disparities in the effect of the interventions, it is necessary to investigate pathways through which food insecurity–related interventions reduce psychological distress and to develop programs customized and targeted for specific racial and ethnic groups, considering their cultural and socioeconomic differences.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.