
Abstract
Objectives:
While the needs of human trafficking survivors have been documented in the academic discourse, the saliency of such needs is understudied. This study aimed to reveal the critical needs of service provision for human trafficking survivors in a Midwestern state as perceived by multidisciplinary service providers.
Methods:
Targeting health care, social service, law enforcement, public health, and other service providers involved in anti–human trafficking service delivery, we disseminated a survey using purposive and snowball sampling. Drawing from survey responses collected in 2019 from 107 service providers working with 422 survivors of human trafficking in the previous 12 months in a Midwestern state, we examined the saliency of needs from the perspective of service providers in the health care, criminal justice, and social service sectors.
Results:
Respondents indicated on a Likert scale (1-5) the level of need for 37 social, health care, and legal services in their communities. The top-indicated needs statewide were mental health care, shelter/housing, peer mentorship programs, legal services, transportation, and provider training in juvenile courts, schools, law enforcement, and health care settings on human trafficking.
Conclusion:
The results suggest the need for statewide responses, such as legal assistance networks, telemental health options, and enhanced training collaborations between interpersonal violence and anti–human trafficking service providers. The study findings are generalizable beyond the study site in 3 ways that can guide strategic action: (1) they provide a framework for state-level analysis and strategic planning that parallels the results; (2) they show that regional variation is possible and should be accounted for in state-level study design, analysis, and strategic planning; and (3) the implications for housing assistance, legal assistance, mental health/substance use disorder–related health care, and training are scalable.
During the last 20 years, anti–human trafficking professionals have worked to understand the phenomenon of human trafficking and improve outreach and response.1-4 Much of this work focuses on understanding the risks and impacts of human trafficking.5-11 However, scant literature has examined the nuances of service needs among human trafficking survivors and related regional contexts. Although the legislation and subsequent approach are largely centered on criminal justice efforts, many other fields, such as public health, have contributed nuanced knowledge about human trafficking and its consequences.
Viewing human trafficking as a public health issue requires a focus on mental and physical health and responses in health care, social, and legal services. While the public health framework helps contextualize negative health outcomes, it also encourages the exploration of individual and community assets, allowing a holistic view of responses. Negative health consequences associated with human trafficking include substance use disorder, sexually transmitted infections, and physical injuries.5,12-14 Known mental health consequences include depression, anxiety, dissociation, hypervigilance, suicidal ideation and attempts, and other symptoms interrelated with posttraumatic stress disorder.9,15,16 Complex trauma can also lead to fragmented memories, attachment disorders, and problems establishing appropriate interpersonal boundaries. 17 The psychological trauma experienced by human trafficking survivors affects well-being, development, trust, and impulse control,18-20 resulting in strained social and interpersonal relationships. Furthermore, poly-victimization involves a trajectory of trauma over time, potentially compounding already complex traumatization.5,18,21,22
Survivors of human trafficking have diverse and multifaceted needs associated with such mental and physical health ramifications, which vary considerably depending on individual experiences. Among the most immediate and basic needs of human trafficking survivors are access to shelter, food, clothing, drinking water, transportation, crisis intervention, drug detoxification, safety/crisis intervention, trauma-informed mental health services, language access services, emergency medical care, and crisis legal advocacy.17,23-26 Long-term needs include access to safe transitional or general housing, physical and mental health care, legal services, language services, immigration services, substance abuse services, education, career counseling, job and life skills training, and financial management.17,23,24 Human trafficking survivors experience difficulty accessing social services, law enforcement assistance, and health care.5,27,28 In addition to resource gaps, training gaps have been identified,25-29 which affect multidisciplinary providers’ ability to identify and respond to potential human trafficking incidents in various organizational sectors. Studies show the need for training in the criminal justice system, health care, intimate partner violence (IPV) services, rape and sexual assault services, and organizations serving young people. Yet, such trainings are limited, nonexistent, or nonmandatory, or they require ongoing training because of high staff turnover rates, such as in policing and children’s services.19,30 Identification, referral, and reporting protocols as well as interagency responses are scarce. While research uncovers the individual needs of survivors and gaps in training, the extent to which these services, training, and protocols are needed in regional contexts is understudied.24-26 We assessed anti–human trafficking service providers’ perceived levels of need for various legal, health care, and social services in Missouri and Metro East St. Louis, Illinois, and by region.
Methods
During May–June 2019, the research team administered a survey intended to provide a needs assessment in Missouri and Metro East St. Louis, Illinois, from the perspective of those working with human trafficking survivors in the social, legal, and health care service sectors. The survey asked service providers for demographic characteristics of the survivors they served in the prior 12 months, as well as demographic characteristics of the providers themselves, as reported in a recent publication documenting the demographic characteristics of survivors in this study. 31 In all, 107 respondents who worked with 422 human trafficking survivors in the previous 12 months participated in the research. The study was approved by the University of Missouri Institutional Review Board.
We disseminated a 41-item electronic survey using an anonymous Qualtrics link emailed to anti–human trafficking coalitions statewide, as well as organizations known to work with human trafficking survivors. These organizations included state domestic and sexual violence response and juvenile justice association listservs. Purposively selected social, health, and legal service organizations were also recruited for survey participation; they were identified in another wave of the larger project from which the current study is drawn to account for regional representation and organizational context. In addition, respondents were encouraged to forward the survey link to people outside the listserv who were involved in anti–human trafficking efforts. Because of our reliance on listservs and snowball sampling, we could not estimate an accurate response rate for this study. Anti–human trafficking service provider respondents were asked to indicate the level of need for 37 services in their respective communities on a 5-point Likert scale, where 5 = very high and 1 = very low. We tabulated median responses for the 37 variables for which respondents indicated the level of need. We also asked respondents to indicate the top 3 needs in their communities, which we sorted by region.
Results
Of 107 survey respondents, 71 (66.4%) indicated primarily working with US citizens and 7 (6.5%) indicated primarily working with foreign nationals; the remaining 29 (27.1%) respondents did not indicate which population they worked with primarily. Respondents reported working primarily with survivors of sex trafficking (57.9%, n = 62), both sex and labor trafficking (12.1%, n = 13), and labor trafficking (2.8%, n = 3); the remaining 29 participants did not report working with a specific type of trafficking. Of the 422 identified survivors with whom respondents indicated they were working within the previous 12 months, 20 (4.7%) experienced labor trafficking only, 53 (12.6%) experienced both sex and labor trafficking, and 349 (82.7%) experienced sex trafficking only.
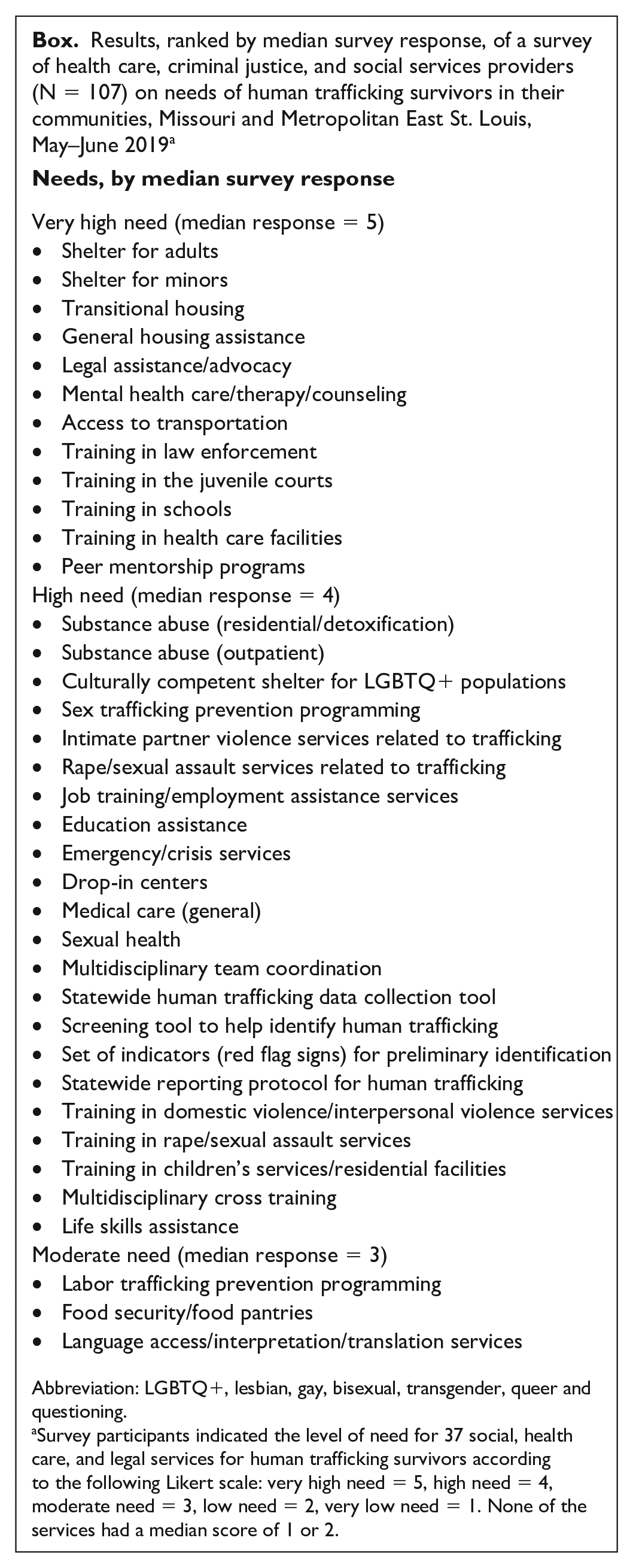
Overall, respondents perceived that their clients had immense needs (Box), all of which were scored as very high (5), high (4), or moderate (3). The most needed services (median = 5) were associated with aspects of mental health care, peer mentorship, shelter/housing, access to transportation, legal assistance/advocacy, and various training needs, particularly in the criminal justice system, schools, and health care.
Results, ranked by median survey response, of a survey of health care, criminal justice, and social services providers (N = 107) on needs of human trafficking survivors in their communities, Missouri and Metropolitan East St. Louis, May–June 2019 a
Abbreviation: LGBTQ+, lesbian, gay, bisexual, transgender, queer and questioning.
Survey participants indicated the level of need for 37 social, health care, and legal services for human trafficking survivors according to the following Likert scale: very high need = 5, high need = 4, moderate need = 3, low need = 2, very low need = 1. None of the services had a median score of 1 or 2.
High-level needs (median = 4) were related to substance use disorder, drop-in centers, emergency/crisis services, health care, training, and rape/sexual assault and IPV services (Box). Services aimed at autonomy, such as education, life skills, and/or job training/employment assistance services, were also ranked as highly needed services. Services related to identification and reporting, such as a statewide reporting protocol, a statewide human trafficking data collection tool, an evidence-based set of indicators (eg, red flags), multidisciplinary team coordination, and an evidence-based screening tool, were also highly ranked. In addition, culturally competent shelter for lesbian, gay, bisexual, transgender, and queer/questioning populations and sex trafficking prevention programming were indicated as high-level needs.
Moderate-level needs (median = 3) included food security/food pantries, language access/interpretation/translation services, and labor trafficking prevention programming (Box). Overall, few differences existed between needs reported by those serving sex trafficking survivors only compared with those serving labor and sex trafficking survivors. Major distinctions of those serving survivors of sex and labor trafficking and labor trafficking only were reporting of labor trafficking prevention programming and language access services as very high-level needs, whereas those who served only sex trafficking survivors reported these needs as moderate.
Regional distinctions are apparent in the ways respondents prioritized service needs (Table). A priority among all regions and the state was mental health care (operationalized as mental health care/therapy/counseling). The greater St. Louis metropolitan area indicated a great need for adult shelter and legal assistance. The Kansas City metropolitan area indicated a great need for emergency crisis and legal services. In the southeastern and northeastern regions, the top 2 needs were shelter for adults and mental health care. The third-ranked need was substance abuse–related services in southeastern Missouri and transitional housing in northeastern Missouri. In southwestern and northwestern Missouri, respondents indicated similar needs with mental health care and legal assistance (Table). In the central region, a rural/suburban mix, the highest needs were for mental health care, transportation, and adult shelter.
Ranked top 3 service needs, by region, identified in a survey of health care, criminal justice, and social services providers (N = 107) on service needs of human trafficking survivors in their communities, Missouri and Metropolitan East St. Louis, Illinois, May–June 2019 a
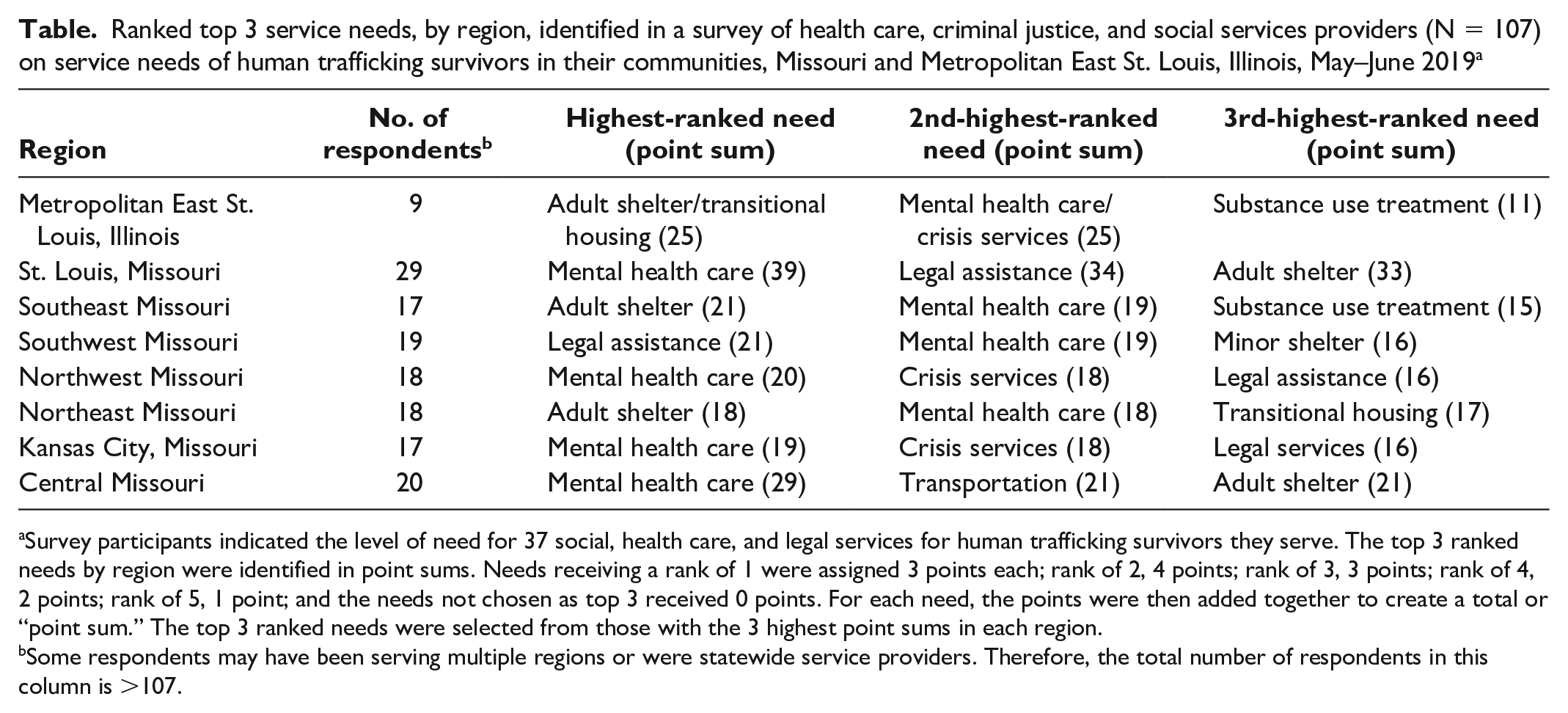
Survey participants indicated the level of need for 37 social, health care, and legal services for human trafficking survivors they serve. The top 3 ranked needs by region were identified in point sums. Needs receiving a rank of 1 were assigned 3 points each; rank of 2, 4 points; rank of 3, 3 points; rank of 4, 2 points; rank of 5, 1 point; and the needs not chosen as top 3 received 0 points. For each need, the points were then added together to create a total or “point sum.” The top 3 ranked needs were selected from those with the 3 highest point sums in each region.
Some respondents may have been serving multiple regions or were statewide service providers. Therefore, the total number of respondents in this column is >107.
Discussion
Although our results were limited to the midwestern state from which the data were drawn, our study findings provide a framework for state-level analysis and strategic planning. First, other states may include in their measures the saliency of needs to identify priority areas to guide targeted intervention. Second, the potential for regional variation (ie, rural vs urban, nation vs western region) can be incorporated into the study design to identify strategic action that is regionally focused. Third, including the salience of needs of human trafficking survivors and service providers (eg, need for screening/identification tools, multidisciplinary teams, data collection tool) into the study design can provide a robust basis for state-level strategic planning.
In our study, the state as a whole indicated many complex needs, as shown by the number of needs ranked highly or very highly. Statewide needs assessments in other locales similarly showed an overall dearth of services.31-35 In one study, more than 80% of respondents indicated their organization was not able to meet human trafficking survivors’ needs, and lack of resources was among the top 3 ranked critical barriers to service provision. 32 Hence, anti–human trafficking service providers perceive a need for developing basic services related to accessibility and delivery of services and more training on human trafficking and the intersections of human trafficking with other phenomena such as domestic and sexual violence, supporting prior research.25,26
We also identified needs related to housing and shelter, which supports previous research.19,25,32,34 A needs assessment in Virginia showed emergency housing as one of the most needed services. 30 Another multistate study found accessing stable and affordable housing as a top-ranked community resource limiting the risk of human trafficking. 33 Public health responses must address housing needs because they are among the most salient needs. One solution may be to use innovative housing programs such as Safe Shelter Collaborative or Sheltered Alliance, which pairs the short-term housing needs of human trafficking survivors with available donors, or establishes a collaborative system to make efficient use of available bed space in social services.36,37
Although our needs assessment did not specify whether survivors were in need of legal services as defendants or if they needed assistance with prosecution, research indicates that human trafficking survivors are often arrested and charged with interrelated crimes, such as loitering, vagrancy, drug-related crimes, and prostitution.11,35,38 In Missouri, human trafficking survivor–based groups and their allies have lobbied for expunged records/vacated convictions of human trafficking survivors, indicating a need in the state for legal services as defendants. 39 Alternatively, if survivors are in need of prosecution-based legal services, this need may reflect a general lack of awareness about human trafficking 26 or that these cases are difficult to litigate. 30 A solution for the limited access to legal assistance may be to develop more coordinated state and national legal networks, such as through law schools, legal clinics, state or local bar associations, or creating a national legal services network similar to the Health, Education, Advocacy, and Linkage (HEAL) Network for public health and medical workers that offers training, technical support, and community (https://healtrafficking.org). Increasing access to services and sharing the work of service provision and advocacy for these complex cases are essential. 35
We identified a need for increased culturally sensitive and basic supportive services for human trafficking survivors across the state, in crisis and longer-term settings, including services related to mental health care and substance use treatment. This finding is consistent with the findings of prior statewide needs assessments, which also showed counseling as a top-ranked need and important community resource.31,33 Moreover, understanding interrelated needs is important to maximize service utilization. Many shelters do not provide services to those who are actively using substances or are in active mental health crises. Hence, these individuals may first need substance use and mental health care stabilization before accessing shelter services, suggesting the need for better collaboration between crisis shelter and mental health care providers. To address this issue, state and national survivor networks may consider collaborating more regularly to propose changes to victim services programs through legislation such as the Violence Against Women Act 40 and the Trafficking Victims Protection Act 41 to ease the conflict agencies and survivors face.
The context of rurality indicates that proximity affects barriers to services and implies potential economic barriers to access, as it does across the nation. This finding indicates that regional contextual dynamics other than urban setting affect service needs in these communities. Overall, the regional comparisons show the importance of locally grounded, contextualized responses to human trafficking, to adequately respond to regionally defined needs, related assets, and deficits. Missouri is a unique microcosm of the United States because it closely replicates national urban–rural population densities. Nationally, 19.3% (about 60 million) of residents live in rural-designated areas. 42 In Missouri, 36.9% (2.2 million) of the state’s population resides in rural-designated areas. 43 A multistate study found resource scarcity in rural communities but also described smaller interagency networks typically of such communities as assets, intensifying collaboration and improving social capital. 34 In Missouri, efforts have been made to increase telemental health options for rural Missourians supported through the expansion of state laws on behavioral health, substance use treatment, and case management. However, one barrier to the sustainability of telehealth options is a lack of broadband internet access, which affects nearly 20% of the state’s rural residents. 44 According to the Brookings Institution, rural United States has an internet problem, much like what is experienced in Missouri. 45 Expanding telehealth capacity for therapy and recovery support services for substance use disorder would address location-based barriers to some degree, although challenges would remain for those with limited connectivity or with inaccessibility of technology. Despite these issues, telemental health and substance use treatment options have been developed in Missouri and the nation. For example, the University of Missouri Health system has offered telehealth services since 1994 in several languages and provides telehealth training for health care providers across the state. 46 Across the United States, there are a number of internet-facilitated mental health services, such as TalkSpace (https://www.talkspace.com) and similar services.
One solution to the lack of therapeutic access may be to identify service providers that are willing to provide services remotely, such as through telehealth, to expand accessibility in rural areas. Another solution is to find local therapists and clinics willing to provide uninsured and sliding-scale services for human trafficking survivors to increase access for those with economic or broadband internet barriers. These solutions could be scaled up to a national network of providers that offer affordable and accessible services. In addition, immigrant survivors could benefit from mental health experts providing letters explaining the individuals’ experiences with trauma and its impact on their lives to the court in their petition for humanitarian relief to address costs.
A potential barrier to the success of telemental health and substance use treatment support is language accessibility. Expanding availability of language access services can be accomplished through dissemination of information about hotlines or expanded outreach from organizations in states that offer these services and expanding virtual options for language access and translation services. In addition, with a national network, professionals with various language abilities would be accessible. Almost all our survey respondents indicated that peer mentorship and support groups are needed among all types of human trafficking. Many organizations specific to human trafficking and exploitation provide peer mentorship, and these organizations should consider expanding peer mentorship through telehealth options or collaborating with the National Survivor Network.
Prior research found human trafficking training in Missouri to be sufficient but lacking in areas such as coordinated case management and trauma-informed identification and intervention. 26 Although most service providers reported having received basic training in human trafficking, they wanted to see more advanced training in best practices, information on key identifiers of human trafficking, case coordination and multidisciplinary team coordination, and trauma-informed care. 26 The findings of our study support previous research showing that training, particularly multidisciplinary training, is a critical need. A needs assessment in Virginia showed training and coordinated services were critically needed, and lack of training was among the top 3 barriers to service provision. 31 A statewide study in Georgia showed coordinated service provision, cross-agency collaboration, and training as top recommendations. 32 A multistate study found interagency networks were essential for training and coordinating key resources. 33 Our study found a very high need for training in juvenile courts, schools, law enforcement, and health care settings on human trafficking, likely reflecting gaps in training, increased likelihood of identification in these sectors, or high staff turnover. Service providers also recognized the need for more training in schools, health care, and law enforcement settings, particularly in multidisciplinary cross-training, coordination, and team building, and these findings support those of previous studies.26,47
Of particular interest is the need for more training for service providers in sexual assault and IPV organizations related to human trafficking. Relatedly, more efforts are needed to form stronger relationships with already existing domestic and sexual violence leaders to develop appropriate service modifications for human trafficking survivors receiving aftercare through non–trafficking-specific agencies. Leaders in the Missouri Coalition Against Domestic and Sexual Violence, Futures Without Violence, the National Coalition Against Domestic Violence, and other anti-violence groups are already addressing some of the intersections between human trafficking and domestic and sexual violence, and they have produced numerous trainings, reports, and research on this intersection. Leaders in the anti–human trafficking movement in Missouri and other states should consider reaching out to these organizations for support and guidance in developing enhanced response services for victims of human trafficking.
Finally, we recommend implementing a strategic plan protocol for statewide and regional anti–human trafficking activities and policymaking using asset mapping and logic modeling to focus on community strengths to address identified needs. We proposed such a plan, which is detailed elsewhere. 48 To scale this emerging protocol to a national scope, regional differences and differences that are inherent between urban and rural settings should be considered.
Our findings are generalizable beyond the study site in 3 important ways that can guide strategic action: (1) they provide a framework for state-level analysis and strategic planning that parallels the results; (2) they show that regional variation is possible and should be accounted for in state-level study design, analysis, and strategic planning; and (3) the implications for housing assistance, legal assistance, mental health/substance use disorder–related health care, and training are scalable.
Conclusion
Our study indicates findings specific to a Midwestern state, an under-researched area in the larger anti–human trafficking discourse. However, our findings are potentially applicable nationally, as nearly all needs were ranked as very highly or highly needed, the findings were consistent with prior research, and top-ranked needs (eg, mental health care, housing) were relatively consistent across rural and urban regions; thus, related recommendations are broadly implicated beyond the state level. Our results also indicate the importance of a locally grounded, regionally contextualized response targeting the top-identified needs to best allocate local resources. This methodology can be replicated in other states that engage in similar needs assessments. Missouri, like other states, is developing collaborative models in an effort to increase the efficiency and accountability of trainings, shelter access, mental health, and legal services. All states can conduct statewide and regional needs assessments to uncover priority areas to guide targeted initiatives to improve service access for human trafficking survivors.
Footnotes
Acknowledgements
The authors acknowledge the participants who helped make this study a success and increase our knowledge about human trafficking strategic planning. We are humbled by your dedication to the pursuit of justice and knowledge.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Missouri Collaborative Against Human Trafficking.