
Abstract
Suicide rates among veterans are higher than those of the general US population. Although veterans compose only 7.6% of the US population, nearly 14% of American adult suicides are among veterans. The rate of suicide is 1.5 times higher among all veterans and 2.1 times higher among female veterans compared with the general population. Only 47% of all veterans are enrolled in the US Department of Veterans Affairs (VA) Healthcare System, leaving a large number either not receiving health care or receiving it outside the VA. Recent legislation has improved access to care for veterans outside the VA, highlighting the need for a broad public health approach to address veteran suicide and the need for all health care institutions and clinicians to be familiar with the unique health concerns in this population. The purpose of this narrative review was to summarize the risk factors contributing to veteran suicide and to provide guidance on how to assess and mitigate these risks. Suicide is preventable through recognition of risk and prompt intervention. Health care providers both inside and outside the VA system are uniquely situated at the intersection of the many contributing factors to veteran suicide and should have a structured, proactive approach to address the problem.
Suicide is preventable through recognition of risks and prompt intervention. This review has a dual mission: to assist Veterans Administration (VA) and non-VA health care providers in recognizing risk factors for veteran suicide and to provide practical guidance for assessing and mitigating risk. Veterans are more likely to die by suicide than nonveterans. Although veterans compose 7.6% of the US population, 1 nearly 14% of American adult suicides are among veterans. 2 The rate of suicide is 1.5 times higher among all veterans and 2.1 times higher among female veterans compared with the general population. 2 Suicide prevention is a top VA priority, and VA initiatives (Veterans Crisis Line, Recovery Engagement and Coordination for Health–Veterans Enhanced Treatment [REACH-VET] program, yearly suicide screenings) may account for reduced suicide rates among veterans who use VA services. 2 However, more than half of veterans do not use VA services, 3 and one-quarter of veterans lacking health insurance who qualify for VA health care remain unenrolled. 4 Eligibility for VA services varies according to veteran status, service-connected disability, and income level. Recent legislation will likely increase care received outside the VA. The Veterans Choice Program of 2014 5 and the MISSION Act of 2018 6 increase access to health care services. The MISSION Act allows access to non-VA providers if appointment wait time or travel time exceeds designated limits. 6 The program has included 880 000 health care providers, and participating community urgent care clinics have accommodated more than 140 000 patient visits. 7 The large number of non-VA health care providers delivering care to veterans emphasizes the need for universal veteran-informed care.
Author’s Personal Story (Frank Ruiz)
I served in the Navy from 2002 to 2007 and spent several years in the Middle East as part of Operation Enduring Freedom and Operation Iraqi Freedom. After discharge, I found myself harboring the problems of service but lacking the structure and support of the military. I struggled with posttraumatic stress disorder (PTSD), substance use disorder, and suicidal ideation. I drifted between Veterans Administration (VA) and non-VA health care providers. If I had not volunteered the information, my status as a combat veteran would have never been discovered by my non-VA health care providers. Over time, I saw improvements in the cultural competency of VA clinicians and better recognition of troubled behaviors. Nearly 9 years after leaving active duty, I attended a residential treatment facility that specialized in treating co-occurring PTSD and substance use disorder. Fortunately, I got back on track and enrolled in medical school. As I learned of yet another brother or sister who had taken their life, it became clear that health care professionals require better training on how to identify and mitigate suicide risk among veterans.
Methods
This narrative review synthesizes recent literature on veteran suicide; it is not an exhaustive or systematic review. In general, lack of systematic selection of studies may lead to interpretation bias. We based our article selection on clinical relevance determined by article metrics (the number of times an article has been accessed and the number of times the article has been cited) and authors who are subject matter experts. In January 2021, we performed a PubMed literature search using the terms “veterans” and “suicide,” with publication dates in the previous 15 years (beginning January 1, 2006, and ending January 31, 2021). We then categorized articles in terms of risk and prevention. Once we identified important risk factors, we pursued additional literature searches to add details to each section. Wherever possible, we stratified articles by journal impact factor, article metrics, and article date to emphasize relevance. Authors also queried subject matter experts in the VA to ensure that we included important, relevant articles.
Results of Synthesis
Contributing Factors
Contributing factors to veteran suicide or suicidal behavior can be categorized into individual risks and broad socioecological risks.
Individual risks
Mental health
Mental health conditions are associated with an increased risk of veteran suicide, a concern given that almost one-quarter of veterans receiving VA care reported 1 or more mental illnesses. 8 A large prospective study of current and former military personnel found mental disorders to be associated with suicide risk, including depression (hazard ratio [HR] = 1.96; 95% CI, 1.05-3.64), manic-depressive disorder (HR = 4.35; 95% CI, 1.56-12.09), and alcohol-related problems (HR = 2.56; 95% CI, 1.56-4.18). 9 A recent retrospective case-control study linked mental health conditions and veteran suicide: anxiety disorders (odds ratio [OR] = 3.52; 95% CI, 1.79-6.92), functional decline (OR = 2.52; 95% CI, 1.55-4.10), suicidal ideation (OR = 2.27; 95% CI, 1.07-4.83), and depression (OR = 1.82; 95% CI, 1.07-3.10) were associated with the highest risk. 10 In another veteran retrospective case-control study, mental health diagnoses, including bipolar disorder, depression, alcohol use disorder (AUD), substance use disorder (SUD), anxiety, schizophrenia, and posttraumatic stress disorder (PTSD), were all associated with an increased suicide risk, with an overall HR of 2.50 (95% CI, 2.38-2.64) among men and 5.18 (95% CI, 4.08-6.58) among women. 11 A retrospective case-control study noted an association of PTSD with veteran suicide risk, although this association attenuated when adjusted for mental health diagnoses, most markedly, depression. 12 Veterans with positive results on the Primary Care–PTSD screen were found to have increased suicide mortality, particularly when reporting feeling numb or detached, 13 and both hopelessness and suicidal ideation were identified among Operation Enduring Freedom/Operation Iraqi Freedom veterans with PTSD symptoms below diagnostic threshold. 14 In an analysis of Vietnam veterans, the risk of suicide associated with PTSD and depression was similar (HR = 7.1 [95% CI, 4.9-10.3] and HR = 7.2 [95% CI, 4.8-10.8], respectively), and veterans with both PTSD and depression had the highest risk (HR = 15.2). 15 Substance use and mental health disorders often co-occur to amplify suicide risk.
Substance use disorder
SUD is linked to an increased risk of veteran suicide. In a recent veteran cohort study, SUD conferred increased suicide risk, especially among women, although co-occurring mental health disorders magnified this association. Adjusted for factors such as comorbid psychiatric diagnosis, the association between SUD and suicide had an HR of 1.67 (95% CI, 1.55-1.97) among men and 2.15 (95% CI, 1.44-3.21) among women. 16 Sedative/hypnotic/anxiolytic use disorder conferred the highest risk. 16 The prevalence of substance misuse is high among young veterans, including past-year illicit drug use (38% among men, 29% among women) and prescription drug misuse (18% among men, 14% among women), and a higher prevalence of AUD, SUD, and heavy episodic drinking among younger male veterans than among civilian males. 17 The complex interplay among mental health, SUD, and suicide should not be underestimated. A cycle of clinical deterioration was described among Vietnam veterans, where SUD exacerbated PTSD and suicidality, which then propagated substance use. 18
Traumatic brain injury (TBI)
TBI is also a risk factor in veteran suicide and suicidal ideation. Nearly 414 000 TBIs occurred among military service members between 2000 and late 2019. 19 A retrospective veteran cohort study found an association between TBI and suicide risk after adjusting for covariates (HR = 1.71; 95% CI, 1.56-1.87), with risk increasing with TBI severity. 20 In addition, rates of suicidal ideation in the general population were higher among people with TBI than those without TBI 21 and among recent Operation Enduring Freedom/Operation Iraqi Freedom veterans with multiple TBIs (vs veterans with no TBI) (OR = 1.76; 95% CI, 1.01-3.06). 22
Life disruptions
Major life disruptions are an important factor in the lives of military personnel and in veteran suicide, with many experiencing a recent life crisis prior to death, including relationship-, job-, or school-related problems; housing instability; military-related stress or separation; legal/financial issues; functional decline; loss of a loved one; or isolation/social withdrawal.10,23,24 One study of US Army personnel showed a high prevalence of stressful life events in suicide decedents, including intimate partner problems (45%), military-related stress (41%), and current job-related problems (61%). 23
Military sexual trauma (MST)
MST (defined as any experience of sexual assault or threatening sexual harassment during military service) has also been associated with increased risk of suicide among veterans (HR = 1.69 [95% CI, 1.45-1.97] among men; HR = 2.27 [95% CI, 1.76-2.94] among women), 25 suicide attempts among female service members (OR = 3.0; 95% CI, 2.5-3.6), 26 and suicidal ideation. 27 All veterans receiving care at the VA are screened for MST using a clinical reminder system, with MST reported by 1.1% of men and 21.2% of women. 25
Socioecological risks
Lethal means access
Firearms are disproportionately used in veteran suicide, accounting for nearly 70% of male and 42% of female suicide deaths (20% higher than the general population). 2 This difference is in part attributable to access to firearms. Gun ownership is approximately 120% higher among veterans than in the general US population. 2 Nearly 45% of veterans own 1 or more firearms. 2 Only 1 in 3 veterans follow guidelines for safe firearm storage. 28 Intentional poisoning is also a common method of suicide, particularly among female veterans, with drug overdose the method in more than 31% of female veteran suicide deaths. 29
Homelessness, poverty, and geography
Homelessness and poverty are important risk factors for veteran suicide. Veterans with a history of homelessness were 7.8 times more likely to have attempted suicide than veterans without a history of homelessness, with lifetime homelessness associated with lifetime suicide attempts when adjusted for potential confounders (adjusted OR = 3.75 [95% CI, 3.72-3.77] among veterans; adjusted OR = 1.83 [95% CI, 1.83-1.84] among nonveterans). 30 Among patients receiving VA care, those at risk of or with a history of homelessness had higher rates of suicide than those who were not experiencing homelessness. 31 Conversely, veterans who have a service-connected disability (injury/illness related to military service that links the veteran with VA benefits, including financial compensation, depending on disability) have decreased odds of suicide.10,31 Poverty has been identified as a risk factor for death by suicide in the older US population (adjusted HR = 1.34; 95% CI, 1.22-1.47). 32 Veteran poverty rates are increasing, with highest rates in the group aged 18-34 years, 33 a population mostly made up of veterans from the Iraq and Afghanistan wars. Veterans from these conflicts may face difficulties finding civilian-equivalent placement for their training and skills. Of note, geographically rural veterans fare worse economically 34 than veterans living in nonrural areas, and veteran suicide decedents were more likely to live in rural areas than in nonrural areas. 31 Military and veteran suicides were concentrated in a small number of counties, with 33% of veteran suicides occurring in just 3.4% of US counties. 35
Potential or understudied factors
Deployment and combat
The relationship between deployment and combat and suicide is complex, although in general neither is linked to increased suicide risk. In a large prospective analysis, deployment-related factors such as combat experience, cumulative days deployed, and number of deployments were not found to be associated with suicide risk. 9 Limited evidence suggests that exposure to death or killing may increase suicidal ideation or risk, although the association is weak. A meta-analysis found substantial heterogeneity and only a small positive association between deployment factors and suicide-related outcomes, with the largest effect from exposure to killing and atrocities (such as direct contact with wounded and deceased or exposures during involvement in humanitarian relief efforts or peacekeeping missions). 36 A literature review pointed to elevated risk of specific combat exposures, such as killing or witnessing death. 37 A retrospective analysis revealed an association between combat experiences involving direct exposure to death, killing, or grave injury and suicidal ideation/attempts (ORs ranged from 1.46 to 1.70). 38
Sexual minority groups
In the general population, suicide attempts are more common among adults in sexual minority groups than among heterosexual adults. 39 Yet, despite literature supporting an increased risk of suicidality among lesbian, gay, bisexual, transgender, and queer (LGBTQ+) individuals in the general population, suicide risk among LGBTQ+ veterans has not been thoroughly evaluated. Lack of data fields for sexual orientation and gender identity in VA electronic health records (EHRs) has impeded accurate data collection. One retrospective study that used language processing of clinical notes found increased crude suicide rates among sexual minority veterans compared with the general veteran population (82.5 vs 37.7 suicides per 100 000 person-years). 40 To address the risk of suicide among LGBTQ+ veterans, the VA has launched a prospective study. 41 The prevalence of gender identity disorder (GID) is higher among VA populations than among the general US population, and the rate of suicide events is 20 times higher among GID-diagnosed veterans than among non–GID-diagnosed veterans. 42
Incarceration
Suicide risk among incarcerated veterans has also been inadequately evaluated, although both incarceration and veteran status increase suicide risk. 43 About 8% of all federal and state incarcerated individuals are veterans, and 55% of incarcerated veterans reported having a mental health diagnosis. 44 In an analysis of incarcerated veterans, 73% were unemployed, 21% experienced long-term homelessness, and alcohol and drug abuse were reported in 50% and 37%, respectively. 45 An incarceration history provides an important insight into many overlapping suicide risk factors.
COVID-19
The VA has yet to identify an increase in suicide-related behavior resulting from the COVID-19 pandemic, 2 although increases in unemployment, 46 substance abuse, suicidal ideation, mental health problems, 47 gun ownership, 48 and isolation 49 may magnify the size of the population of veterans at risk of suicide. Social distancing interventions implemented to reduce the transmission of COVID-19 carry the potential for adverse outcomes on suicide risk. 50
Assessing and Mitigating Suicide Risk in Veterans
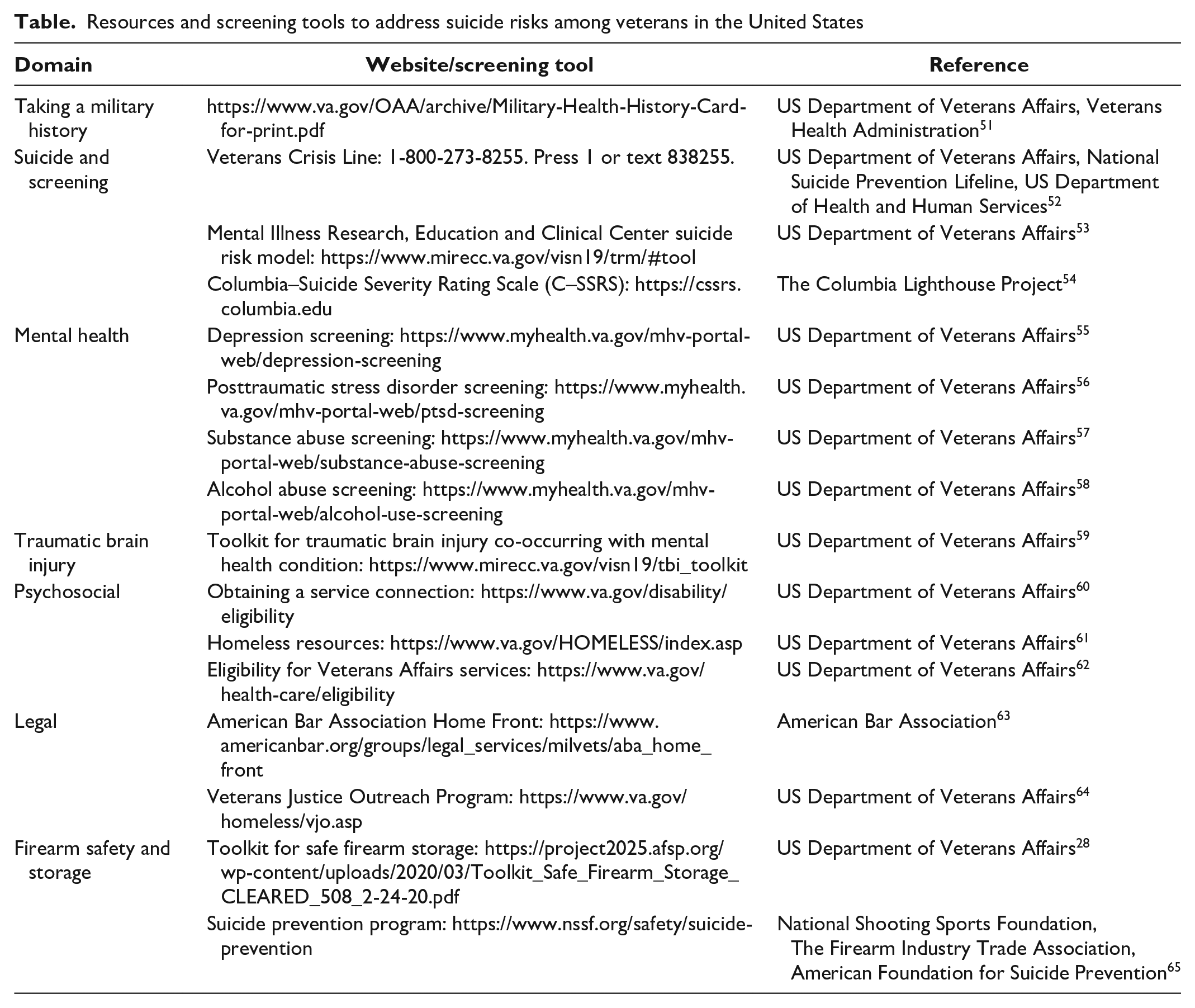
Numerous resources and screening tools, including a list of websites, are available to address suicide risk among veterans (Table). These resources include guidance on how to take a military history, mental health screening, a toolkit on traumatic brain injury, psychosocial resources, legal resources, and a toolkit on firearm safety and storage.
Resources and screening tools to address suicide risks among veterans in the United States
Cultural competency
The most important first step to veteran-informed care is to ask whether a patient is a veteran.66-68 In 1 survey, only 19% of primary care providers reported asking about veteran status on a regular basis. 69 Little guidance exists on how to integrate military history into non-VA EHRs; although the National Academy of Medicine recommended routine incorporation of social and behavioral factors into EHRs, veteran status (initially listed as a potential field) was not on the final list of recommended domains. 70 This problem highlights ongoing systematic challenges in integrating military service history into routine clinical care.
Health care access
Health care access represents an untapped opportunity for suicide risk identification and mitigation. In a study of US Army soldiers, nearly 50% of suicide decedents were found to have accessed health care in the month before their death, and more than 25% had health care contact in the week before their death. 71 More than 80% of people in 11 American health care systems who died of suicide received health care in the year prior to death 72 ; in 1 systematic review, approximately 45% of people had contact with a primary care provider within a month of suicide. 73 Although the highest risk period for suicide among veterans is after a psychiatric hospitalization, 74 more than 85% of suicide decedents do not have such a hospitalization. 72 Many veterans are not eligible for VA health care, and not all eligible veterans are enrolled in VA health care. 4 In a 2014 analysis, about 7% of the nearly 22 million veterans lacked health insurance, 75 and an additional 9% received health care coverage through Medicaid. 76
Suicide risk screening
Given the frequency of health care contact prior to suicide, routine screening has been proposed as a way of mitigating risk. The most recent guidelines of the US Preventive Services Task Force conclude that there is insufficient evidence to assess the balance of benefits and harms of primary care screening for suicide risk in the general adult population. 77 To address whether universal screening can identify veterans at risk of suicide, the VA implemented a suicide risk identification strategy in 2018, which standardized screening and evaluation tools. 78 A recent cross-sectional study of more than 4 million veterans screened in ambulatory care and emergency department settings identified a prevalence of 3.5% for suicidal ideation, with acuity of suicide risk being greater among patients screened in the emergency department and urgent care setting compared with those screened in ambulatory care settings. 78 This study argued that population-based suicide risk screening of veterans in VA care settings may facilitate identification of suicide risk, particularly among veterans not receiving mental health treatment. 78 Given the complex interplay of many contributing individual and socioecological suicide risk factors, researchers have examined predictive modeling as a way of identifying veterans at highest risk. One predictive modeling study indicated suicide rates that were 60 times greater in the validation samples in the highest 0.01% stratum for calculated risk (compared with the overall sample) and 30 times greater in the highest 0.10% stratum, suggesting that predictive modeling effectively recognized patients at high risk of suicide not identified on clinical grounds. 31 The VA uses predictive modeling via the REACH–VET program, which analyzes EHR data to identify veterans at significantly elevated risk of suicide and allows for preemptive support. 79 Timely awareness, screening, and treatment of mental illness and SUD; assessment for a history of TBI; and identification of life stressors and MST are critical. Psychosocial evaluation is also crucial, including assessment for homelessness, poverty, and lack of health insurance.
Reduction in access to lethal means
Reducing immediate access to firearms is an important step in suicide prevention. A recent VA toolkit recommended clinicians distribute safety education materials to veterans at risk of suicide, encourage temporary transfer of firearms or safe gun storage, and provide information on free or affordable options for storing weapons. 28 Safe storage counseling should be considered for veterans who exhibit changes in behavior (including violence, recklessness, or self-isolation), have a history of mental illness or increased use of alcohol or drugs, have had a recent major life event, and express hopelessness. 28 Health care providers should also be knowledgeable of medications with high lethality (including analgesics, stimulants/street drugs, cardiovascular agents, antidepressants, and sedatives/hypnotics) and take steps to limit access to these medications among veterans at high risk of suicide. 29
Integration of mental health services into primary care
Integration of mental health services into VA primary care practice increases the likelihood of continuation of mental health care. 80 An initial encounter in an integrated VA setting results in 1.4 times greater likelihood of follow-up with specialty mental health care. 81 The VA uses patient record flags in the EHR to designate those at high risk of suicide and increase clinical outreach. 82
Suicide prevention framework
From a public health perspective, suicide may be addressed from a primary, secondary, and tertiary prevention framework. Primary prevention involves attention to whole health, including the opportunity for a fulfilling life, financial stability, solid social networks, and health care access. Primary prevention should begin during active duty and be a standard part of transition support after military service. Secondary prevention includes public education and awareness, routine suicide risk assessment and mental health screening, and reduction of access to lethal means. A recent report on community-based approaches to suicide prevention found that reducing lethal means access and screening for depression may reduce suicide deaths. 83 Tertiary prevention includes access to a crisis hotline, urgent care, specialty mental health referral, and hospitalization—interventions that may prevent those actively thinking about suicide from choosing to act. Ultimately, our success in reducing veteran suicides will depend upon efforts in all 3 of these realms of prevention.
Conclusion
One unique quality of military service members is that regardless of their reasons for joining the military, for a time they became a team member, placed their life in harm’s way, and lived with a shared purpose. For some veterans, the return to the civilian life they spent years protecting is no small feat. There is no more tragic failure in reintegrating military service members into civilian society than suicide. When, for whatever reason, a veteran feels alone, without a team, family, or support system, the public health response should be proactive, immediate, and effective. Identifying elevated suicide risk among veterans should occur in all health care settings, including screening for mental health conditions, suicidal ideation, and firearm safety. An integrated, nationwide effort to identify veterans who are hurting and to connect them to resources is imperative. The complexity of how various factors contribute to suicide risk among veterans should not be overlooked. Relief will not be found through patchwork effort but through an integrated, veteran-informed, and veteran-centered approach.
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the US Department of Veterans Affairs or the US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.