
Abstract
Objectives:
Although much research has been conducted on knowledge and awareness of the connection between human papillomavirus (HPV) and cervical cancer risk among university students, few studies have examined these associations among low-income populations. We examined knowledge of HPV and cervical cancer risk among racially and ethnically diverse low-income women.
Methods:
We used a cross-sectional study design to recruit and interview 476 low-income women in New Jersey from November 1, 2013, through February 28, 2016. We used multivariate logistic regression to determine whether knowledge of HPV and its association with cervical cancer risk differed by race and ethnicity.
Results:
Compared with non-Hispanic White women, Hispanic (odds ratio [OR] = 0.37; 95% CI, 0.18-0.77) and non-Hispanic Black (OR = 0.38; 95% CI, 0.19-0.77) women were significantly less likely to report having heard of HPV. Of women who had ever heard of HPV (n = 323), non-Hispanic Black women were significantly less likely (OR = 0.44; 95% CI, 0.21-0.89) than non-Hispanic White women to report knowing that HPV can be associated with cervical cancer.
Conclusions:
Given the higher rates of HPV infection among non-Hispanic Black and Hispanic women, these results suggest a need to improve education about risks of HPV among low-income populations. These messages need to include information on the connection between HPV and cervical cancer and must be provided in culturally and linguistically appropriate ways.
The American Cancer Society (ACS) estimated that about 14 480 new cases of invasive cervical cancer would be diagnosed in 2021 and be responsible for an estimated 4290 deaths. 1 The incidence of and mortality rates for cervical cancer have declined overall in the past 50 years.2-5 In addition, rates of human papillomavirus (HPV), which is responsible for virtually all cervical cancer diagnoses, 2 have decreased as a result of HPV vaccines. 6 While overall decreases have occurred in HPV prevalence 6 and in cervical cancer incidence and mortality rates,2-5 disparities persist in cervical cancer incidence.1,7
Consistent racial and ethnic disparities in the overall incidence of cancer may result from poverty, lack of access to health insurance, and broader social inequalities. 1 Cervical cancer diagnosis rates are higher among non-Hispanic Black and Hispanic women than among their non-Hispanic White counterparts. 1 This disparity may be a result of differences in screening behavior or general knowledge of cervical cancer and HPV. Cervical cancer is highly preventable with early prevention screening efforts.7,8 Most women who are diagnosed with cervical cancer have not been screened recently, 1 and delayed screening results in a higher death rate. Hispanic women are the main population group to be diagnosed in the later stages of cervical cancer, 8 which may in part lead to disparities in cervical cancer mortality. For example, Hispanic women are 1.26 times more likely to die of cervical cancer than their non-Hispanic White counterparts. 7
In addition to differences in screening patterns, differences in HPV and vaccination rates may account for disparities in cervical cancer outcomes. HPV rates are significantly higher among those living below the federal poverty level, as well as among racial and ethnic minority groups such as non-Hispanic Black and Hispanic women.3,9 While the impact of race and socioeconomic status (SES) on HPV vaccination rates is inconsistent in the literature, with some data indicating higher rates among low-income groups 10 and other data showing higher rates among high-income populations, 11 some evidence suggests that non-Hispanic Black and Latina populations in the United States are less likely to complete the HPV series than non-Hispanic White women.12,13 Differences in HPV incidence by race also intersect with income, such that race–class disparities exist; non-Hispanic Black and Hispanic women with lower SES have a higher incidence of HPV than do non-Hispanic Black or Hispanic women with higher SES and non-Hispanic White women regardless of SES. 14
Currently, women aged 21-65 years are recommended to undergo cytology screening (Papanicolaou [Pap] test) every 3 years, and women aged 30-65 years can extend the screening interval to every 5 years with the addition of an HPV test. 15 While the incidence of cervical cancer has mirrored the national trend and has been declining in New Jersey, substantial variation in Pap testing and HPV tests persists within population subgroups. 16 Llanos and colleagues 16 noted that in their sample of more than 50 000 uninsured and underinsured women in New Jersey, 70.6% had had only 1 Pap test in the previous 6 years, and women who reported more Pap tests were also more likely to have been tested for HPV. In addition, racial and ethnic minority, uninsured, and lower-SES women tended to be screened less often than non-Hispanic White, insured, and higher-SES women. 16 In New Jersey, several counties (eg, Atlantic, Essex, Hudson) have lower rates of HPV testing and a higher incidence of cervical cancer across all racial and ethnic groups, while other counties (eg, Bergen, Morris, Mercer) have higher rates of HPV testing and a lower incidence of cervical cancer.16,17 There is a paucity of literature assessing what may be leading to these variable screening rates in terms of knowledge or awareness of HPV among medically underserved, low-income racial and ethnic minority populations. To begin to understand factors that may influence differences in cervical cancer incidence in New Jersey, we examined HPV knowledge and awareness of the association between HPV and cervical cancer risk among low-income non-Hispanic Black, non-Hispanic White, and Hispanic women in this region.
Methods
Study Population
Our study design is described in detail elsewhere. 18 Briefly, study participants were recruited by using a convenience sampling methodology and posting fliers describing the study at collaborating agencies. These agencies included NJ SNAP-Ed and Expanded Food and Nutrition Education Program (EFNEP) classes, Work First NJ program centers, and other agencies serving low-income people in New Jersey. People interested in participating then contacted the research team to schedule an interview. Participants received either $20 cash or a $20 gift card as compensation for participation. We conducted face-to-face interviews for 476 participants using a tablet application survey tool, QuickTap Survey (Formstack), between November 1, 2013, and February 28, 2016.
Interview Questions
Before initiating each interview, we obtained informed consent from all participants. During the interview, trained interviewers administered a structured questionnaire in either English or Spanish. Interviewers collected information on participant awareness and knowledge of HPV as a risk factor for cervical cancer. Participants were first asked if they had ever heard of HPV, and for those who responded yes, we asked them to respond yes, no, or unsure to the following questions: “HPV can cause cervical cancer,” “HPV is a sexually transmitted infection,” and “HPV is a virus.” Data collected on demographic characteristics included race and ethnicity, age, annual household income (<$8000 or ≥$8000 per year), education (≤high school diploma, ≥some college), and marital status (not married/not living as married or married/living as married). We measured access to medical care through health insurance status (current status and status within the past 2 years), having a primary care physician or usual source of care (yes/no), number of physician visits in the past year, and physician recommendation for screening (yes/no). In addition, interviewers asked participants their perception of the risk of developing cervical cancer by asking participants the following questions: “How likely do you think it is that you will develop cervical cancer during your lifetime?” and “Would you say that your chance of getting cervical cancer is . . . ?”
Of the 476 people who were interviewed, we considered participants ineligible for inclusion in these analyses if they did not answer the question on our primary dependent variable, “Have you ever heard of HPV?” (n = 18) or if they reported a racial and ethnic identity other than non-Hispanic White, non-Hispanic Black, or Hispanic (n = 17). Thus, we included a total of 442 study participants in these analyses.
Data Analysis
We conducted unadjusted comparisons of potential explanatory variables using analysis of variance (for continuous variables) and Pearson χ2 tests (for categorical variables) to determine differences in knowledge and awareness of HPV as a risk factor for cervical cancer, by race and ethnicity, as well as between these variables and potentially confounding factors.
We then used unconditional logistic regression to estimate odds ratios (ORs) and corresponding 95% CIs for the association between knowledge and awareness of HPV as a risk factor for cervical cancer and race and ethnicity. We used multivariate models controlling for potential confounders such as income, education, age, marital status, health insurance status, access to health care, and perception of cancer risk to determine the most parsimonious models.
All tests of significance were 2-tailed, with P < .05 considered significant. We performed all analyses using SPSS version 21.0 (IBM Corp). This study was approved by the Montclair State University Institutional Review Board.
Results
Of the 442 study participants included in the analysis, 24.4% were non-Hispanic White, 35.5% were non-Hispanic Black, and 40.0% were Hispanic (Table 1). The mean (SD) age of participants was 37.2 (12.2) years. Non-Hispanic Black women (mean [SD] age, 39.6 [13.1] y) were significantly older than both Hispanic (mean [SD] age, 36.0 [11.9] y; P = .02) and non-Hispanic White (mean [SD] age, 35.9 [10.7] y; P = .04) women. Fewer than half of participants (40.7%) earned <$8000 per year; non-Hispanic Black women were most likely to report earning <$8000 per year (P < .001). Most women (65.8%) had ≤high school diploma. Most participants were unmarried at the time of the interview (82.1%), although more Hispanic women reported being married/living as married (24.3%) than did non-Hispanic Black (10.8%) and non-Hispanic White (17.6%) women (P = .006). Most participants reported some form of health insurance at the time of interview (93.7%), and 90.5% reported having had health insurance within the past 2 years. Hispanic women were more likely to report being currently uninsured (11.4%) than their non-Hispanic Black (2.7%) and non-Hispanic White (3.1%) counterparts (P = .002).
Socioeconomic and health care access characteristics of low-income women aged 18-75 years with no history of cervical cancer, by race and ethnicity, New Jersey, 2013-2016 (N = 442) a
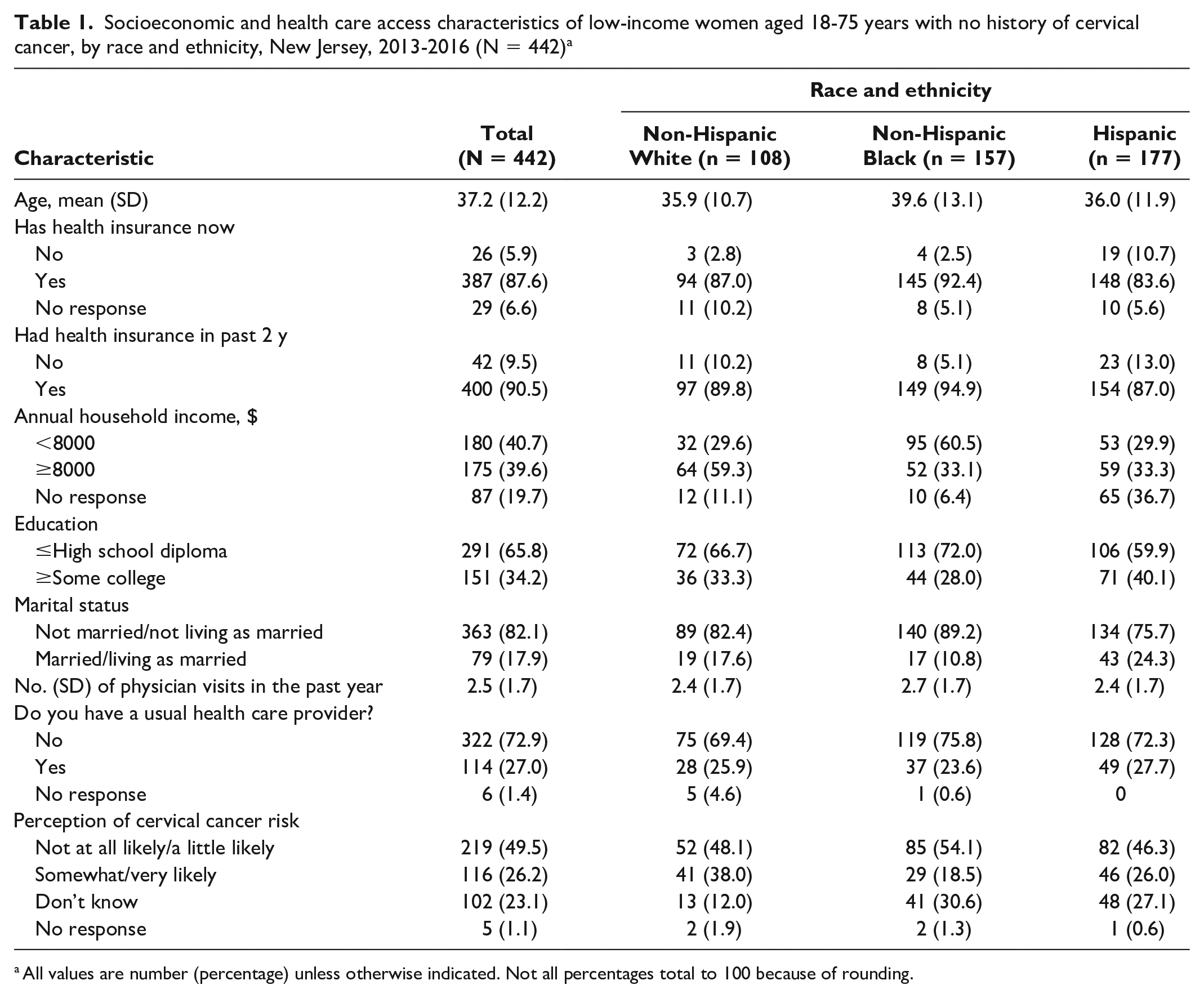
All values are number (percentage) unless otherwise indicated. Not all percentages total to 100 because of rounding.
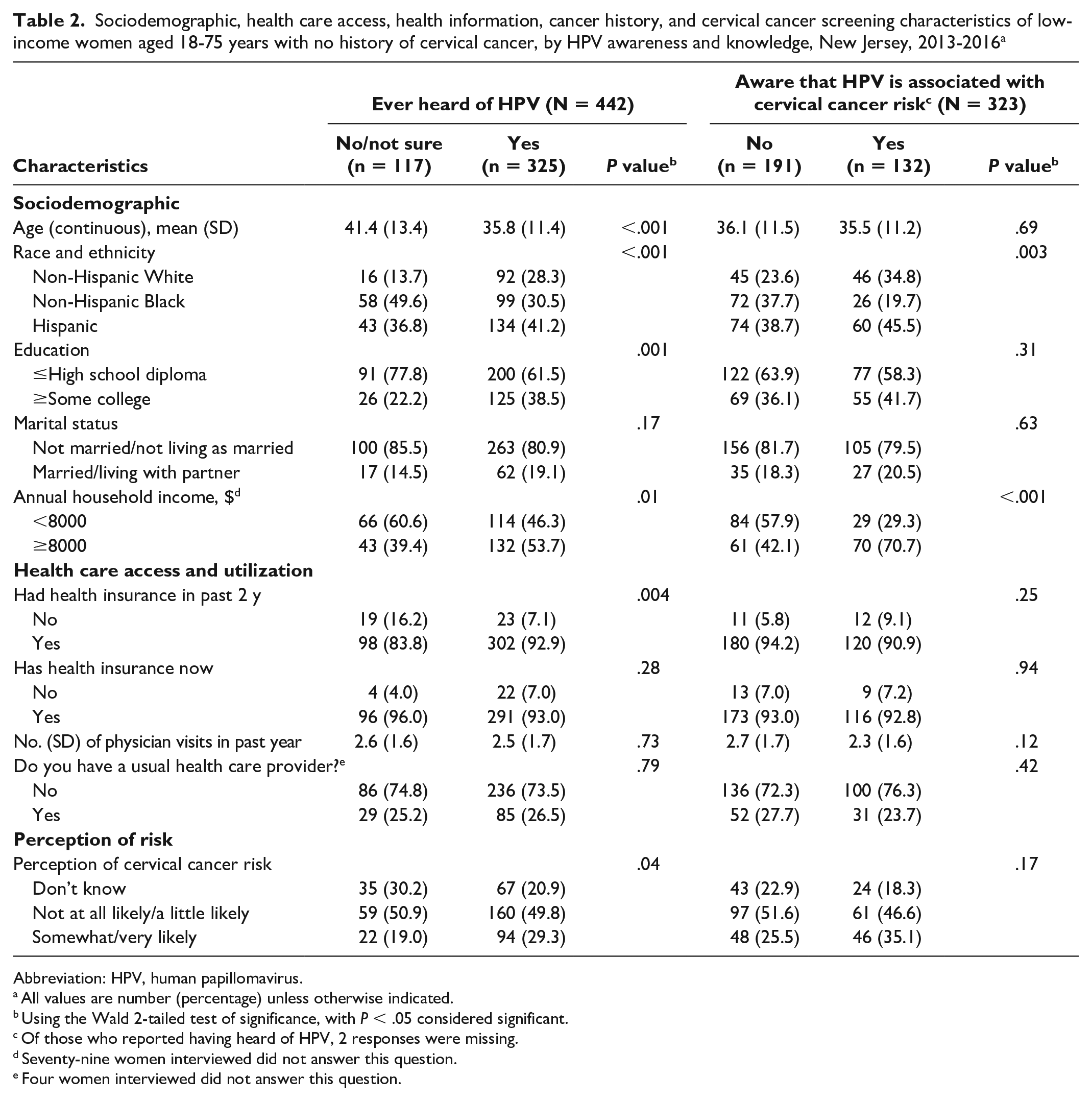
About one-quarter (26.5%) of study participants were unfamiliar with HPV (Table 2). Awareness of HPV varied by race and ethnicity, education, annual household income, and health insurance status. Women who had heard of HPV tended to be younger (mean [SD] age, 35.8 [11.4] y) than women who were unsure/had not heard of HPV (mean [SD] age, 41.4 [13.4] y; P < .001). Women who had heard of HPV were also more likely to report having completed ≥some college (38.5%) than women who had not heard of HPV (22.2%) (P = .001). While 7.1% of women who had heard of HPV lacked health insurance in the past 2 years, 16.2% of women who had not heard of HPV reported not having health insurance (P = .004).
Sociodemographic, health care access, health information, cancer history, and cervical cancer screening characteristics of low-income women aged 18-75 years with no history of cervical cancer, by HPV awareness and knowledge, New Jersey, 2013-2016 a
Abbreviation: HPV, human papillomavirus.
All values are number (percentage) unless otherwise indicated.
Using the Wald 2-tailed test of significance, with P < .05 considered significant.
Of those who reported having heard of HPV, 2 responses were missing.
Seventy-nine women interviewed did not answer this question.
Four women interviewed did not answer this question.
In addition, most women who had heard of HPV did not know it was associated with cervical cancer (59.1%) nor did they know it was a sexually transmitted infection (58.5%). This proportion also varied by race and ethnicity (Table 2). Of the 132 women who reported that they believed there was an association between HPV and cervical cancer, 19.7% (n = 26) were non-Hispanic Black women, compared with 34.8% (n = 46) who identified as non-Hispanic White and 45.5% (n = 60) as Hispanic (P = .002).
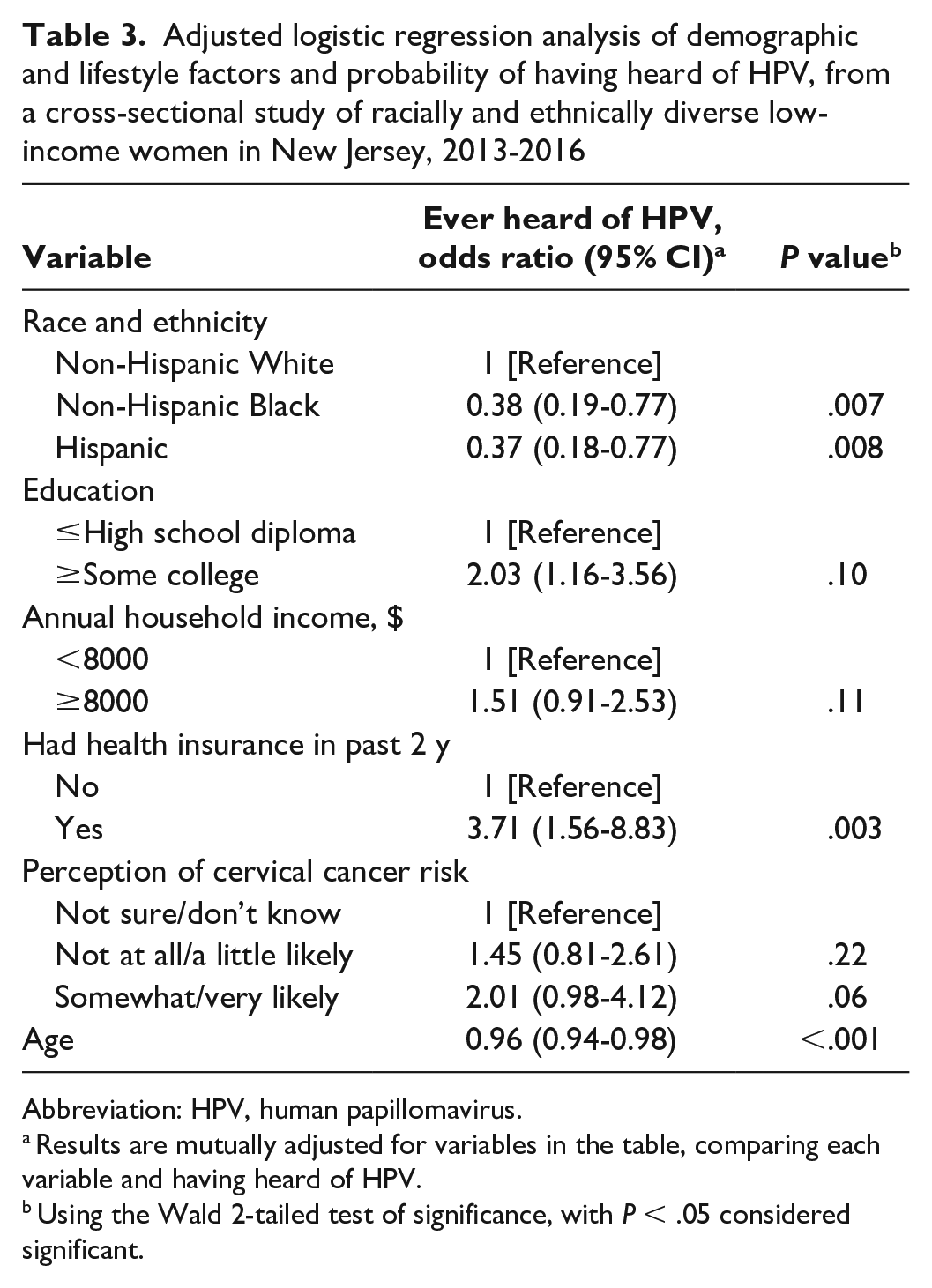
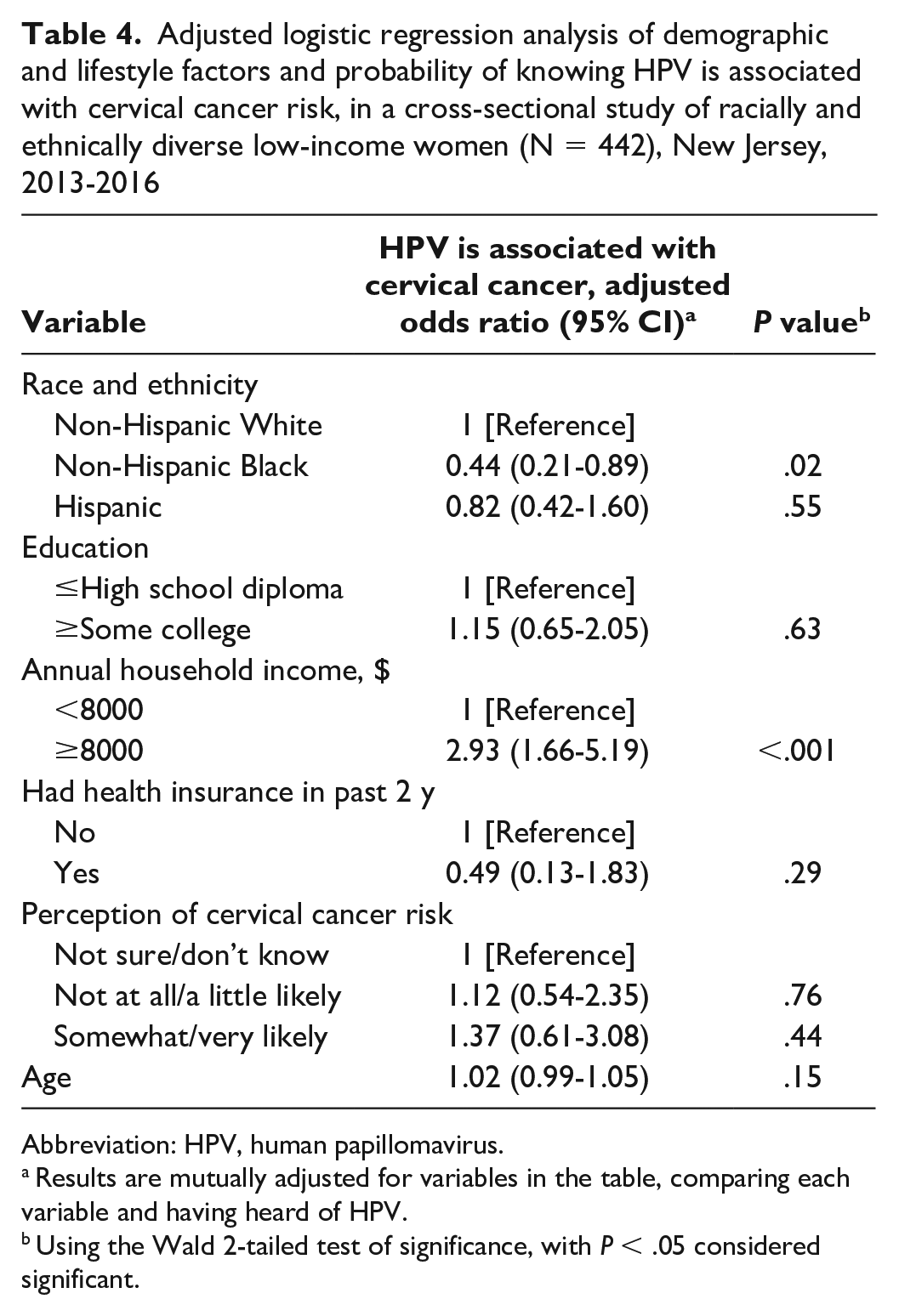
We used multivariate logistic regression models to examine the association between race and ethnicity and knowledge of HPV and the association between HPV and cervical cancer risk, with the most parsimonious models (Table 3) identified using backward selection. After adjustment for age, annual household income, education, and health insurance status, Hispanic and non-Hispanic Black women were less likely than non-Hispanic White women to report knowing about HPV (Hispanic OR = 0.37 [95% CI, 0.18-0.77]; non-Hispanic Black OR = 0.38 [95% CI, 0.19-0.77]), and women with ≥some college were more than twice as likely as women with ≤high school diploma to be aware of HPV (OR = 2.03; 95% CI, 1.16-3.56). Non-Hispanic Black women were also less likely than non-Hispanic White women to report knowledge of the association between HPV infection and cervical cancer risk (OR = 0.44; 95% CI, 0.21-0.89), and women with an annual household income of ≥$8000 per year were more likely than women with an income of <$8000 per year to be aware of this association (OR = 2.93; 95% CI, 1.66-5.19; Table 4).
Adjusted logistic regression analysis of demographic and lifestyle factors and probability of having heard of HPV, from a cross-sectional study of racially and ethnically diverse low-income women in New Jersey, 2013-2016
Abbreviation: HPV, human papillomavirus.
Results are mutually adjusted for variables in the table, comparing each variable and having heard of HPV.
Using the Wald 2-tailed test of significance, with P < .05 considered significant.
Adjusted logistic regression analysis of demographic and lifestyle factors and probability of knowing HPV is associated with cervical cancer risk, in a cross-sectional study of racially and ethnically diverse low-income women (N = 442), New Jersey, 2013-2016
Abbreviation: HPV, human papillomavirus.
Results are mutually adjusted for variables in the table, comparing each variable and having heard of HPV.
Using the Wald 2-tailed test of significance, with P < .05 considered significant.
Discussion
The results of this cross-sectional study provide evidence that low-income Hispanic and non-Hispanic Black women in New Jersey are less likely to report having heard of HPV than their non-Hispanic White counterparts. Furthermore, our study also suggests a disparity in knowledge in the association between HPV and cervical cancer risk. Specifically, among women who said they had ever heard of HPV, non-Hispanic Black women were less likely than non-Hispanic White women to know about the association between HPV and cervical cancer risk. This study also suggests that awareness of HPV varies by demographic characteristics.
Disparity in General Knowledge of HPV
Our finding that 26.5% of study participants were unfamiliar with HPV is in keeping with the current literature. Previous studies have reported rates of HPV knowledge ranging from 60% 19 to 75%. 20 Some of the variation in these findings can be attributed to differences in the study populations. While our study focused on low-income non-Hispanic White, non-Hispanic Black, and Hispanic women, McBride and Singh analyzed data from a national sample, 19 and Sherman et al surveyed college students. 20
While the overall study population reflects a comparable rate of HPV knowledge, disparities persist in HPV knowledge related to race and ethnicity. Our study found that non-Hispanic Black and Hispanic women were less likely to report ever having heard of HPV than non-Hispanic White women. McBride and Singh likewise reported a significant and inverse association with knowledge of HPV among Black participants compared with White participants 19 ; however, they found no significant difference between Hispanic and non-Hispanic participants, although this finding could be the result of their low response rate. The authors’ assessment of race and ethnicity differed from our study in that Hispanic ethnicity was asked separately from race; thus, participants in their study could identify as both White and Hispanic or Black and Hispanic. In addition, compared with our study participants, most of their study participants were White, had some college education, were employed, did not have children, and reported higher household incomes. 19 This topic warrants additional research to further explore general knowledge of HPV among racial and ethnic minority groups, as findings may differ within demographic groups, such as by SES or education level.
Disparities in Cervical Cancer Knowledge
Our study further found that non-Hispanic Black and Hispanic women were significantly less likely than non-Hispanic White women to report knowing HPV was associated with an increased risk of cervical cancer. A systematic review conducted by Kim and Han 21 identified 9 studies that indicated an association between health literacy and cervical cancer screening behaviors, 4 of which found that high levels of health literacy were associated with cervical cancer knowledge.22-25 Furthermore, national data from the Health Information National Trends Survey found a significant negative association between self-reported Black race and general HPV knowledge but did not find differences by race in cervical cancer knowledge. 19 Two important differences should be noted. First, the analysis by McBride and Singh included both male and female participants. Furthermore, our study population is not representative of the general population and differs from participants in the study by McBride and Singh, who tended to be older, more educated, and wealthier. Our study also included a greater proportion of non-Hispanic Black and Hispanic participants than did the McBride and Singh study, suggesting that studies using national samples may not reflect the unique experiences of low-income non-Hispanic Black and Hispanic women.
Disparities in Demographic Characteristics
Awareness of HPV also varied by race and ethnicity, education, annual household income, and health insurance status. Our findings suggest that educational attainment contributed to differences in HPV knowledge between those who had more than a high school diploma and those who did not. This finding is supported by current and previous literature,19,26 which confirms that HPV knowledge varies by demographic factors, and these differences should be considered in future studies.
Furthermore, differences resulting from current health insurance status warrant further exploration of health insurance status as it relates to HPV knowledge. Women who self-identified having health insurance in the past 2 years were more likely to have ever heard of HPV than women who were uninsured. Interestingly, limited research has examined health insurance status and knowledge of HPV in general. While McBride and Singh note the importance of sociodemographic variables influencing differences in HPV knowledge, they do not report health insurance status in their results. 19 However, research suggests that health insurance status influences HPV vaccination rates (ie, having health insurance is positively associated with HPV vaccination rates). 27
Limitations
This study had several limitations. First, although we sought to maximize participation in several ways, including by recruiting and completing interviews at scheduled SNAP-Ed/EFNEP classes and offering compensation for participation, all cross-sectional studies are susceptible to bias because of low response rates. In addition, given that this study focused on low-income participants by design, our study findings should be interpreted within that context. Second, we recruited participants solely from New Jersey; thus, our findings may not be generalizable to other states. Third, although diversity and variety exist in the lived experience of Latinas, we did not ask Latina participants about their or their families’ country of origin. Finally, although some studies have considered the role of stigma in HPV and sexually transmitted infections in Hispanic populations, these questions were not included in our study.
Conclusion
This study adds to the limited literature on HPV knowledge and cervical cancer risk among limited-resource populations. Given the disparities in cancer outcomes by race, ethnicity, and SES, our findings add to the overall understanding of HPV and knowledge of the association between HPV and cervical cancer risk. Our findings suggest a need to expand primary prevention efforts and develop culturally appropriate and tailored educational material to begin to address these disparities. Future studies conducted in low-income populations should explore additional avenues of recruitment methods, including reaching out to women who are experiencing extreme poverty through women’s shelters and other social service agencies, as well as further exploring the potential cultural influence on HPV knowledge and awareness as it relates to cervical cancer.
Footnotes
Acknowledgements
The authors thank Elisa V. Bandera, MD, PhD; Beth A. Jones, PhD, MPH; and Kitaw Demisse, MD, PhD, MPH, for their mentorship on this project. The authors also thank the many graduate students who assisted in data collection and geocoding of data. The authors are grateful to the research sites for introducing us to their clientele and to the study participants for sharing their lived experiences with us.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Cancer Institute Career Development Award (1K01CA157690).