
Abstract
Objective:
There is increasing recognition that cardiovascular disease (CVD) risk factors vary by Asian subgroups. We examined CVD risk factor prevalence among Vietnamese adults in a northern California health plan.
Methods:
We used electronic health record data to examine smoking, overweight/obesity (body mass index ≥23.0 kg/m2), obesity (body mass index ≥27.5 kg/m2), prediabetes, diabetes, and hypertension among middle-aged (n = 12 757; aged 45-64 years) and older (n = 3418; aged 65-84 years) Vietnamese adults, including 37.8% whose preferred language was Vietnamese. Findings were compared with East Asian adults.
Results:
Current smoking prevalence was 20.3% for middle-aged men, 7.0% for older men, and <1% for women in both age groups. Obesity prevalence was 12.0% for older men, 17.9% for middle-aged men, and 10% for women in both age groups. Among middle-aged men and women, 20.9% and 17.0% had hypertension and 13.5% and 8.5% had diabetes, respectively. Among older men and women, 64.0% and 60.0% had hypertension and 32.8% and 29.3% had diabetes, respectively. In both age groups, Vietnamese language preference was associated with higher risk of smoking (men only) and of diabetes and hypertension (women only). Compared with East Asian adults, Vietnamese adults had lower obesity prevalence but similar prevalence of diabetes, prediabetes, and hypertension. Vietnamese men were more likely and Vietnamese women less likely than East Asian adults to be current smokers.
Conclusions:
Study results suggest that more research on health conditions, lifestyle, and social factors among Vietnamese American adults is needed to develop culturally competent interventions to reduce CVD risk in this growing ethnic group.
Heart disease is the second leading cause of death among Asian American adults. 1 However, because data pertaining to Asian American health are often aggregated, ethnic differences in health challenges faced by distinct Asian subgroups may not be fully appreciated. 2 There is increasing recognition that cardiovascular disease (CVD) risk factors and modifiable health behaviors vary by Asian ethnic subgroups.2 -4 A greater understanding of these attributes within population subsets can inform research, public health policy, and clinical practice relevant to the ethnic and cultural needs of a specific population.
One important but relatively understudied Asian subgroup is the Vietnamese American population, currently composing the fourth-largest Asian subgroup in the United States. According to the 2010 US Census, more than half of all Vietnamese American people reside in the western United States, with the vast majority in California. 5 In comparison with other Asian American subgroups, the Vietnamese population shares an immigration history that largely began after the mid-1970s. Now more than 40 years later, an opportunity exists to examine generational attributes and unique sex differences among ethnic Vietnamese adults in health care settings. In this study, we used electronic health record (EHR) data for Vietnamese plan members aged 45-84 years who were part of an Asian cohort in a large northern California health plan designed to investigate the prevalence of CVD risk factors and other health-related characteristics. 2 We examined differences in risk factor prevalence by age group (middle-aged and older adults), sex, and preferred language. We then compared the prevalence of age-standardized risk factors among Vietnamese women and men with previously reported estimates for East Asian ethnic groups from the same source cohort. 2
Methods
Study Population
Kaiser Permanente Northern California (KPNC) is an integrated health care delivery system that provides comprehensive medical care to >3 million adult members residing primarily in the San Francisco Bay and Greater Bay Area, Sacramento area, Silicon Valley, and Central Valley. This cross-sectional study used EHR data for 16 175 Asian adults (7552 women and 8623 men) aged 45-84 years who were members of KPNC for all 12 months of 2016 and who were classified as being Vietnamese based on ethnicity code in the EHR or information from member surveys (55.8%), Vietnamese language preference in the EHR (15.4%), or Vietnamese surname (28.8%) that did not overlap with a potential Chinese surname. We focused on adults aged 45-84 years because most older Vietnamese adults living in the United States were born outside the United States and arrived as refugees after the end of the Vietnam War in 1975 or through subsequent immigration pathways. This study was reviewed and approved by KPNC’s Institutional Review Board, which waived the requirement to obtain informed consent as allowed under {§46.116(d)}.
Study Variables
We created 2 smoking status variables, current smoker and ever smoker (current or former), based on documented tobacco use history from 2012-2016. 2 We calculated body mass index (BMI) from clinic-measured height and weight on the date closest to December 1, 2016. We determined overweight and obesity status using the Asian-specific BMI intervention thresholds (≥23.0 kg/m2 and ≥27.5 kg/m2, respectively) recommended by the World Health Organization. 6 Smoking status was available for 95% of the cohort and overweight/obesity status for 74%. We assigned diabetes status based on inclusion in the KPNC Diabetes Registry by 2016, as identified through inpatient and outpatient diagnoses, laboratory criteria, and diabetes pharmacotherapy.2,7 We assigned prediabetes based on having an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) 8 or International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) 9 outpatient or problem list visit code for prediabetes in 2015-2016 or a 2016 laboratory value in the prediabetes range (glycated hemoglobin A1c 5.7%-6.4% or fasting glucose 100-125 mg/dL) and noninclusion in the Diabetes Registry by December 31, 2016. We assigned hypertension based on ICD-9 or ICD-10 outpatient or problem list visit code in 2015-2016. 2 Preferred language was the language indicated in the EHR as the plan member’s preferred language for oral communications related to their health care. Research suggests that English language acquisition can be used as a reasonable proxy for acculturation and assimilation. 10
Statistical Analysis
We performed all analyses using SAS version 9.4 (SAS Institute, Inc). We tabulated unadjusted prevalence estimates as point estimates and 95% CIs. We assessed differences by sex and age group using Pearson χ2 tests, with P < .05 used to determine significance. We examined the effect of Vietnamese preferred language versus English preferred language within the 4 age–sex groups using prevalence ratios produced from modified log-Poisson regression models that adjusted for age as a continuous variable. To compare health risks among Vietnamese adults aged 45-84 years with published results for 3 East Asian ethnic groups (Chinese, Korean, Japanese) in the same source cohort, 2 we produced age-standardized (to the 2016 US Census) prevalence estimates with 99% CIs using Proc Surveyreg models (SAS Institute, Inc) with weighting factors for 4 age groups (45-54 years, 0.3367; 55-64 years, 0.3261; 65-74 years, 0.2252; 75-84 years, 0.1120). Age-standardized prevalence estimates for obesity, diabetes, and hypertension among Chinese, Korean, and Japanese American adults were previously reported, 2 but we provided new estimates for overweight or obesity and prediabetes or diabetes.
Results
Among 16 175 Vietnamese American adults, the mean age was 56.8 (SD, 9.3) years, and about three-fourths were middle-aged (aged 45-64 years). More than half (59.3%) indicated English as their preferred language in the EHR (a greater percentage among men than among women), with the remainder listing Vietnamese (37.8%) or other Southeast Asian or Chinese (1%) language (Table 1). Middle-aged adults were significantly more likely than older adults (aged 65-84 years) to indicate English as their preferred language (62.6% vs 46.7%,). Accordingly, the mean [SD] age of plan members who preferred English was lower than the mean [SD] age of plan members who preferred Vietnamese (women, 55.3 [8.5] vs 58.8 [9.9] years; men, 55.6 [8.6] vs 59.4 [9.9] years; P < .001).
Age and language characteristics of a Vietnamese American adult cohort (N = 16 175), by sex, Kaiser Permanente Northern California, 2016 a
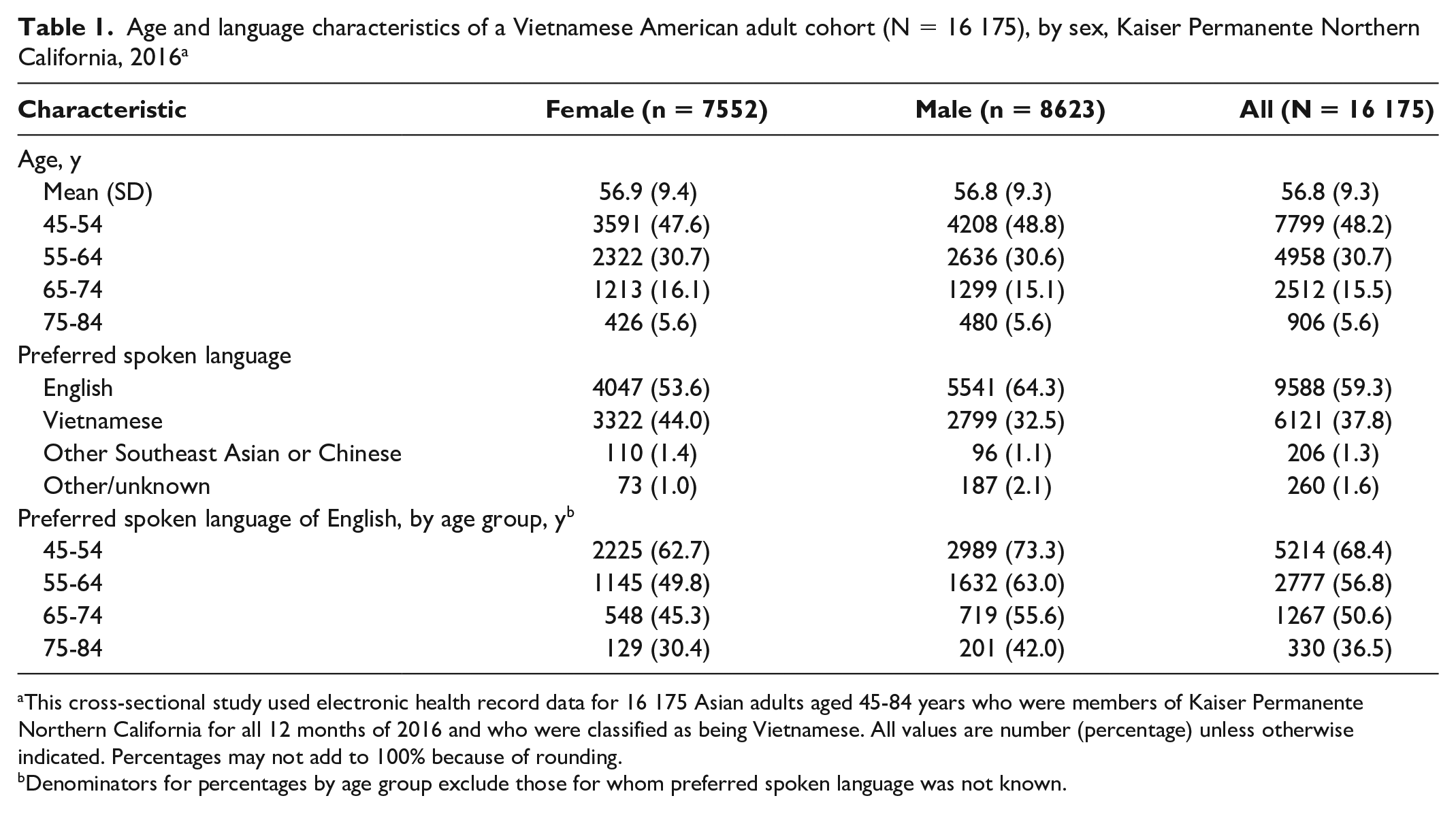
This cross-sectional study used electronic health record data for 16 175 Asian adults aged 45-84 years who were members of Kaiser Permanente Northern California for all 12 months of 2016 and who were classified as being Vietnamese. All values are number (percentage) unless otherwise indicated. Percentages may not add to 100% because of rounding.
Denominators for percentages by age group exclude those for whom preferred spoken language was not known.
Prevalence of CVD Risk Factors
The prevalence of current smoking was <1% among women in both age groups, 7.0% among older men, and 20.3% among middle-aged men, but ≥45% of men had a history of smoking (Table 2). Nearly half of women and >60% of men in both age groups were classified as overweight or obese; in both age groups, men were more likely than women to be classified as overweight or obese. However, the prevalence of obesity was relatively low (10%-12%) among women and older men and higher among middle-aged men (17.9%) compared with the other groups. In both age groups, the prevalence of diabetes, prediabetes/diabetes, and hypertension was also higher among men than among women. The prevalence of prediabetes and diabetes combined was more than 3 times higher than the prevalence of diabetes among middle-aged adults and more than twice as high among older adults.
Prevalence of CVD risk factors, by age group and sex, in a Vietnamese American adult cohort (N = 16 175), Kaiser Permanente Northern California, 2016 a
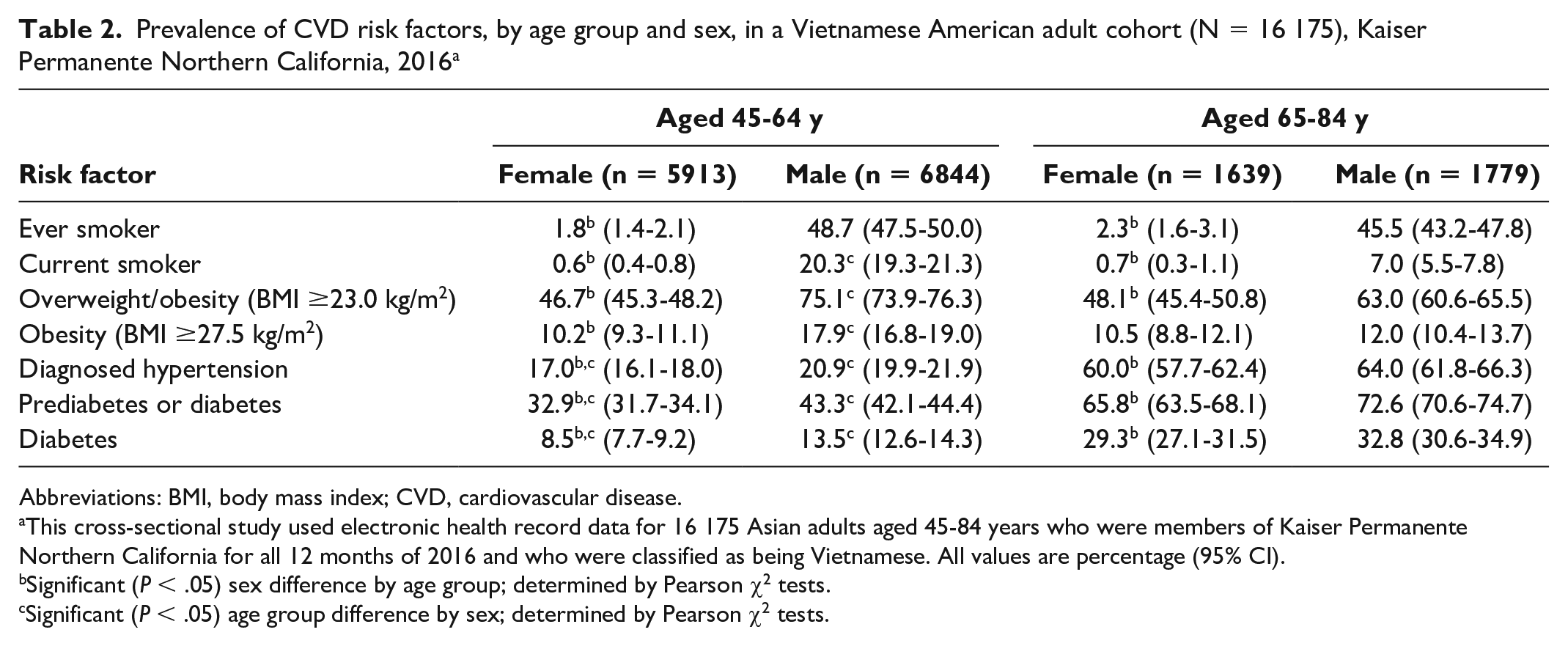
Abbreviations: BMI, body mass index; CVD, cardiovascular disease.
This cross-sectional study used electronic health record data for 16 175 Asian adults aged 45-84 years who were members of Kaiser Permanente Northern California for all 12 months of 2016 and who were classified as being Vietnamese. All values are percentage (95% CI).
Significant (P < .05) sex difference by age group; determined by Pearson χ2 tests.
Significant (P < .05) age group difference by sex; determined by Pearson χ2 tests.
Differences by Preferred Language
In unadjusted analyses that compared the prevalence of CVD risk factors by spoken language preference, we found the most notable differences among men. Specifically, compared with men who preferred to speak English, men who preferred to speak Vietnamese had a higher prevalence of current smoking (middle-aged, 26.6% vs 17.3%; older aged, 8.3% vs 5.3%) and ever smoking (middle-aged, 60.5% vs 43.4%). In both age groups, men with a Vietnamese language preference had a higher prevalence of hypertension, and among middle-aged men, those with a Vietnamese language preference had a higher prevalence of diabetes and prediabetes/diabetes and a lower prevalence of obesity. Compared with women with an English language preference, women with a Vietnamese language preference in both age groups had a higher prevalence of hypertension, diabetes, and prediabetes/diabetes. In addition, middle-aged women with a Vietnamese language preference had a lower prevalence of ever smoking and older-aged women with a Vietnamese language preference had a higher prevalence of obesity.
Because language preference differed by age, we examined the prevalence ratio of all 5 CVD risk factors by language preference after additionally adjusting for age within age group (Table 3). Vietnamese language preference was associated with a higher prevalence ratio of being a current or ever smoker among men in both age groups and a lower prevalence ratio of being an ever smoker among middle-aged women. Vietnamese language preference was associated with a lower prevalence ratio of obesity among middle-aged men and a higher prevalence ratio of obesity among older women. A preference for Vietnamese language was also associated with higher prevalence ratios for diabetes and hypertension among women in both age groups, for prediabetes/diabetes among middle-aged women and men, and for hypertension among older-aged men.
Prevalence ratios for CVD risk factors among adults who prefer to speak Vietnamese compared with English, by sex and age group, in a Vietnamese American adult cohort (N = 16 175), Kaiser Permanente Northern California, 2016 a
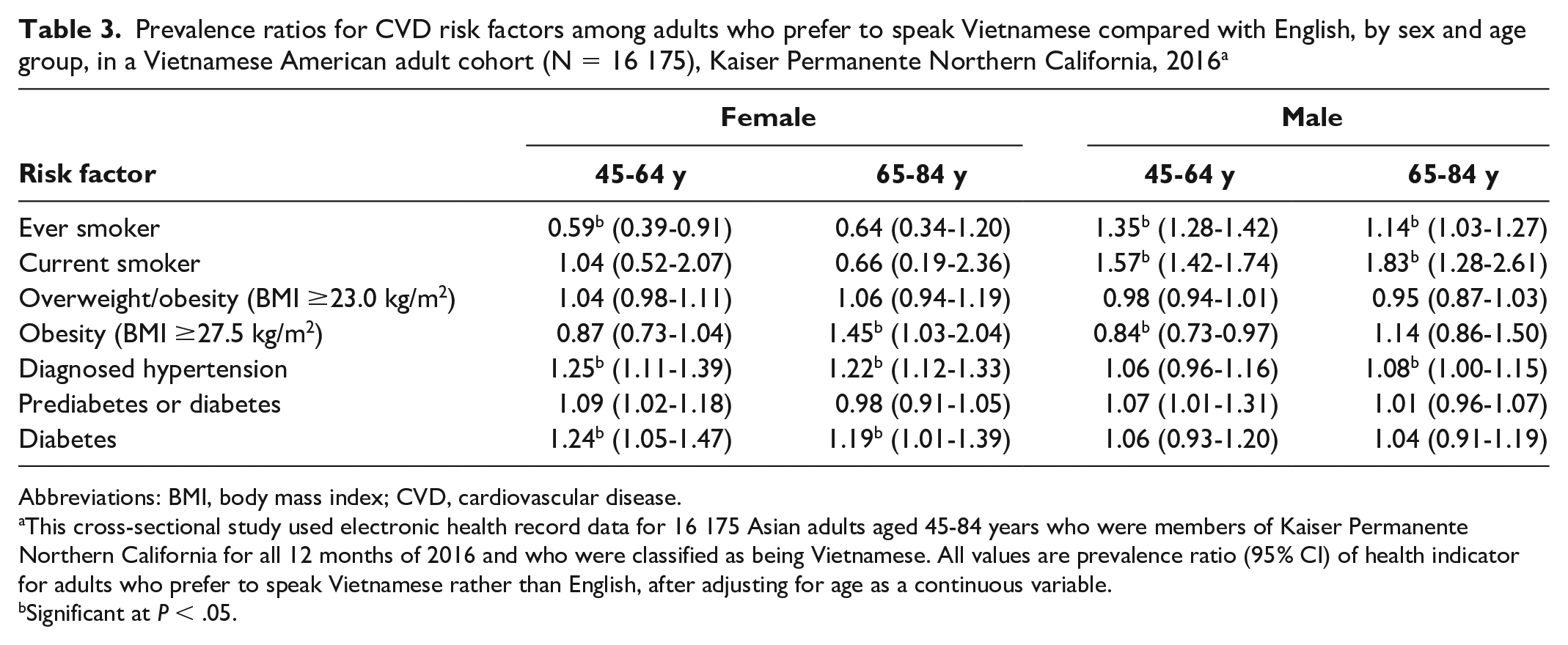
Abbreviations: BMI, body mass index; CVD, cardiovascular disease.
This cross-sectional study used electronic health record data for 16 175 Asian adults aged 45-84 years who were members of Kaiser Permanente Northern California for all 12 months of 2016 and who were classified as being Vietnamese. All values are prevalence ratio (95% CI) of health indicator for adults who prefer to speak Vietnamese rather than English, after adjusting for age as a continuous variable.
Significant at P < .05.
Age-Standardized Prevalence Estimates for Vietnamese and East Asian Adults
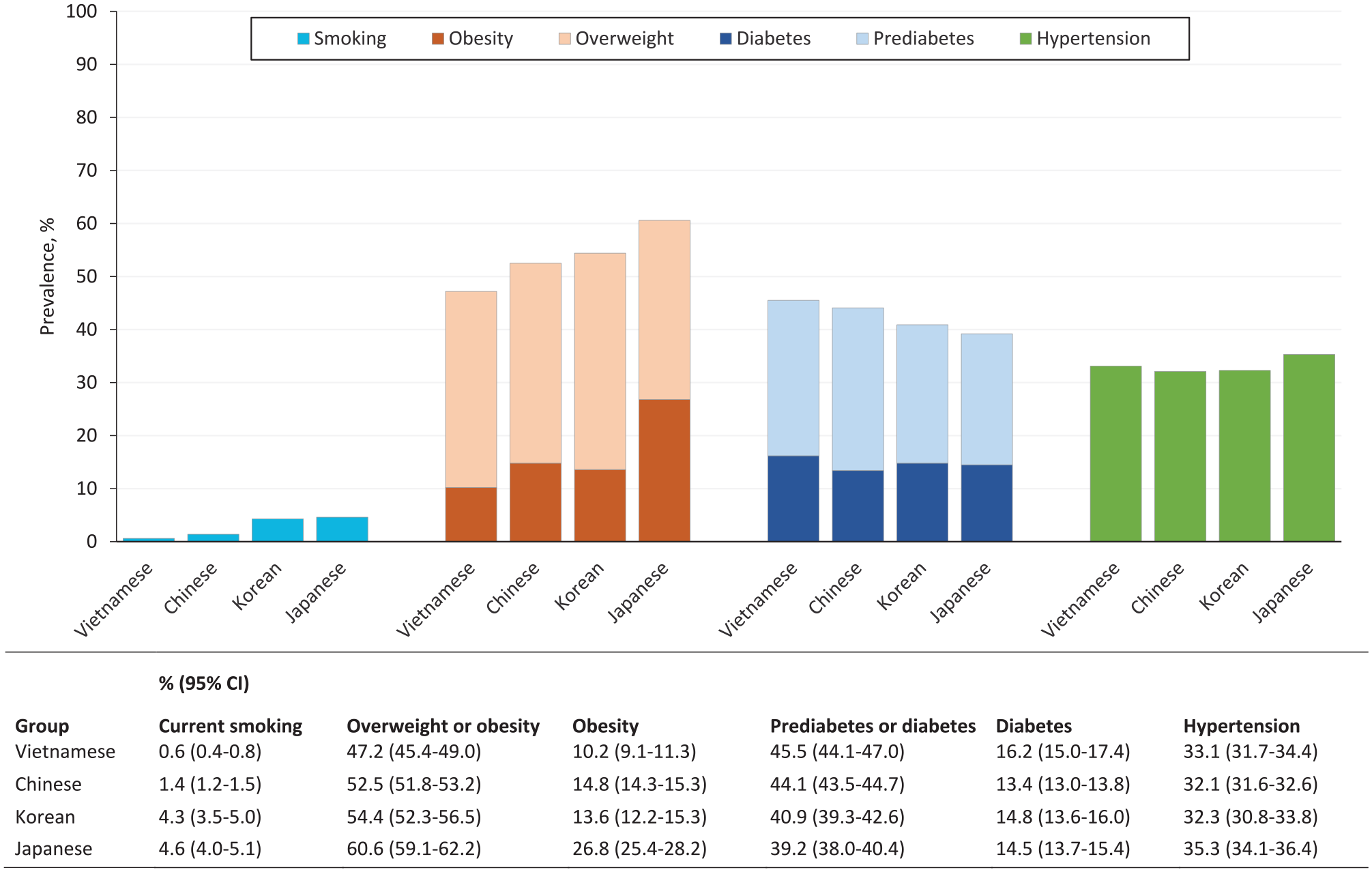
The prevalence of current smoking among Vietnamese men was significantly higher than among men in the East Asian groups (Figure 1), whereas the prevalence of current smoking was significantly lower among Vietnamese women than among East Asian women (Figure 2). The prevalence of obesity and overweight/obesity was significantly lower among Vietnamese adults than among the other East Asian groups. The prevalence of diabetes among Vietnamese adults was higher than among Chinese adults but similar to that among Korean and Japanese adults. The prevalence of prediabetes or diabetes was higher among Vietnamese men than among the other East Asian groups, but among women, was similar to that among Chinese adults and higher than among Korean and Japanese adults. Hypertension prevalence among Vietnamese women was similar to that among women in the other East Asian groups, whereas prevalence among Vietnamese men was similar to that of Chinese and Korean men but lower than among Japanese men.
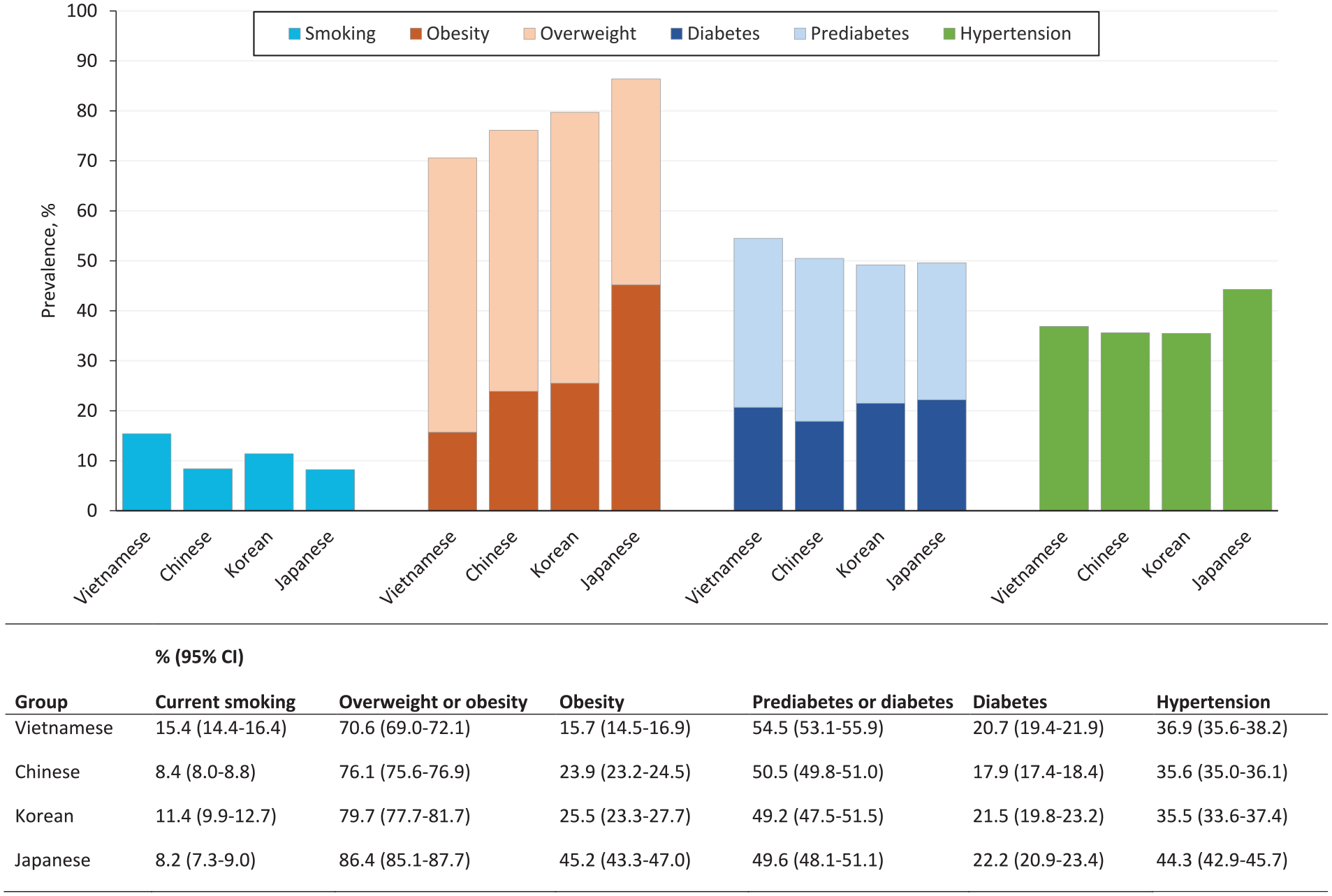
Age-standardized prevalence of cardiovascular disease risk factors among Vietnamese American men aged 45-84 years and East Asian ethnic groups. Data on smoking, obesity, diabetes, and hypertension for Chinese, Korean, and Japanese American adults were previously reported. 2 Data for Vietnamese American adults and for overweight/obesity and prediabetes/diabetes were not previously reported. Data source: electronic health record data for 16 175 Asian adults aged 45-84 years who were members of Kaiser Permanente Northern California for all 12 months of 2016 and who were classified as being Vietnamese.
Age-standardized prevalence of cardiovascular disease risk factors among Vietnamese American women aged 45-84 years and East Asian ethnic groups. Data on smoking, obesity, diabetes, and hypertension for Chinese, Korean, and Japanese American adults were previously reported. 2 Data for Vietnamese American adults and for overweight/obesity and prediabetes/diabetes were not previously reported. Data source: electronic health record data for 16 175 Asian adults aged 45-84 years who were members of Kaiser Permanente Northern California for all 12 months of 2016 and who were classified as being Vietnamese.
Discussion
In our study of middle-aged and older Vietnamese adult members of a northern California health plan, we found that compared with women, men in both age groups had a significantly higher prevalence of diabetes, prediabetes, hypertension, and current and ever smoking. Based on the lower Asian intervention thresholds for overweight and obesity, men in both age groups were more likely than women to be overweight or obese, but we observed significant differences by sex in obesity prevalence only in the middle-aged group. Although the prevalence of current and ever smoking and the prevalence of overweight and obesity were similar across age groups for women, men in the middle-aged group were more likely than men in the older age group to be overweight, obese, and current smokers, while not differing in history of smoking. The overall high prevalence of smoking and weight-related risk factors among middle-aged Vietnamese men highlights a need for aggressive outreach, assessment, and intervention in this subgroup to decrease risk of progression to cardiometabolic conditions and CVD.
A comparison of the age-standardized prevalence estimates for Vietnamese men and women aged 45-85 years with those of other East Asian ethnic groups in the same source cohort 2 showed that although Vietnamese adults had a lower prevalence of obesity and overweight/obesity than East Asian adults, they did not differ in the prevalence of diabetes and hypertension. This finding is consistent with other studies suggesting that Vietnamese people have obesity-related medical problems at a lower BMI threshold than usual standards11,12 and underscores the importance of addressing these CVD risk factors in nonobese Vietnamese adults in primary care practice. Our study also adds to the growing literature examining CVD risk prevalence among different Asian subgroups,2,13 in which heterogeneity in CVD mortality has also been reported. 3
Previous research has identified an adverse effect of acculturation to Westernized lifestyles among Asian American adults who live in the United States, that is, adoption of diets higher in processed foods and fat and lower in fruits and vegetables, coupled with less physical activity. 14 Similar trends have been noted in Vietnam as well, where increases in the prevalence of diabetes, obesity, and hypertension have been observed during the past decade, likely because of economic growth.15,16 These findings suggest that social and dietary factors may play an important role in the development of hypertension and diabetes even in the absence of obesity. Although we did not observe consistent differences in obesity prevalence by language preference, modest differences in the risk of hypertension and diabetes by language preference were evident, especially among women.
Our comparisons of current smoking prevalence among Vietnamese men and men of various East Asian subgroups highlight that smoking cessation should remain an important focus for preventive health interventions for Vietnamese men, especially for middle-aged and younger age groups. Other studies of Vietnamese men have also shown high rates of tobacco use.17 -19 Telephone survey data obtained in 2002-2005 from Vietnamese residents of Santa Clara County, California, demonstrated that 29.8% of Vietnamese men were current smokers (compared with 19.0% of non-Hispanic White men) and that among Vietnamese men, those who spoke Vietnamese were more likely to be current smokers than those who spoke English. 18 Because smoking is considered a socially desirable behavior by many younger and middle-aged adult Vietnamese men, 19 culturally tailored smoking prevention and cessation outreach efforts are needed, especially for less acculturated Vietnamese men with limited English proficiency, who in our study had significantly higher smoking prevalence than similarly aged English-speaking men. Because successful smoking cessation before older age can prevent development of cardiometabolic and cardiovascular conditions, helping smokers quit will be important for improving the health of Vietnamese adults. 20
Strengths
This study had several strengths. A major strength of our study was the use of EHR data for a large cohort of insured Vietnamese adults who lived in the same region of the United States and received care in the same integrated health care delivery system. Few studies focused on Vietnamese American adults have been conducted among insured health care populations where patients have equal access to care. As the Vietnamese population continues to grow, it is important to understand their health care attributes and needs in such settings to help direct programs focused on culturally responsive care and achieving health equity. With the large sample size of Vietnamese adults available for our analyses, we were able to disaggregate health risk profiles for middle-aged and older adults. Because we used EHR data, our prevalence estimates were not subject to low response rates and underrepresentation of limited English–proficient adults, as often happens with survey-based studies. In addition, we were able to put the CVD risk profile of Vietnamese men and women in context by comparing their risk profiles with those of East Asian ethnic groups.
Limitations
Our study also had some limitations. First, nearly 30% of our cohort was identified according to a combination of identification of Asian race in the EHR and Vietnamese surname rather than indication of Vietnamese ethnicity in the EHR. This categorization may have led to misclassification of some women, although we anticipate that only a small number of Asian women with a Vietnamese surname in this generation (average age, 55 years) would have been non-Vietnamese. Second, we did not have detailed information about country of origin, duration of residence in the United States, or individual socioeconomic characteristics (eg, income, education, and employment), which are not routinely captured in EHR fields. We also lacked information about acculturation and English language proficiency. Third, we did not examine hyperlipidemia/dyslipidemia or statin therapy because diagnosis and treatment vary according to underlying risk conditions, and we did not have complete data on pretreatment or screening lipid/lipoprotein levels. Fourth, we focused on clinically recognized hypertension and did not ascertain serial blood pressure measurements. Fifth, we lacked detailed information about smoking history, including number of years smoked, amount smoked, and, for noncurrent smokers, recency of quitting. Finally, our study was based on a cohort of insured adults who were members of a non–safety-net health plan in northern California and may not be generalizable to Vietnamese adult populations who receive care in safety-net clinics or who reside in other parts of the United States.
Conclusion
This study described the prevalence of CVD risk factors in a contemporary insured adult Vietnamese population in northern California and how risk factor prevalence differs by sex, age group, and preferred language. The persistently high prevalence of smoking among Vietnamese men, especially those who are likely first-generation immigrants, is consistent with findings published more than a decade earlier 18 and highlights the imperative of implementing culturally tailored public health and clinic-based smoking prevention and smoking cessation efforts to reduce smoking among younger Vietnamese men. Our finding that diabetes and hypertension prevalence among Vietnamese men and women was comparable to other East Asian groups, despite a lower prevalence of obesity, suggests a need for research focused on identifying dietary practices and other modifiable behavioral and social factors that may influence the development of diabetes and hypertension in this population. Such information is needed to develop and implement culturally competent public health outreach and patient education strategies that will promote cardiovascular health in this growing Asian ethnic group.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nirmala Ramalingam owns stock valued at <$20 000 in AbbVie, Inc, and previously owned stock in Takeda and Amgen.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Kaiser Permanente Northern California Region’s Community Health Program. The funder had no role in the design of the study; in the collection, analysis, and interpretation of the data; or in the writing or approval of the article.