
Abstract
SARS-CoV-2 has exposed limitations of public health mitigation measures such as traditional case investigations and contact tracing. The Whiteriver Service Unit is a rural, acute care hospital on the Fort Apache Indian Reservation in Arizona with integrated health care delivery and public health services. During the first wave of COVID-19 cases in May–June 2020, we developed an innovative case investigation contact tracing approach that relied heavily on cross-trained personnel, in-person encounters, and baseline clinical evaluations. A second COVID-19 surge during December 13, 2020–January 31, 2021, caused incidence to peak at 413 cases per 100 000 community members. During that second surge, we investigated all 769 newly identified COVID-19 cases and notified 1911 (99.4%) of 1922 reported contacts. Median time interval from nasopharyngeal specimen collection to both case investigation and contact notification was 0 days (range, 0-5 days and 0-13 days, respectively). Our primary lesson was the importance of cross-trained personnel who integrated tasks along the testing–tracing continuum (eg, in-person interviews, prompt referral for additional testing and evaluation). These successive steps fed forward to identify new cases and their respective contacts. Our innovative community-based approach was both successful and efficient; our experience suggests that when adapted based on local needs, case investigation and contact tracing remain valuable and feasible public health tools, even in rural, resource-limited settings.
SARS-CoV-2, the virus responsible for COVID-19, overwhelmed public health efforts across the country during much of 2020.1,2 Despite an increased contact tracing workforce, case counts consistently outstripped case investigation and contact tracing capacity. The failures of contact tracing to slow the spread and reduce morbidity of COVID-19 were often attributed to limited funding, poor planning, a lack of trained personnel, and variability in the application of other public health measures. 3 However, exclusively focusing on external factors or broader system failures misses an opportunity to address flaws inherent to this established public health tool. Existing recommendations for the structure and practice of contact tracing follow a traditional framework of delegating responsibilities across multiple roles held by separate individuals. 4 Such a framework is used in sexually transmitted infections and tuberculosis. 5 Yet this trusted approach is likely inadequate to contain a public health crisis on the scale and speed of the COVID-19 pandemic. The aforementioned challenges are exacerbated on American Indian reservations that tend to be rural and have less reliable access to transportation and telecommunication than the general population. 6
The Indian Health Service provides care to millions of American Indian people in the United States, many of whom have been disproportionately affected by COVID-197,8 and live on Tribal Lands in rural areas. 9 The Whiteriver Service Unit on the Fort Apache Indian Reservation is an integrated health care delivery and public health system that serves as both an acute care hospital and the local public health authority for approximately 18 000 American Indian people in eastern Arizona. Some of the highest reported COVID-19 incidence in the United States in May–July 2020 occurred in this public health jurisdiction. After the first COVID-19 case was detected in the Whiteriver Service Unit on April 1, 2020, incidence increased exponentially and peaked at 430 cases per 100 000 community residents in mid-June 2020. 10 We also noted a household transmission rate >80%, far greater than what had been previously described in the literature11-13 and commonly involving asymptomatic people.14,15 The rapidly increasing case counts in a community with multigenerational and often crowded homes—combined with a limited baseline capacity to manage the surge of cases and trace their contacts—compelled us to restructure our case investigation and contact tracing procedures.
During that first wave, we developed an innovative and integrated approach that relied heavily on cross-trained personnel enabled to conduct in-person encounters and provide in-home SARS-CoV-2 testing. A second COVID-19 surge during December 13, 2020–January 31, 2021, created an opportunity to examine performance metrics of this program and compare those metrics with published reports. Here, we describe the results of that performance review and discuss potential lessons learned. The Whiteriver Service Unit tracing program serves as a case study on the benefits of an integrated health care delivery and public health approach to case investigation and contact tracing.
Purpose
Three important features of the Whiteriver Service Unit case investigation and contact tracing program departed from common practice: integration of roles to prevent handoffs to various personnel among the testing–tracing continuum, an emphasis on in-person case investigation and contact tracing, and baseline clinical evaluations of all people with positive SARS-CoV-2 test results and their contacts at high risk for severe COVID-19.
First, we cross-trained personnel to combine roles that are usually distributed among individual team members. Field teams included public health nurses, health care staff members retrained for public health roles (eg, pharmacists, physical therapists, medical assistants), and volunteers from the community. Centers for Disease Control and Prevention guidance suggests that investigation of index cases and the tracing of their contacts be performed by separate people and that contacts be referred for testing rather than tested by the contact tracers themselves. 4 To improve the timeliness of identifying new cases and contacts, we sought to prevent this series of handoffs by cross-training personnel to integrate tasks. Each field team member took courses or passed competencies in case investigation, contact tracing,16,17 and collection of nasopharyngeal swab specimens, 18 along with standard privacy training, all of which were freely available online. New members underwent a short apprenticeship by shadowing seasoned tracers for 2 weeks. Twice-daily feedback during contact tracing rounds emphasized key differences in information collection between index case investigation and their associated contacts. Like many agencies across the country, the Whiteriver Service Unit could not add staff members easily or quickly enough to meet demands, so expanding the scope of each member was central to our response.
Second, the program defaulted to in-person encounters for all case investigation and contact tracing. Most public health agencies relied on telephone banks for contact tracing during the COVID-19 pandemic. However, the success of a telephone bank approach relies on public willingness to disclose personal information and provide contact information by telephone to strangers.3,19,20 Furthermore, the population served by the Whiteriver Service Unit has no consistent or reliable telecommunication access (either landline or cellular telephone). Contact tracers were either themselves members of the local community or paired with community members to navigate the Reservation. Although in-person activities require additional time, the hope was that an increased yield of investigations would subsequently yield a higher proportion of contacts successfully notified and tested.
The third distinct feature of the Whiteriver Service Unit’s approach was facilitated by our having a preexisting integrated health care delivery and public health system. We incorporated baseline clinical evaluations into routine case investigation and contact tracing activities. Our concern was that infection with SARS-CoV-2 can lead to objective illness in people who otherwise appear and self-report feeling well (ie, “happy hypoxia”). 21 Thus, the field team routinely collected resting and ambulatory vital signs (eg, heart rate, oxygen saturation levels) on all people at high risk for severe disease. For people meeting certain prespecified parameters, team members directly facilitated transportation to the emergency department for further evaluation.
To evaluate the efficiency and performance of our COVID-19 response, we examined data collected as part of routine case investigation and contact tracing operations.
Methods
For this performance review, we examined case investigation and contact tracing data from December 13, 2020, through January 31, 2021, a 7-week period during which local COVID-19 incidence was the highest it had been since June 2020, peaking at 413 cases per 100 000 people on January 6, 2021. 10 All investigated cases had received a positive test result for SARS-CoV-2 via molecular testing from nasopharyngeal swabs. We extracted de-identified information from case investigation sheets into a Microsoft Excel spreadsheet: age, sex, dates (of test, results, investigation), number of contacts reported, and, if known, epidemiologic link to a previous COVID-19 case. Information extracted on each reported contact included age, sex, success of contact notification (yes/no), and date of notification. Staff members maintained all information for both cases and contacts on hospital servers. All activities were a part of the Whiteriver Service Unit’s public health surveillance (45 CFR 46.102[l]) and were approved by the Phoenix Area Indian Health Service and Tribal Health Board.
Outcomes
We investigated 769 (100%) new COVID-19 cases during December 13, 2020–January 31, 2021 (Table 1). Median time interval from specimen collection to case investigation was 0 days (range, 0-5 days); 422 (54.9%) cases were investigated the same day the specimen was collected (day 0), and 686 (89.2%) cases were investigated by the end of the next calendar day (day 1). Using the alternative metric of positive test result, median time interval from receipt of positive test result to case investigation was 0 days (range, 0-5 days), with 486 (63.2%) investigated the same day of the test result (day 0) and 751 (97.7%) by the end of day 1. An epidemiologic link to a previous COVID-19 case could be identified in 567 (73.7%) cases.
Time to complete COVID-19 case investigations and notify contacts, Whiteriver, Arizona, December 2020–January 2021 a
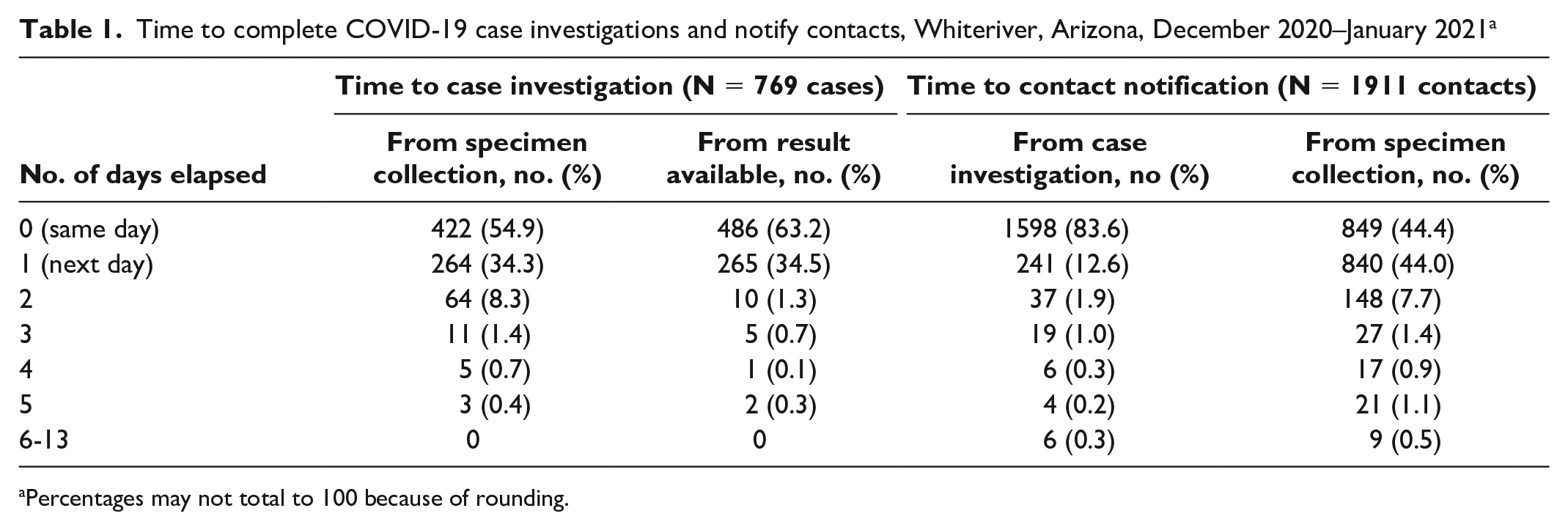
Percentages may not total to 100 because of rounding.
During case interviews, 302 (39.3%) people either denied having or refused to name contacts during their COVID-19 infectious period. Among the 467 people who did report contacts, 1922 unique contacts were reported (ie, mean of 4.1 contacts per case) (Table 2). Median time interval from case investigation to contact notification, as well as from case specimen collection to contact notification, was 0 days (range, 0-13 days). Among all 1922 named contacts, 1911 (99.4%) were traced and notified, 1839 (96.2%) by the end of the next calendar day (96.2%) (Table 1).
COVID-19 case investigation and contact tracing metrics in 3 states, 2020-2021
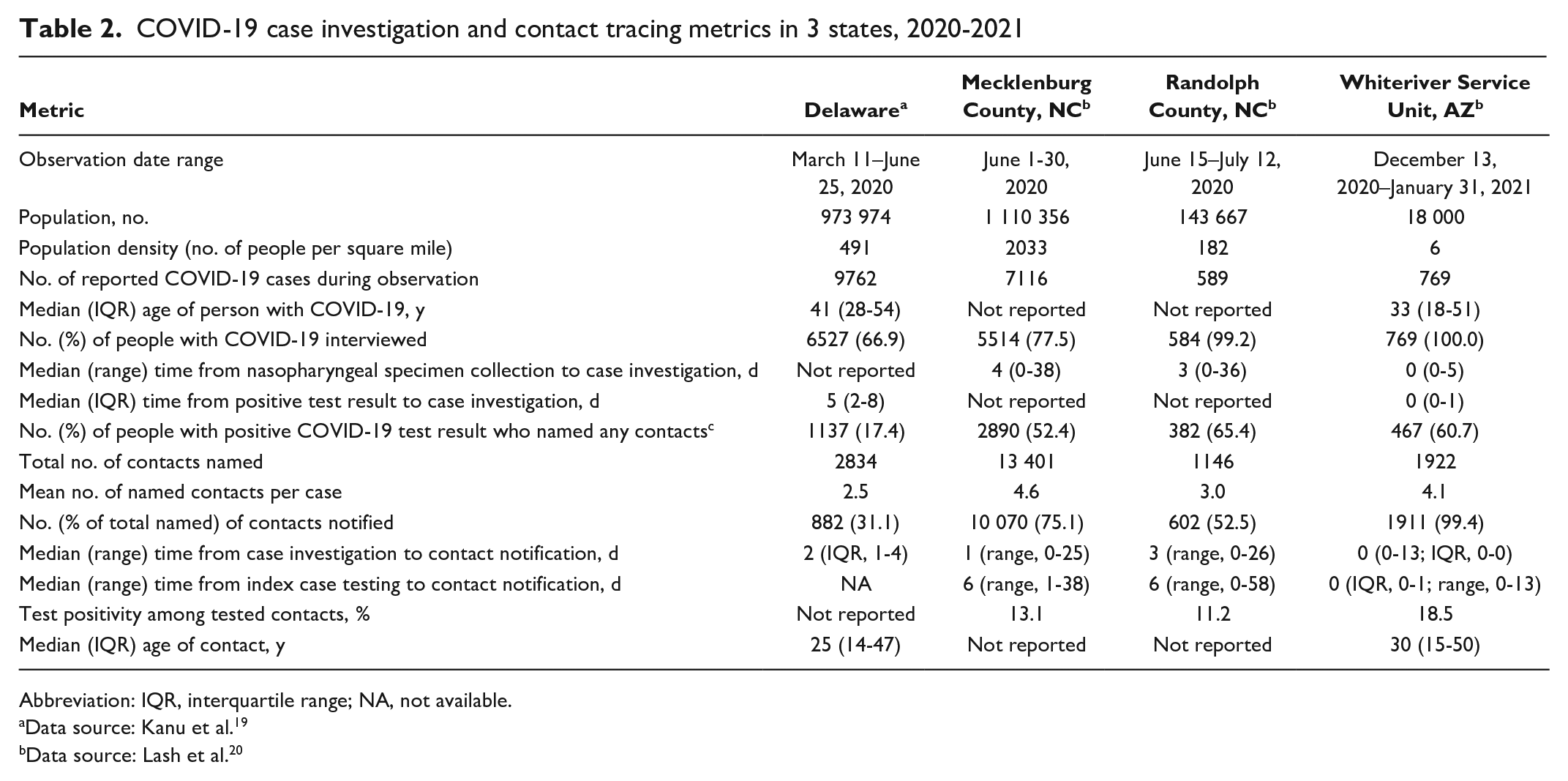
Abbreviation: IQR, interquartile range; NA, not available.
Data source: Kanu et al. 19
Data source: Lash et al. 20
Lessons Learned
Compared with what has been reported elsewhere,1,2,19,20,22 the Whiteriver Service Unit community experienced a higher COVID-19 incidence and test positivity, while achieving greater success and efficiency for both case investigations and contact notifications.
We compared our performance metrics with those previously reported in Delaware and North Carolina.19,20 The median time interval from specimen collection or result notification to case investigation in those reports was 3-5 days compared with our median of 0 days. This advantage was compounded by additional gains of several days in contact notification. The Whiteriver Service Unit was able to exceed the Harvard Global Health Institute recommendations for cases investigated (>90%), contacts notified (>90%), and time to investigation and notification (<24 hours). 23 Despite being situated in a low-resource setting, our efficient and effective contact tracing approach highlights the benefit of a health care delivery system that is well integrated with public health activities, as well as the value of having community members fully participating in the field teams. Our partnership with the local Tribe was vital and ensured that community volunteers were available to assist non-local staff members in navigating the reservation.
With the multiple steps along the testing–tracing continuum, timely implementation of each successive step forward helps to identify new cases and their respective contacts while there is still time for the isolation and quarantine interventions to be effective public health measures. Our ability to eliminate and minimize multiple handoffs along that continuum undoubtedly improved our efficiency of not only tracing contacts but also identifying new cases. Our observations also strongly support a strategy that pushes testing out to the community—specifically to the homes of cases and contacts—to support isolation and quarantine and to expedite the next round of investigations and tracings.
Initially, in-person activities and offering testing within homes might seem counterintuitive; concerns about resource efficiency and staff member safety likely led most other jurisdictions in the United States to rely on the broad implementation of telephone banks and mass testing sites for case investigation and contact tracing. Like many other health care settings, we also experienced shortages in personal protective equipment (PPE). However, all field staff members, including volunteers, were provided the same PPE fit-testing and training as hospital staff members; they also underwent additional donning and doffing training unique to field situations. Vehicles were equipped with ample PPE and testing materials for field visits as well as other supplies, including biohazard and trash bags.
Despite our timely case interviews, approximately 40% of interviewed people named no contacts during their COVID-19 infectious period. Nevertheless, that proportion might have been even higher had we used a slower process or relied on a telephone bank (ie, without the opportunity to meet in person to read body language and develop rapport).
We acknowledge that we benefited greatly from operating in a context in which hospital services and field teams were already accustomed to operating as one service unit. Use of the same electronic health record system, for example, facilitated immediate delivery of positive test results to the field team and allowed seamless referrals to the hospital. In addition, our integrated system allowed rapid cross-training and shifting of human resources to assist the outreach field teams. Point-of-care molecular testing platforms further expedited test result delivery; many patients were notified of their results and interviewed during the same clinical encounter during which the nasopharyngeal specimen was collected. Nevertheless, more than 60% of all the Whiteriver Service Unit’s SARS-CoV-2 positive test results originated from specimens collected by field team members who drove them back to our laboratory.
A limitation of this case study was the lack of information on symptomatology and proportions of tested contacts. Investment in tracing applications might improve our ability to more comprehensively evaluate future efforts. Second, some might argue that the experience of an integrated health care delivery and public health system that exclusively serves an American Indian population in rural Arizona may not be generalizable. However, our unique circumstances add import to our successful efforts. We would suggest that an integrated system with combined roles among multidisciplinary staff members who are committed to implementing a field-based approach is worth considering. Such an approach might address some of the case investigation and contact tracing failings experienced across other parts of the country.
Successful contact tracing is possible. Public health agencies may need to reimagine case investigations and contact tracing in their respective jurisdictions, not only in response to COVID-19 but to prepare for future pandemics. Success requires working with local community partners to learn from the recent COVID-19 experience and to reimagine how to respond to future public health threats. Our assessment suggests that an integrated field-based tracing program that continuously feeds forward along the testing–tracing continuum works for a rapidly moving respiratory epidemic such as COVID-19. In addition, as SARS-CoV-2 will remain with us for the foreseeable future, an opportunity exists to reimagine, and realize, the potential of contact tracing for preventing COVID-19–related morbidity and mortality.
Footnotes
Acknowledgements
The authors thank the White Mountain Apache Tribe’s Emergency Operations Center and Community Health Representatives, Johns Hopkins Center for American Indian Health, Mark A. Veazie, DrPH, of Phoenix Area Indian Health Service, and Georgina Peacock, MD, MPH, of the Centers for Disease Control and Prevention.
Disclaimer
The content does not represent the opinions of the Indian Health Service or other affiliated institutions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.