
Abstract
Objectives:
The Ending the HIV Epidemic (EHE) initiative prioritizes treatment and prevention efforts in counties where most new HIV diagnoses occur and states with substantial incidence of new HIV diagnoses in rural areas. Understanding the characteristics of adults with HIV living in EHE priority areas, and how these characteristics compare with adults with HIV living in non–EHE priority areas, can inform EHE efforts.
Methods:
We analyzed data from the 2018 Medical Monitoring Project (MMP) to understand the characteristics of adults with HIV living in 36 of 48 EHE priority counties; San Juan, Puerto Rico; and 1 of 7 EHE priority states. We calculated weighted percentages of sociodemographic characteristics, behaviors, and clinical outcomes of adults with diagnosed HIV living in MMP EHE priority areas and compared them with characteristics of adults who did not live in MMP EHE priority areas using prevalence ratios (PRs) with predicted marginal means.
Results:
Living in an MMP EHE priority area was more common among adults who were non-Hispanic Black or Hispanic, experienced homelessness, or were food insecure compared with adults who were non-Hispanic White (59.3% and 58.4% vs 41.0%), not experiencing homelessness (60.9% vs 51.9%), or not food insecure (59.8% vs 51.0%). Adults who lived in MMP EHE priority areas were significantly less likely to be adherent to their HIV medications (PR = 0.95; 95% CI, 0.91-0.99) and durably virally suppressed (PR = 0.94; 95% CI, 0.91-0.97), and more likely to miss scheduled appointments for HIV care (PR = 1.31; 95% CI, 1.10-1.56) than adults who did not live in MMP EHE priority areas.
Conclusion:
To increase viral suppression and reduce HIV transmission, it is essential to strengthen public health efforts to improve medication and appointment adherence in this population.
During 2018, an estimated 1.2 million people in the United States aged ≥13 years were living with HIV, and there were an estimated 36 400 new HIV infections. 1 The estimated incidence of HIV infection remained stable from 2014 to 2018. The number of new HIV diagnoses rose by 6% among adults aged 25-34 years from 2014 to 2018, and non-Hispanic Black and Hispanic people accounted for 69% of new HIV diagnoses in 2018. 2 In 2019, the US Department of Health and Human Services launched an initiative, Ending the HIV Epidemic (EHE): A Plan for America, to prioritize treatment and prevention efforts in areas with a high number of new HIV diagnoses and where HIV transmission occurs most frequently. 3 EHE priority areas include 48 counties; Washington, DC; and San Juan, Puerto Rico, where most new HIV diagnoses occur, as well as 7 states (Alabama, Arkansas, Kentucky, Mississippi, Missouri, Oklahoma, and South Carolina) with substantial new HIV diagnoses in rural areas. 4 EHE focuses on 4 key strategies: diagnose, treat, prevent, and respond. The “treat” pillar emphasizes treating “HIV infection rapidly after diagnosis and effectively in all people who have HIV, to help them get and stay virally suppressed.” 3 Thus, to reduce HIV transmission, understanding sociodemographic characteristics, behaviors, and clinical characteristics of adults with diagnosed HIV living in EHE priority areas, and how they differ from adults not living in EHE priority areas, can inform EHE treat pillar efforts by identifying key areas for tailored interventions to improve outcomes and achieve the goals of EHE.
Methods
Study Design and Population
The Medical Monitoring Project (MMP) is a surveillance system that produces nationally representative estimates of behavioral and clinical characteristics of adults aged ≥18 years with diagnosed HIV living in the United States. 5 MMP uses a 2-stage sampling design, where 23 project areas are sampled from all 50 states, the District of Columbia, and Puerto Rico. During the second stage, simple random samples of eligible adults aged ≥18 years with diagnosed HIV living in those areas are sampled from the National HIV Surveillance System (NHSS), a census of people in the United States with diagnosed HIV. 2 Information about MMP sampling, data collection, and weighting processes has been described previously. 5 MMP is conducted as part of routine public health surveillance; it is deemed to be nonresearch. 6 Participating project areas obtained institutional review board approval for data collection as needed; currently, only 2 MMP project areas submit the project to their local institutional review boards. Informed consent was obtained from all MMP participants.
For its 2018 cycle, MMP collected interview and medical record data from June 2018 through May 2019. All sampled project areas participated. In total, 9700 people were sampled from NHSS, 9092 were eligible, 4050 responded, and the response rate among eligible people was 45%. MMP collects information from 36 of the 48 EHE priority counties, San Juan (Puerto Rico), and 1 of the 7 EHE priority states (Mississippi). Residence in an MMP EHE priority area was determined from the reported county of residence in the Federal Information Processing System (FIPS) code in NHSS at the time of sampling (December 31, 2017). Participants who were sampled in 1 project area but were later discovered, through either the interview or updates to NHSS, to have lived in a different project area at the time of sampling were excluded from the analysis (n = 116). For respondents with missing county FIPS code (n = 199), we were able to determine the county FIPS code from the city or county name for the majority (n = 188). After all exclusions, we analyzed data from 3923 participants.
Statistical Analysis
We conducted all analyses using SAS-callable SUDAAN version 11.03 (RTI International) to account for the complex survey design and weights. We estimated the weighted prevalence and 95% CI of sociodemographic characteristics, quality of care and clinical outcomes, health and sexual behaviors, mental health status, and barriers to HIV care of adults with HIV living in MMP EHE priority areas and not living in MMP EHE priority areas. We assessed sociodemographic characteristics associated with residing in MMP EHE priority areas and compared quality of care and clinical outcomes, health and sexual behaviors, mental health status, and barriers to HIV care of people residing in MMP EHE priority areas with people who did not live in MMP EHE priority areas using prevalence ratios (PRs) with predicted marginal means along with associated 95% CIs. 7
Measures
Data on sociodemographic characteristics, health and sexual behaviors, mental health status, and barriers to HIV care were self-reported and measured during the 12 months before the interview, except where otherwise noted. Quality of care and clinical outcomes included antiretroviral therapy (ART) prescription, ART adherence, measures for engagement in care, and viral suppression. Data on ART prescription, engagement in care, and viral suppression measures were abstracted from medical records. Data on ART prescription were calculated among people who had a medical record abstraction, indicating receipt of HIV care. ART adherence was self-reported among people taking ART, and adherence scores were calculated using a validated scale; scores ranged from 0 to 100 and were dichotomized as ≥85 for analysis. 8 Retention in HIV care in the past 12 and 24 months was measured by 2 elements of outpatient HIV care at least 90 days apart in each 12-month period; outpatient HIV care was defined as any documentation in the medical record of the following: encounter with an HIV care provider, viral load test result, CD4 test result, HIV resistance test or tropism assay, ART prescription, Pneumocystis carinii pneumonia prophylaxis, or Mycobacterium avium complex prophylaxis.
Mental health status included symptoms of depression or anxiety in the past 2 weeks before the interview. Responses to the 8 items on the Patient Health Questionnaire (PHQ-8) 9 were used to define “major depression” and “other depression,” according to criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). 10 Major depression was defined as having ≥5 symptoms of depression; other depression was defined as having 2-4 symptoms of depression. Responses to the Generalized Anxiety Disorder Scale (GAD-7) 11 were used to define anxiety according to criteria from DSM-IV; anxiety was defined as having a score ≥10.
Missed any scheduled HIV care appointments in the past 12 months was self-reported. Viral suppression was defined as most recent viral load measurement documented undetectable or <200 copies/mL, and durable viral suppression was defined as all viral load measurements documented undetectable or <200 copies/mL in the past 12 months. Viral suppression measures were calculated among people with a viral load test result documented in their medical record, indicating receipt of HIV care. Health behaviors included current cigarette smoking, binge and heavy drinking in the past 30 days, and any noninjection or injection drug use. Noninjection drugs assessed marijuana, methamphetamine, cocaine, crack, club drugs, amyl nitrite, or prescription drugs used for nonmedical purposes. Injection drugs included injection of cocaine, heroin, methamphetamine, or prescription opioids injected for nonmedical purposes. Barriers to HIV care were measured using 5 questions about things that impeded receipt of care, which included problems with money and health insurance, depression or mental health problems, delayed care because felt well, problems getting to appointments, and too busy with other personal things, such as family or work.
Results
During 2018, 52.7% of adults with diagnosed HIV lived in MMP EHE priority areas (Table 1). Living in an MMP EHE priority area was more common among adults aged 25-44 years than among adults aged ≥65 years (58.6% [95% CI, 48.5%-68.0%] vs 51.2% [95% CI, 42.5%-59.8%]) and among non-Hispanic Black and Hispanic people than among non-Hispanic White people (59.3% [95% CI, 44.7%-72.4%] and 58.4% [95% CI, 49.4%-66.8%] vs 41.0% [95% CI, 30.4%-52.6%]). People who were homeless or who reported food insecurity in the past 12 months were more likely to live in an MMP EHE priority area than those who were not homeless (60.9% [95% CI, 48.7%-71.8%] vs 51.9% [95% CI, 43.7%-60.1%]) or who did not report food insecurity (59.8% [95% CI, 50.9%-68.1%] vs 51.0% [95% CI, 42.3%-59.6%]).
Prevalence of residing in Medical Monitoring Project (MMP) Ending the HIV Epidemic (EHE) priority areas among adults aged ≥18 years with diagnosed HIV, by sociodemographic characteristics of participants, United States, 2018 a
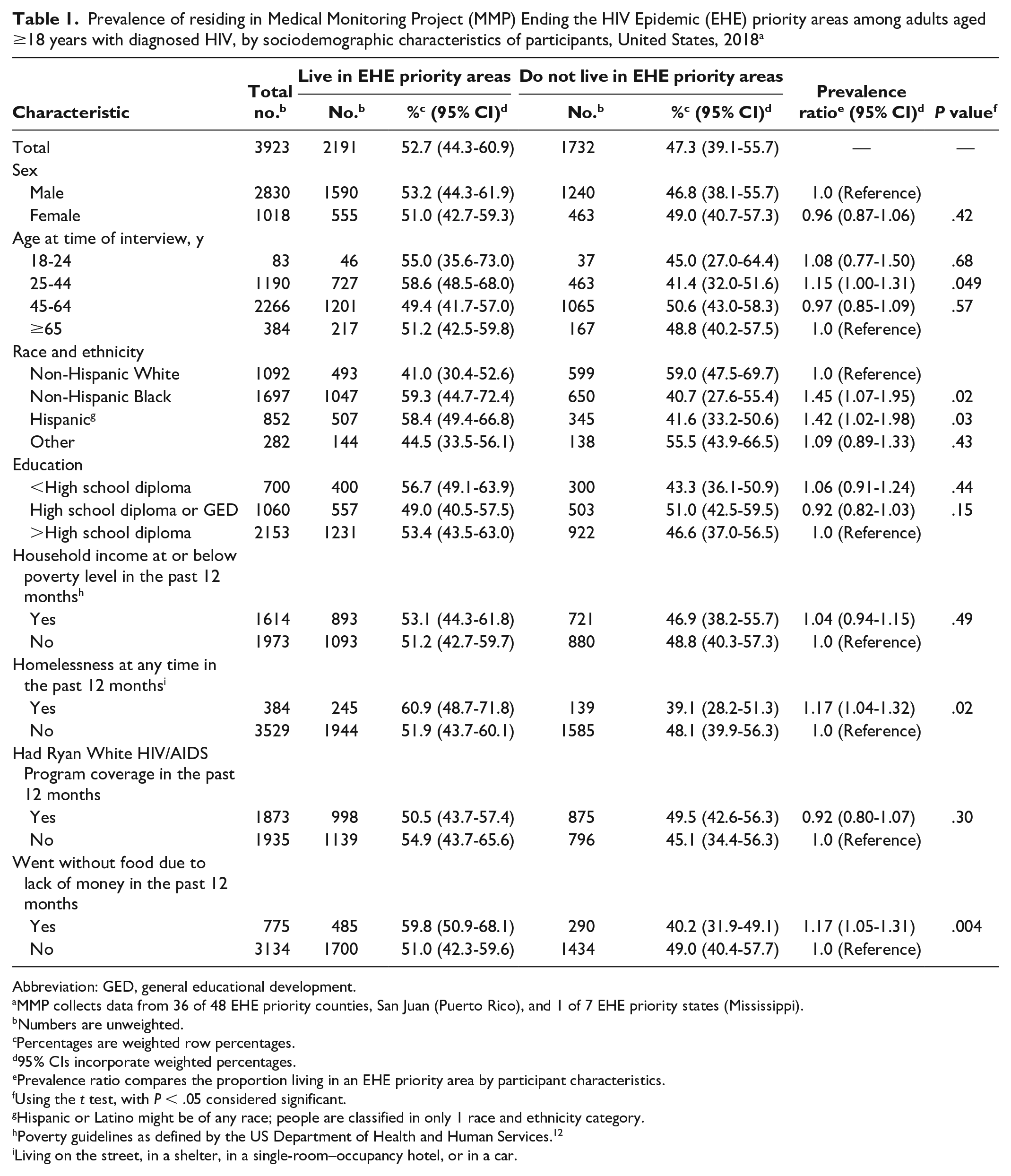
Abbreviation: GED, general educational development.
MMP collects data from 36 of 48 EHE priority counties, San Juan (Puerto Rico), and 1 of 7 EHE priority states (Mississippi).
Numbers are unweighted.
Percentages are weighted row percentages.
95% CIs incorporate weighted percentages.
Prevalence ratio compares the proportion living in an EHE priority area by participant characteristics.
P < .05 was considered significant.
Hispanic or Latino might be of any race; people are classified in only 1 race and ethnicity category.
Poverty guidelines as defined by the US Department of Health and Human Services. 12
Living on the street, in a shelter, in a single-room–occupancy hotel, or in a car.
We found no association between living in an MMP EHE priority area and ART prescription among people who received HIV care (Table 2). Among people in care, people living in MMP EHE priority areas were significantly less likely to have recent viral suppression (PR = 0.96; 95% CI, 0.94-0.98) and be durably virally suppressed (PR = 0.94; 95% CI, 0.91-0.97). People living in MMP EHE priority areas were 5% less likely to be adherent to their HIV medications (PR = 0.95; 95% CI, 0.91-0.99), 31% more likely to miss any scheduled appointment for HIV care (PR = 1.31; 95% CI, 1.10-1.56), and 10% more likely to have engaged in vaginal or anal sex during the past 12 months (PR = 1.10; 95% CI, 1.02-1.18) than people not living in MMP EHE priority areas. Depression was marginally (PR = 0.85; 95% CI, 0.73-1.00) associated with living in an MMP EHE priority area. People living in an MMP EHE priority area were 26% (PR = 0.76; 95% CI, 0.62-0.88) less likely to report anxiety than people not living in MMP EHE priority areas. Regarding barriers to HIV care, people living in MMP EHE priority areas were 30% more likely (PR = 1.30; 95% CI, 1.07-1.58) to report being too busy with other personal things such as family or work as a barrier to care compared with people not living in MMP EHE priority areas.
Associations between quality of care and clinical outcomes, health and sexual behaviors, mental health status, and barriers to HIV care and residing in Medical Monitoring Project Ending the HIV Epidemic (EHE) priority areas among people with diagnosed HIV, United States, 2018 (N = 3923) a
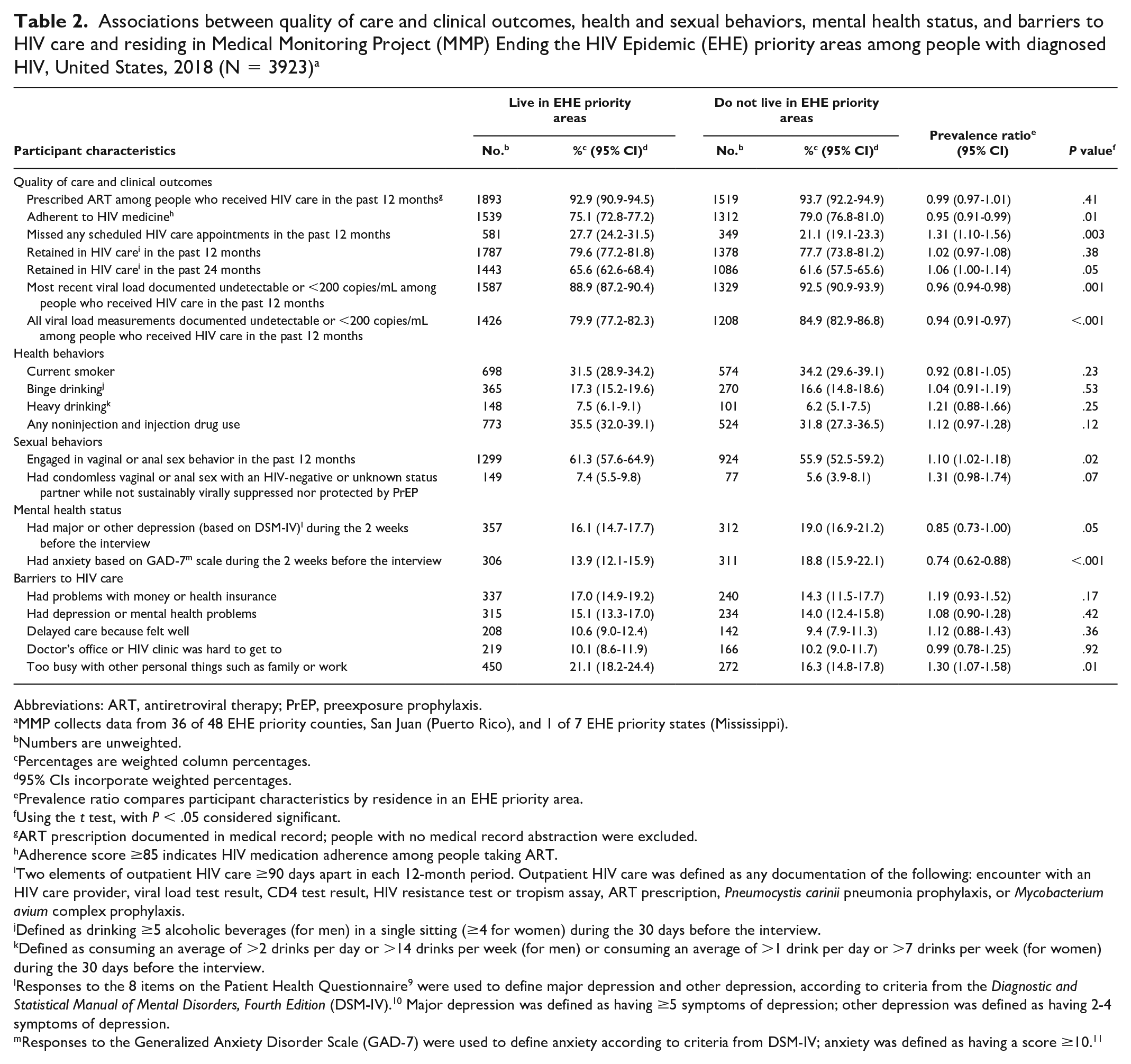
Abbreviations: ART, antiretroviral therapy; PrEP, preexposure prophylaxis.
MMP collects data from 36 of 48 EHE priority counties, San Juan (Puerto Rico), and 1 of 7 EHE priority states (Mississippi).
Numbers are unweighted.
Percentages are weighted column percentages.
95% CIs incorporate weighted percentages.
Prevalence ratio compares participant characteristics by residence in an EHE priority area.
P < .05 was considered significant.
ART prescription documented in medical record; people with no medical record abstraction were excluded.
Adherence score ≥85 indicates HIV medication adherence among people taking ART.
Two elements of outpatient HIV care ≥90 days apart in each 12-month period. Outpatient HIV care was defined as any documentation of the following: encounter with an HIV care provider, viral load test result, CD4 test result, HIV resistance test or tropism assay, ART prescription, Pneumocystis carinii pneumonia prophylaxis, or Mycobacterium avium complex prophylaxis.
Defined as drinking ≥5 alcoholic beverages (for men) in a single sitting (≥4 for women) during the 30 days before the interview.
Defined as consuming an average of >2 drinks per day or >14 drinks per week (for men) or consuming an average of >1 drink per day or >7 drinks per week (for women) during the 30 days before the interview.
Responses to the 8 items on the Patient Health Questionnaire (PHQ-8) 9 were used to define major depression and other depression, according to criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. 10 Major depression was defined as having ≥5 symptoms of depression; other depression was defined as having 2-4 symptoms of depression.
Responses to the Generalized Anxiety Disorder Scale (GAD-7) were used to define anxiety according to criteria from DSM-IV; anxiety was defined as having a score ≥10. 11
Discussion
We found differences among sociodemographic groups in prevalence of MMP EHE priority area residence and lower prevalence of ART and visit adherence in MMP EHE priority areas. Moreover, among adults with diagnosed HIV who received medical care in the past 12 months, people who were living in MMP EHE priority areas were significantly less likely to be virally suppressed than people not living in MMP EHE priority areas.
Adherence to ART is necessary to maintain viral suppression and reduce HIV transmission 13 ; missed HIV medical visits can lead to poor clinical outcomes. 14 Because ART and visit adherence have been shown to be essential for optimal health and viral suppression, and we found both to be significantly lower in MMP EHE priority areas, interventions that focus on improving these indicators could help improve viral suppression among people receiving HIV care. To improve ART and visit adherence, evidence-based guidelines emphasize monitoring self-reported ART adherence and HIV care retention (eg, visit adherence, gaps in care, and visits per interval of time) and use of adherence reminders (eg, pill organizers, dose planners, and reminder alarm devices), combined with education and counseling. 15
People with HIV experiencing homelessness have substantial barriers to HIV medical care access, poor ART adherence, decreased viral suppression, and engagement in behaviors that increase the risk of HIV transmission.16,17 People with HIV living in MMP EHE priority areas were 17% more likely than people not living in MMP EHE priority areas to experience homelessness and to report food insecurity, indicating the need to enhance access to ancillary medical and support services. 18 Use of on-site support services may improve viral suppression—and, thus, reduce HIV transmission—by addressing immediate needs, offering comprehensive health services, systemically monitoring retention in care, and supporting ART adherence.19,20 Furthermore, because we found that people in MMP EHE priority areas were more likely than people not living in MMP EHE priority areas to report being too busy with personal things as a barrier to receiving HIV care, these jurisdictions could consider expanding alternatives to traditional care such as telehealth programs, which have been found to be effective in increasing access to quality HIV care. 21
We also found that the prevalence of depression and anxiety symptoms was lower among adults who lived in MMP EHE priority areas compared with adults who did not live in MMP EHE priority areas. To explore further, we adjusted the regression models for depression and anxiety by sex, age, and race and ethnicity, but the results were substantively the same. A possible explanation beyond these demographic factors might be that most of the counties prioritized for EHE are large urban areas. HIV stigma has been found to be more prevalent in smaller urban and rural areas compared with large urban areas, 22 and stigma is associated with a higher prevalence of depression and anxiety among people with HIV.23,24 Our findings may support the need to enhance access to mental health screening and treatment for people with HIV who do not live in EHE priority areas. Further work may be needed to more fully elucidate the relationship between residence in an EHE priority area and mental health.
Limitations
Our analysis had several limitations. First, self-reported information may be subject to recall biases that may lead to measurement error. Second, our study used most recent address in NHSS to determine residence in an EHE priority area. Thus, participants sampled in 1 MMP project area but who had moved to a different MMP project area by the time of the interview were excluded from the analysis, although this movement only applied to 3% of all respondents. Third, MMP did not sample areas by EHE and non–EHE priority designation, and the data were not weighted according to the population distribution among those areas; therefore, the results are not representative of all EHE and non-EHE jurisdictions. However, MMP is designed to represent all adults with diagnosed HIV in the United States, and the demographic characteristics among people living in MMP EHE priority areas align with characteristics among populations with higher HIV incidence, on which EHE priority area designation was based. 2 Although we were able to include only those EHE priority areas that participated in MMP (ie, 36 of 48 EHE priority counties, San Juan, and 1 of 7 EHE priority states), all participating MMP project areas included approximately 72.8% of all people in the United States with diagnosed HIV in 2016. 5
Conclusion
Rates of appointment adherence for HIV care, ART adherence, and viral suppression among people with HIV living in MMP EHE priority areas were low compared with those of people not living in MMP EHE priority areas. To improve health outcomes and reduce transmission of HIV, our findings suggest that strengthening efforts to improve medication and appointment adherence among adults with HIV living in EHE priority areas could improve their health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: The Medical Monitoring Project is funded by the Centers for Disease Control and Prevention.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.