
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has challenged the ability of harm reduction programs to provide vital services to adolescents, young adults, and people who use drugs, thereby increasing the risk of overdose, infection, withdrawal, and other complications of drug use. To evaluate the effect of the COVID-19 pandemic on harm reduction services for adolescents and young adults in Boston, we conducted a quantitative assessment of the Community Care in Reach (CCIR) youth pilot program to determine gaps in services created by its closure during the peak of the pandemic (March 19–June 21, 2020). We also conducted semistructured interviews with staff members at 6 harm reduction programs in Boston from April 27 through May 4, 2020, to identify gaps in harm reduction services, changes in substance use practices and patterns of engagement with people who use drugs, and how harm reduction programs adapted to pandemic conditions. During the pandemic, harm reduction programs struggled to maintain staffing, supplies, infection control measures, and regular connection with their participants. During the 3-month suspension of CCIR mobile van services, CCIR missed an estimated 363 contacts, 169 units of naloxone distributed, and 402 syringes distributed. Based on our findings, we propose the following recommendations for sustaining harm reduction services during times of crisis: pursuing high-level policy changes to eliminate political barriers to care and fund harm reduction efforts; enabling and empowering harm reduction programs to innovatively and safely distribute vital resources and build community during a crisis; and providing comprehensive support to people to minimize drug-related harms.
Keywords
As stores closed their doors and businesses reduced hours to curb the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus disease 2019 (COVID-19), many life-saving harm reduction programs also shut their doors, increasing vulnerability to drug-related harms for people who use drugs (PWUD). Although drug use and associated harms, including overdose, HIV, and other bloodborne infections, continued and likely increased, 1 the void created by the loss of harm reduction services designed to mitigate these harms may have led to greater mortality and morbidity for this population.
Adolescents and young adults are a particularly vulnerable population among PWUD. 2 In 2017, 5455 adolescents and young adults aged 15-24 died of drug overdose in the United States—a 340% increase from 1999 compared with a 317% increase in the total population. 3 Compared with older adults, adolescents and young adults are just as affected by the myriad harms associated with drug use, 4,5 yet they do not engage with traditional harm reduction services. 6,7 In response to increasing overdose rates and a cluster of HIV cases that emerged in December 2019, harm reduction efforts in Boston were expanded. 8 Among the services deployed was a mobile health program, Community Care in Reach (CCIR). 9 Additional funding that was originally focused on adults prompted the formation of a pilot program to expand and tailor harm reduction services to adolescents and young adults who use drugs. From December 23, 2019, through March 18, 2020, the pilot program brought clinical staff members and outreach workers who were experienced in working with adolescents and young adults to drug use hotspots in Boston two days per week to build relationships with adolescents and young adults who use drugs; distribute naloxone and syringes; and offer medications for opioid use disorder (OUD), testing for sexually transmitted infections, health care, and other social services.
We conducted an evaluation of the CCIR youth pilot program to assess the number of contacts made and the number of syringes and units of naloxone distributed, as well as to investigate gaps in care. Although the CCIR pilot program continued serving adolescents and young adults of Boston well into the COVID-19 pandemic, CCIR suspended services in March 2020, before the peak of the pandemic in April 2020, because of concerns about infection control, the ability to maintain social distance, and loss of staff members as workers aided in the COVID-19 emergency response. The gap in services left by the closure of CCIR during a critical time prompted us to consider the effect of COVID-19 on harm reduction services for adolescents and young adults in Boston, including what other gaps in harm reduction services existed, how substance use practices and patterns of engagement with PWUD changed, and how other harm reduction programs adapted to pandemic conditions.
Methods
We used quantitative methods to assess the number of contacts made and the number of syringes and units of naloxone distributed by the CCIR youth pilot program from December 23, 2019, through March 18, 2020, when the program was suspended for 3 months. The program resumed services on June 15, 2020. The mobile van was deployed twice weekly, on Mondays and Wednesdays, excluding holidays. For each visit, we recorded the number of contacts engaged with and the number of units of naloxone and number of syringes distributed. We estimated the number of contacts missed per month during the 3-month closure by calculating the average number of contacts from the complete months of service (January 1–February 29, 2020, and July 1–October 19, 2020). We repeated this method to estimate the number of units of naloxone and number of syringes that were not distributed.
We used qualitative methods to investigate how harm reduction programs are adapting to provide services to adolescents and young adults during the COVID-19 pandemic, describe changes in substance use practices and patterns of engagement with PWUD, and identify gaps in harm reduction services. We identified a convenience sample of 12 harm reduction programs commonly visited by adolescents and young adults in Boston, generated from an internet search and expert knowledge. We contacted each program by telephone and asked to speak with a program worker who was familiar with the harm reduction operations. We made contact with and interviewed harm reduction program workers at 6 of the 12 programs: 3 harm reduction programs associated with community health centers, 1 harm reduction–focused homeless shelter for young people, and 2 standalone harm reduction programs. After obtaining verbal consent, we conducted semistructured interviews by telephone from April 27 through May 4, 2020, during the height of the COVID-19 pandemic. We inquired about (1) the harm reduction services provided to adolescents and young adults; (2) changes in hours, staffing, and supplies; (3) challenges that affected their capacity to provide services; (4) changes in what clients were asking for; (5) changes in patterns of substance use that program workers had observed; and (6) other reflections on the effect of the COVID-19 pandemic on harm reduction for adolescents and young adults. We used conventional content analysis to distill the findings from our conversations into emergent themes. We then used the Ecological Model of Public Health to translate these findings into lessons learned and recommendations. 10 This model emphasizes the levels of influence in public health practice and interventions and recognizes that drug-related harms are not solely the result of individual behaviors but are also affected by the upstream organizations serving them and the policy environment in which they reside.
Because this study was a verbal research survey with a low risk of harm to participants, the Harvard Longwood Campus Institutional Review Board determined this study to be exempt from review.
Outcomes
From December 23, 2019, through March 18, 2020, the CCIR mobile van made 284 contacts and distributed 520 syringes and 421 units of naloxone (Figure). During the 3-month suspension of mobile van services, CCIR missed an estimated 363 contacts, 169 units of naloxone distributed, and 402 syringes distributed. From June 15 through October 19, 2020, the mobile van made 593 contacts and distributed 248 units of naloxone and 590 syringes during 32 visits.
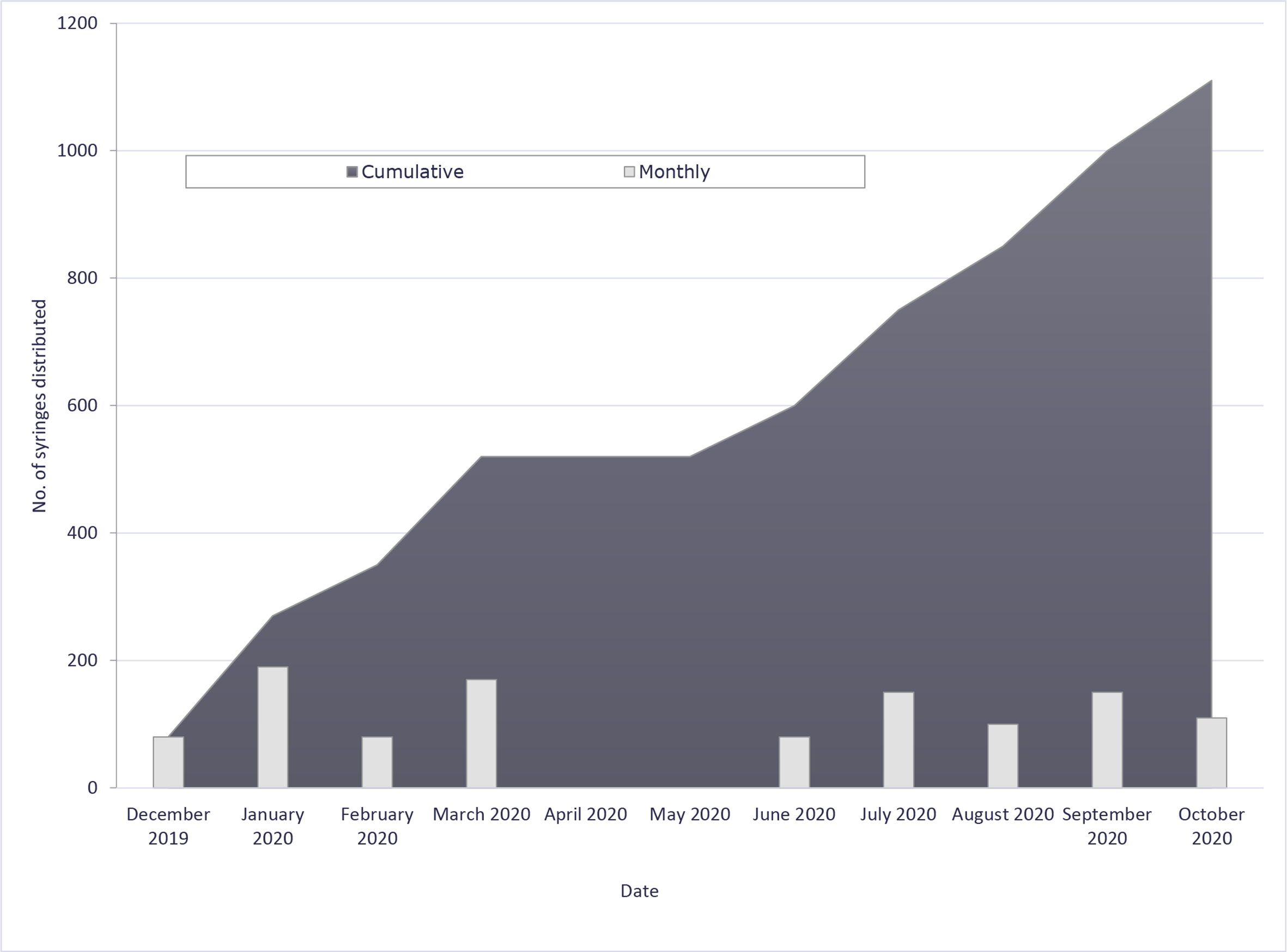
Number of syringes distributed to adolescents and young adults through the Community Care in Reach harm reduction program, Boston, December 2019–October 2020. Services were suspended during the coronavirus disease 2019 pandemic, from March 19 to June 21, 2020; as such, no syringes were distributed during this time.
Several common themes emerged from our qualitative interviews, including capacity to continue operations, shifting focus to outreach, greater risk of harm, and need for community. These observations are not specific to adolescents and young adults, because all but 1 of the 6 harm reduction programs serve all populations and do not have programming specific to young people.
Reduced Capacity
All of the harm reduction service providers we interviewed were operating during the pandemic but at reduced capacity and restricted hours. Many interviewees reported that program staffing was reduced as workers became sick, student workforces dissolved, and medical and public health professionals balanced multiple new obligations. New workflow practices created more work for programs, including increased cleaning and packaging of supplies into single-serve packets. Most programs encountered difficulty securing sufficient supplies such as naloxone, safer drug use equipment (eg, clean needles, cookers, and cottons), personal protective equipment (PPE), and hygiene products (eg, hand sanitizer).
Increased Focus on Outreach
Most programs shifted from drop-in service to scaled-up outreach. One program tried a “one in, one out” policy, but shortly thereafter it closed the drop-in center completely because of concerns about hygiene and a decreasing number of visitors. Another program moved drop-in services outside, offering naloxone and pre-made outreach kits. Before COVID-19, one program estimated caring for up to 150 visitors daily at its drop-in center. During COVID-19, the outdoor drop-in site served about two-thirds of the normal number of visitors. Other programs reported similar reductions in contacts.
Greater Risk of Complications
With reductions in access to naloxone, syringes, safer drug use equipment, and usual drug supply, PWUD faced a greater risk of overdose, infection, and withdrawal. As libraries, public transportation, public bathrooms, shops, and other public spaces closed, more overdoses occurred in isolated and private areas than in public spaces. People used naloxone to rescue peers from overdose without reporting naloxone use or calling 911, suggesting that overdose statistics were underestimated.
New Encampments
People who lacked stable housing were less likely to stay in shelters during the pandemic than before the pandemic because of reduced shelter capacity and/or personal desire to avoid crowding, infection risk, and COVID-19 testing. More encampments cropped up in areas outside of Boston. Although encampments were present before the pandemic, the number of encampments increased and they frequently moved in response to police presence. These changes challenged programs to adapt services to cover new geographic areas with potentially different needs.
Asking for Help
An inconsistent drug supply, caused by border closures, reduced income, and social distancing measures, may have precipitated withdrawal. Barriers to entering detoxification and sober houses increased, and PWUD were reluctant to enter residential programs because of concerns about infection control and hesitant to enter a new environment during uncertain times. Accordingly, many programs noticed an increase in interest in OUD medications. Sublocade, an injectable form of buprenorphine administered once per month, became an increasingly popular treatment option. Take-home methadone and longer suboxone prescriptions helped people maintain stable recovery. Programs also made more referrals to behavioral health during the pandemic than before the pandemic. One program worker said, “People seem more inclined to ask for help; it’s less stigmatized right now.”
Different Priorities
PWUD had different priorities when it came to guidelines for social distancing and pandemic preparations. For example, they may not have had a safe place to isolate, they may have been food insecure, or they may have been worried about how to stay out of withdrawal. A street outreach worker said, “It [was] difficult to stress the importance of precautions for the COVID-19 pandemic when their priority chain is so different.”
Community
People who worked in harm reduction programs said they were not able to provide the community and support that are central to their practice. Multiple interviewees emphasized that harm reduction programs are a haven for unconditional acceptance and support for people who are already marginalized, stigmatized, and ostracized in their daily lives. They serve as trusted centers for communication and dissemination of information to this population, who may not have received mainstream public health messaging about COVID-19. Interviewees emphasized that building trust is imperative to delivering services to adolescents and young adults. It is challenging to build trust with adolescents and young adults who use drugs under non-pandemic conditions; closed doors, social distancing, and PPE diminished these opportunities even further.
Lessons Learned
Results from the CCIR adolescents and young adults pilot highlight the gap left by the suspension in services and underscore the importance of continuing harm reduction service outreach for PWUD, particularly during the COVID-19 pandemic, when traditional models of care may be less preferable or even inaccessible than targeted outreach services. Distribution of supplies, including naloxone and clean syringes, is even more crucial for reducing drug-related harms as the risk of overdose, infection, withdrawal, and other complications of drug use increases and consistent access to harm reduction services decreases. Engagement with the mobile van may help alleviate the ostracization that adolescent and young adult PWUD feel, which is worsened by pandemic precautions, and instead promote the trust that is vital to their interaction with services.
We integrated insights gathered from our qualitative interviews with harm reduction program workers with the expertise of harm reduction specialists (S.K., A.O., J.M.G., E.M.T., A.C.) to present our lessons learned and recommendations, nested within the framework of the Ecological Model of Public Health. 10 We recommend far-reaching structural changes at the policy level, program level, and individual level (Box). We also discuss recommendations specific to adolescents and young adults.
Recommendations for sustaining harm reduction services for adolescents and young adults during a crisis
Engage with experts in the community. Learn from PWUD to inform policy decisions.
Reduce barriers to treatment.
Designate syringe access, buprenorphine, methadone, naltrexone, naloxone, and other services provided by harm reduction organizations as “essential services.”
Support longer take-home periods for OUD medications. 11
Cover all OUD medications without prior authorization.
Suspend counseling and in-person visit requirements to receive OUD medications.
Expand coverage for telehealth services, including virtual counseling, peer support, and OUD treatment initiation.
Ensure that telehealth includes telephone calls for people who cannot access smartphones or laptops.
Reimburse for visits with licensed clinical addiction specialists and peer counselors.
Whenever possible, programs should continue services to protect PWUD, with modifications to maintain social distancing and infection control.
Plan for supply shortages: stock up on naloxone, syringes, safer drug use equipment, PPE, and hand sanitizer for distribution to participants.
Plan for staff shortages: cross-train staff members and create contingency plans to prioritize essential services.
Outreach: scale up street outreach and mobile delivery to ensure access to naloxone, syringes, safer drug use equipment (eg, clean needles, cookers, and cottons), and infection control materials, in addition to information on safer drug use strategies and infection precautions.
Connect PWUD to health care, case management, and housing services as needed.
Reorient to social media.
Use technology to build community virtually, check on participants, and guide outreach efforts, while respecting that many in this group will not have access to telephones and/or the internet.
Offer alternatives to people using drugs in isolation: hotline, FaceTime, or safety applications, such as Canary, 12 Remote Egg Timer, 13 and Kitestring. 14
Programs with OUD treatment capacity should lower barriers to treatment, engage in advance planning for treatment continuity, and use telehealth where appropriate.
Protect against infection.
Minimize close contacts, minimize sharing of supplies, and prepare your own drugs.
Stock up on supplies (syringes/safer injecting equipment, drugs, soap, hand sanitizer).
If possible, have enough syringes and injecting equipment to last 2-4 weeks.
If sick, see if programs will deliver equipment or medications.
If out of unused syringes, disinfect used syringes with 1:10 diluted bleach.
Protect against overdose.
Prepare for overdose by carrying multiple doses of naloxone (less likely to be dispensed to adolescents and young adults). 17
When using with others, maintain social distance, stagger times of use, and create an overdose plan. 18
If alone, use less, call a hotline, 19 call or FaceTime someone, and/or use safety applications.
Disruption to usual supply chain could lead to more heroin with fentanyl—use fentanyl test strips to test your drugs before using. 20
Prepare for a drug shortage by stocking up, considering alternatives (eg, buprenorphine/methadone), and/or preparing for withdrawal with over-the-counter medications (eg, Pepto-Bismol, ibuprofen, and Imodium), taking care to stay within dosage guidelines.
Reduce policy barriers to care for adolescents and young adults.
Suspend antiquated laws that increase treatment barriers, such as a Massachusetts law that requires that 2 physicians agree that a person aged 12-18 years meets the criteria for OUD before prescribing treatment without parental consent. 21
Eliminate delays for parental/guardian consent for services. 22
Increase flexible funding for programs specific to adolescents and young adults. 22
Tailor services to the needs of people who identify as lesbian, gay, bisexual, transgender, queer/questioning, intersex, and/or asexual and racial/ethnic minority adolescents and young adults, who are disproportionately affected by homelessness and high rates of infection. 22,23
Use telehealth, mobile check-ins, social media community groups, and other methods to connect with adolescents and young adults, who will benefit from engagement with technology. 24
Abbreviations: OUD, opioid use disorder; PPE, personal protective equipment; PWUD, people who use drugs.
Policy Level
Policies need to facilitate safer drug use and reduce barriers to services and treatment for PWUD who use drugs. Policy makers should engage with experts in the community and learn from PWUD to inform policy decisions. Policies should designate syringe access, OUD medications, naloxone, and other services provided by harm reduction organizations as “essential services” to allow continuous operation during a state of emergency. States should request exceptions to give patients longer take-home periods for OUD medications, cover all OUD medications without prior authorization, and suspend counseling and in-person visit requirements. 11 Programs stressed the need for expansion and coverage of telehealth services, including virtual counseling and OUD treatment initiation, visits with licensed clinical addiction specialists, and peer support. Telehealth should include telephone calls for people who cannot access smartphones, laptops, or the internet.
Program Level
Whenever possible, programs should continue services to protect PWUD, with modifications to maintain social distancing and infection control. Programs should plan for supply shortages and stock up on naloxone, syringes, safer drug use equipment, PPE, and hand sanitizer for distribution to participants. They can also plan for staff shortages by cross-training staff members and creating contingency plans to prioritize essential services. Our interviewees stressed the importance of scaling up street outreach and mobile delivery to ensure access to naloxone, syringes, safer drug use equipment, and infection control materials, in addition to information on safer drug use strategies and COVID-19 precautions. Technology can be used to build community virtually, check in on regular participants, and guide outreach efforts, while respecting that many people in this group will not have access to a telephone. With more drug use occurring in isolated and private areas, PWUD face an increased risk of death from overdose. 25 Thus, it is important to offer resources to PWUD who use drugs: hotline, Facetime, and safety apps, such as Canary, 12 Remote Egg Timer, 13 and Kitestring. 14 These safety apps work by alerting an emergency contact or 911 if a person does not move or press a button within a certain period.
Individual Level
PWUD can protect against infection by minimizing close contacts, limiting the sharing of supplies, and preparing their own drugs. 15,16 PWUD can stock up on supplies (syringes/safer injecting equipment, drugs, soap, sanitizer), ideally having enough to last 2-4 weeks. If PWUD run out of unused syringes, they can disinfect used syringes with a 1:10 diluted bleach. PWUD should protect against overdose by carrying multiple doses of naloxone, which is less likely to be dispensed to adolescents and young adults than to PWUD. 17 When using drugs with others, PWUD should maintain social distance, stagger times of use, and create an overdose plan. 18 If alone, PWUD should use less, call a hotline, 19 call or FaceTime someone, and/or use a safety app. PWUD should be aware that disruption to usual supply chains could lead to more heroin laced with fentanyl, so it is good practice to use fentanyl test strips to test drugs before using. 20 Lastly, PWUD can prepare for a drug shortage by stocking up, considering alternatives such as buprenorphine/methadone, and/or preparing for withdrawal with over-the-counter medications, such as Pepto-Bismol, ibuprofen, and Imodium (taking care to stay within dosage guidelines).
Recommendations Specific to Adolescents and Young Adults
One policy recommendation specific to adolescents and young adults is to eliminate service delays due to parental/guardian consent. 22 States should also suspend antiquated laws that increase barriers to treatment, such as a Massachusetts law that requires that 2 physicians agree that a person aged 12-18 years meets criteria for OUD before prescribing treatment without parental consent. 21 Increasing flexible funding for programs specific to adolescents and young adults will enable the provision of life-saving services for young people. 22 At the program level, programs should tailor services to the needs of people who identify as lesbian, gay, bisexual, transgender, queer or questioning, intersex, and/or asexual and racial/ethnic minority adolescents and young adults, who are disproportionately affected by homelessness and high rates of COVID-19 infection. 22,23 One author (A.O.) emphasized that high rates of institutional involvement (Department of Children and Families, Department of Youth Services) promote mistrust of authority and institutions among adolescents and young adults; thus, building trust is imperative for the successful delivery of services. Adolescents and young adults in particular may benefit from greater engagement with technology, including telehealth visits, text check-ins, peer support via FaceTime, and hotlines. 24 At the individual level, adolescents and young adults may be less likely to wear face masks and maintain social distance than older adults; as such, spreading information about safe social distancing practices and strategies for safer drug use is important. 15,16
Although our findings illustrate changes and challenges that PWUD and harm reduction programs face and expose existing gaps in services, a major limitation of convenience sampling lies in generalizing these findings to other programs. It was difficult to obtain information specific to adolescents and young adults, because most harm reduction programs serve all populations and do not have programming that is specific to young people. These limitations speak to the need for targeted investigation to understand how we can develop services to address the needs of this unique population. An additional area for investigation is a direct assessment and evaluation of the CCIR adolescent and young adult program. In addition, directly interviewing clients of harm reduction programs and PWUD about their patterns of drug use, experiences with harm reduction programs, and unique needs during the pandemic would be invaluable to identify gaps in services and develop effective engagement strategies.
Conclusion
Amid the pandemic, harm reduction programs for PWUD are struggling to maintain staffing, supplies, infection control measures, and regular connection with their participants. Participants face a greater risk of complications and decreased access to life-saving services during the pandemic than before the pandemic. Adolescents and young adults are a unique population, and further investigation is needed to understand how to tailor harm reduction services to their needs and patterns of engagement. As additional waves of the COVID-19 pandemic occur, we must prepare and build for the future by pursuing high-level policy changes to eliminate political barriers to care and fund harm reduction efforts; enabling and empowering harm reduction programs to innovatively and safely distribute vital resources and build community during a crisis; and providing comprehensive support to people to minimize drug-related harms.
Footnotes
Acknowledgments
The authors are grateful to the Grayken Center for Addiction Medicine, the Kraft Center for Community Health, and the Hearst Foundation for their support of the Community Care in Reach mobile van’s work in providing harm reduction and mobile health services to adolescents and young adults in Boston.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.