
Abstract
Objective:
Bacteremia is the presence of bacteria in the bloodstream. The objective of this study was to determine the relationship between low socioeconomic status (SES) and the epidemiology, process of care, and outcomes of patients with Staphylococcus aureus bacteremia (SAB).
Methods:
We conducted a multicenter, retrospective, cohort study that evaluated adult patients with SAB in 3 Los Angeles County hospitals from July 15, 2012, through May 31, 2018. We determined SES (low SES, intermediate SES, and high SES) for each patient and compared sociodemographic and epidemiologic characteristics, management of care received by patients with SAB (ie, process of care), and outcomes. We used a Cox proportional hazards model to determine predictors of 30-day mortality for each SES group.
Results:
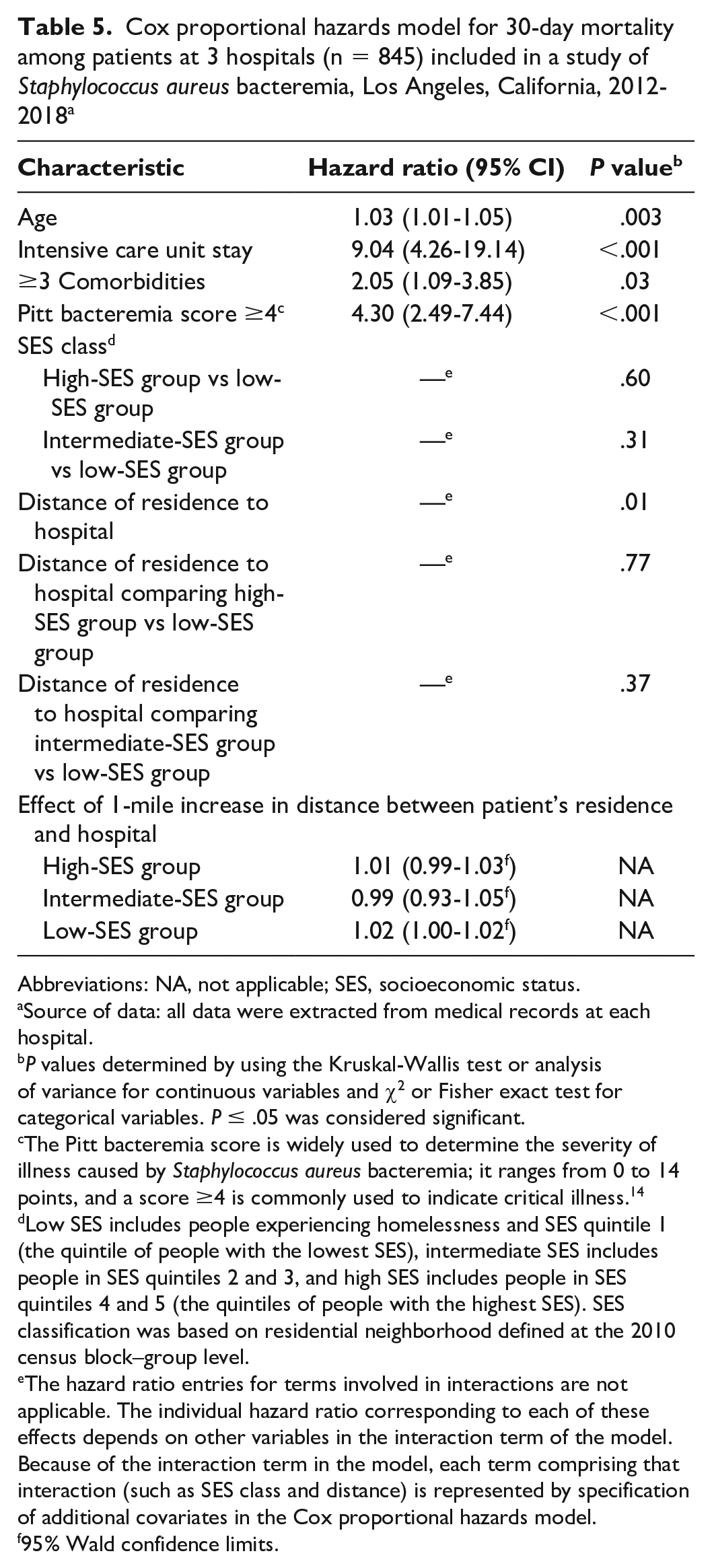
Of 915 patients included in the sample, 369 (40%) were in the low-SES group, 294 (32%) in the intermediate-SES group, and 252 (28%) in the high-SES group. Most significant predictors of 30-day mortality in the Cox proportional hazards model were admission to an intensive care unit (hazard ratio [HR] = 9.04; 95% CI, 4.26-19.14), Pitt bacteremia score ≥4 indicating critical illness (HR = 4.30; 95% CI, 2.49-7.44), having ≥3 comorbidities (HR = 2.05; 95% CI, 1.09-3.85), and advanced age (HR = 1.03; 95% CI, 1.01-1.05). Distance between home and admitting hospital affected mortality only in the low-SES group (HR = 1.02; 95% CI, 1.00-1.02).
Conclusions:
SES did not independently affect the outcome of SAB; however, the farther the patient’s residence from the hospital, the greater the negative effect on survival in a low-SES population. Our findings underscore the need to develop multipronged, targeted public health efforts for populations that have transportation barriers to health care.
Socioeconomic status (SES) is a complex variable that encompasses multiple measures, including a person’s income, education, and occupation. 1 SES affects health through environmental exposure, health behavior, and lifestyle, 1 and it is inversely related to health.2,3 Patients with low SES may have more severe illness than patients with intermediate or high SES when they arrive at a hospital because they lack preventive care, and they may require admission to an intensive care unit (ICU). 4 SES can affect the incidence of infectious diseases through differences in living conditions, comorbidities, and health care access. 5 Medically underserved populations face economic, cultural, or linguistic barriers to health care, with competing priorities that consume large proportions of their time to meet basic survival needs, which may result in health becoming a low priority.6,7
Bacteremia is the presence of bacteria in the bloodstream. Staphylococcus aureus is a leading cause of bacteremia in the United States; it is a major health care problem, often leading to bacterial persistence, metastatic complications, and death.8,9 Previous studies focused on the risk factors of microbial characteristics, age and comorbid conditions, and antibiotic exposure on outcomes of S aureus bacteremia (SAB).10 -12 However, the relationship between SAB and SES on the process of care received by the patient and outcomes has not been well studied in the United States. To develop strategies to eliminate health disparities caused by differences in SES, the objective of this study was to determine the epidemiology, process of care, and outcomes of SAB, focusing on a medically underserved population.
Methods
We performed this retrospective cohort study at 3 university-affiliated hospitals in Los Angeles County, California, serving the ninth most diverse population in the United States. 13 The University of Southern California and Quorum Review institutional review boards approved the study protocol. Informed consent was waived because this was a retrospective study. We screened microbiology reports from July 15, 2012, through May 31, 2018, for patients who had growth of S aureus in at least 1 blood culture. To be included, the patient had to be aged ≥18 years, be hospitalized, receive the first dose of an in vitro–active antimicrobial within 48 hours of the first positive blood culture result for S aureus, and receive antimicrobials for ≥48 hours. Exclusion criteria were having an invalid California address, residence in a skilled nursing facility, evidence of polymicrobial blood cultures, or an incomplete medical record.
We reviewed medical records and extracted relevant data. We calculated the Pitt bacteremia score on the day of the first positive blood culture result for S aureus. 14 The Pitt bacteremia score is used to determine the severity of illness; it ranges from 0 to 14 points, and a score ≥4 indicates critical illness. 14 We entered extracted data into Research Electronic Data Capture software (https://redcap.med.usc.edu).
Study Definitions
We based SES classification on residential neighborhood defined at the 2010 census block–group level. Area-based SES measurements take advantage of the assumed population homogeneity at census block–group levels when SES information for individuals is lacking.15,16 We geocoded home addresses into 2010 census block–group levels by using GeoServices. 17 We then assigned patients to the SES value of their neighborhoods. The SES block–group level for Los Angeles County used previously validated methods with updated 2010 census data, which produces a composite SES index in quintiles based on combined rankings of average educational attainment and median annual household income of a given area.16,18,19 For California residents living outside Los Angeles County, we defined SES by using a similar area-based method of statewide ranking that produces closely matched SES measures, also in quintiles. 16 We grouped patients into 3 categories: low SES (includes people experiencing homelessness and SES quintile 1, the quintile of people with the lowest SES), intermediate SES (includes people in SES quintiles 2 and 3), and high SES (includes people in SES quintiles 4 and 5, the quintiles of people with the highest SES). Patients in SES quintile 1 have an average of 9.9 years of education and an annual household income of $30 867.
We divided the source of SAB into 3 categories of risk of mortality, defined as death occurring within 30 days of initiating antimicrobials: low risk (<10%), intermediate risk (10%-20%), and high risk (>20%). 11 Low-risk sources were intravenous catheter–related, genitourinary, ear–nose–larynx, gynecologic, and manipulation-related; intermediate-risk sources were osteoarticular, soft-tissue, and unknown sources; and high-risk sources were endovascular, pneumonia, intra-abdominal, and central nervous system. We defined community-onset SAB as having the first blood culture with growth of S aureus within 48 hours of admission date and hospital-acquired SAB as having the first blood culture with growth of S aureus after 48 hours of admission date.
Data Analysis
We compared SES groups by sociodemographic and epidemiologic characteristics, process of care, and outcomes. We assessed the process of care by examining the receipt and timing of antimicrobials, infectious diseases consultation, and procedures used to control the source of SAB (ie, source-control procedures). Source-control procedures included removal of infected devices, surgeries, or incision and drainage to eliminate the source of SAB. Outcome measures were 30-day mortality and length of stay. We analyzed continuous data by using the Kruskal-Wallis test or analysis of variance for ≥3 group comparisons and the Wilcoxon rank sum or Student t test for 2 groups. We analyzed categorical data by using the Pearson χ2 test or Fisher exact test for dichotomous variables or R-by-C contingency χ2 test for ≥3 categories. We determined predictors of 30-day mortality by univariate analysis; we then evaluated variables identified as significant at P < .20 in a Cox proportional hazards model. We identified significant variables via forward stepwise selection for the model building, controlling for potential confounding factors. We included the distance of the patient’s residence from the admitting hospital in the Cox model; we also included patients experiencing homelessness who had a known address of a homeless shelter. Because distance of a patient’s residence from the hospital was significant by univariate analysis, we included it in the Cox model. To evaluate if the distance from the hospital significantly affected the outcome of 30-day mortality across the 3 categories of SES, we evaluated the interaction between the distance to the hospital and SES in the Cox model. In addition, we conducted a sensitivity analysis excluding patients experiencing homelessness and patients with hospital-acquired SAB. A P value of ≤.05 denotes significance. We performed statistical analysis using Prism version 5.0 (GraphPad Software) and SAS version 9.4 (SAS Institute, Inc).
Results
Of 1397 patients screened, 482 patients were excluded for the following reasons: 11 were aged <18 years, 130 received an antimicrobial for <48 hours, 44 did not receive an in vitro–active antimicrobial within 48 hours from the first positive blood culture, 82 had an invalid California address, 80 resided in a skilled nursing facility, 104 had polymicrobial blood cultures, and 31 had an incomplete medical record.
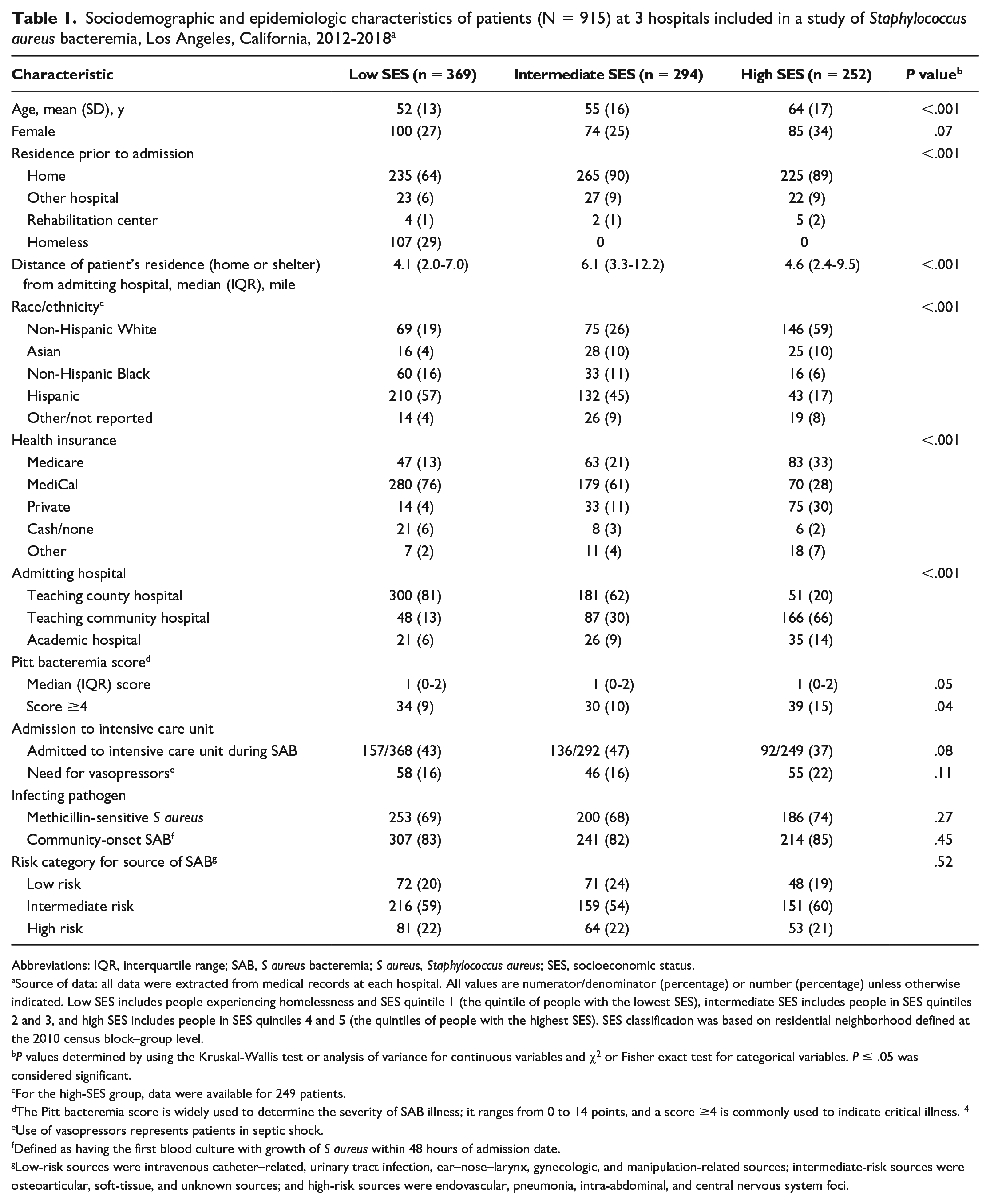
Of 915 patients included in the sample, 369 (40%) were in the low-SES group, 294 (32%) in the intermediate-SES group, and 252 (28%) in the high-SES group. The low-SES group consisted of 107 (12%) patients experiencing homelessness and 262 (29%) patients in quintile 1, the intermediate-SES group consisted of 168 (18%) patients in quintile 2 and 126 (14%) patients in quintile 3, and the high-SES group consisted of 152 (17%) patients in quintile 4 and 100 (11%) patients in quintile 5. The median distance between the patients’ residence and the admitting hospital was similar in the low-SES and high-SES groups (4.1 and 4.6 miles, respectively), but it was greatest in the intermediate-SES group (6.1 miles; P < .001; Table 1). Among the 40 patients who reported a homeless shelter as a residence, the median distance was 3.9 miles to the admitting hospital.
Sociodemographic and epidemiologic characteristics of patients (N = 915) at 3 hospitals included in a study of Staphylococcus aureus bacteremia, Los Angeles, California, 2012-2018 a
Abbreviations: IQR, interquartile range; SAB, S aureus bacteremia; S aureus, Staphylococcus aureus; SES, socioeconomic status.
Source of data: all data were extracted from medical records at each hospital. All values are numerator/denominator (percentage) or number (percentage) unless otherwise indicated. Low SES includes people experiencing homelessness and SES quintile 1 (the quintile of people with the lowest SES), intermediate SES includes people in SES quintiles 2 and 3, and high SES includes people in SES quintiles 4 and 5 (the quintiles of people with the highest SES). SES classification was based on residential neighborhood defined at the 2010 census block–group level.
P values determined by using the Kruskal-Wallis test or analysis of variance for continuous variables and χ2 or Fisher exact test for categorical variables. P ≤ .05 was considered significant.
For the high-SES group, data were available for 249 patients.
The Pitt bacteremia score is widely used to determine the severity of SAB illness; it ranges from 0 to 14 points, and a score ≥4 is commonly used to indicate critical illness. 14
Use of vasopressors represents patients in septic shock.
Defined as having the first blood culture with growth of S aureus within 48 hours of admission date.
Low-risk sources were intravenous catheter–related, urinary tract infection, ear–nose–larynx, gynecologic, and manipulation-related sources; intermediate-risk sources were osteoarticular, soft-tissue, and unknown sources; and high-risk sources were endovascular, pneumonia, intra-abdominal, and central nervous system foci.
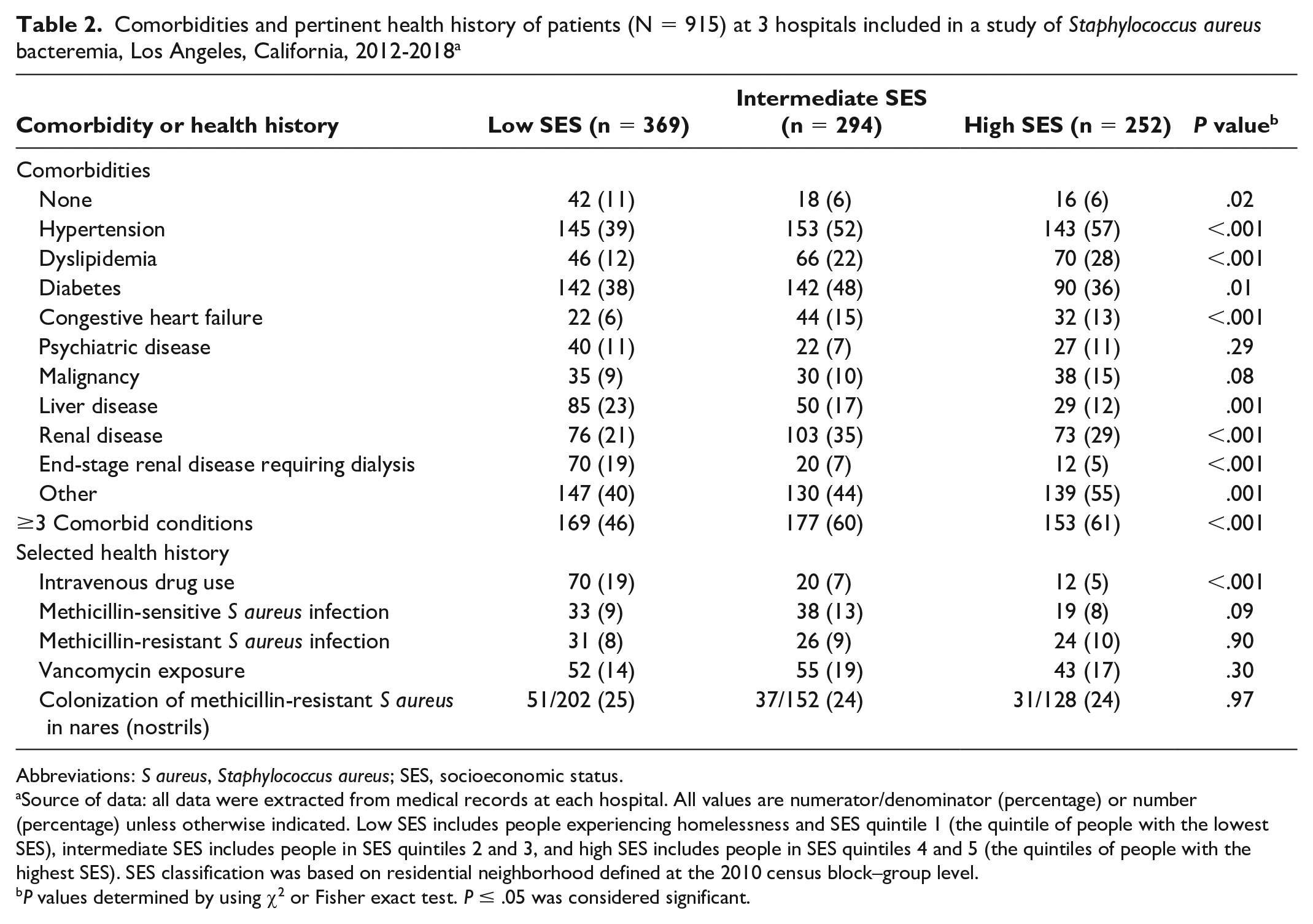
Patients in the low-SES group had significantly fewer underlying conditions than patients in the intermediate-SES and high-SES groups (Table 2). In the low-SES group, liver disease was more common among patients experiencing homelessness than among patients in quintile 1 (homeless, 34% [36 of 107] vs SES quintile 1, 19% [49 of 262]), whereas end-stage renal disease requiring dialysis was more common among patients in SES quintile 1 than among patients experiencing homelessness (SES quintile 1, 23% [60 of 262] vs homeless, 3% [3 of 106]). History of intravenous drug use was >3 times more common in the low-SES group (odds ratio = 3.72; 95% CI, 2.41-5.77; P < .001) than in the intermediate-SES and high-SES groups combined.
Comorbidities and pertinent health history of patients (N = 915) at 3 hospitals included in a study of Staphylococcus aureus bacteremia, Los Angeles, California, 2012-2018 a
Abbreviations: S aureus, Staphylococcus aureus; SES, socioeconomic status.
Source of data: all data were extracted from medical records at each hospital. All values are numerator/denominator (percentage) or number (percentage) unless otherwise indicated. Low SES includes people experiencing homelessness and SES quintile 1 (the quintile of people with the lowest SES), intermediate SES includes people in SES quintiles 2 and 3, and high SES includes people in SES quintiles 4 and 5 (the quintiles of people with the highest SES). SES classification was based on residential neighborhood defined at the 2010 census block–group level.
P values determined by using χ2 or Fisher exact test. P ≤ .05 was considered significant.
The high-SES group had the most severe presentation caused by SAB: 39 of 252 (15%) patients in this group had a Pitt bacteremia score ≥4 (vs 9% [34 of 368] in the low-SES group and 10% [30 of 293] in the intermediate-SES group; P = .04; Table 1). Skin and soft tissue was the most common source of SAB (low SES, 44% [162 of 369]; intermediate SES, 39% [114 of 294]; high SES, 43% [109 of 252]; P = .37). Catheter-associated SAB occurred similarly among low-SES and high-SES groups (16% vs 17%) but significantly more frequently in the intermediate-SES group (24%, P = .02).
Process of Care
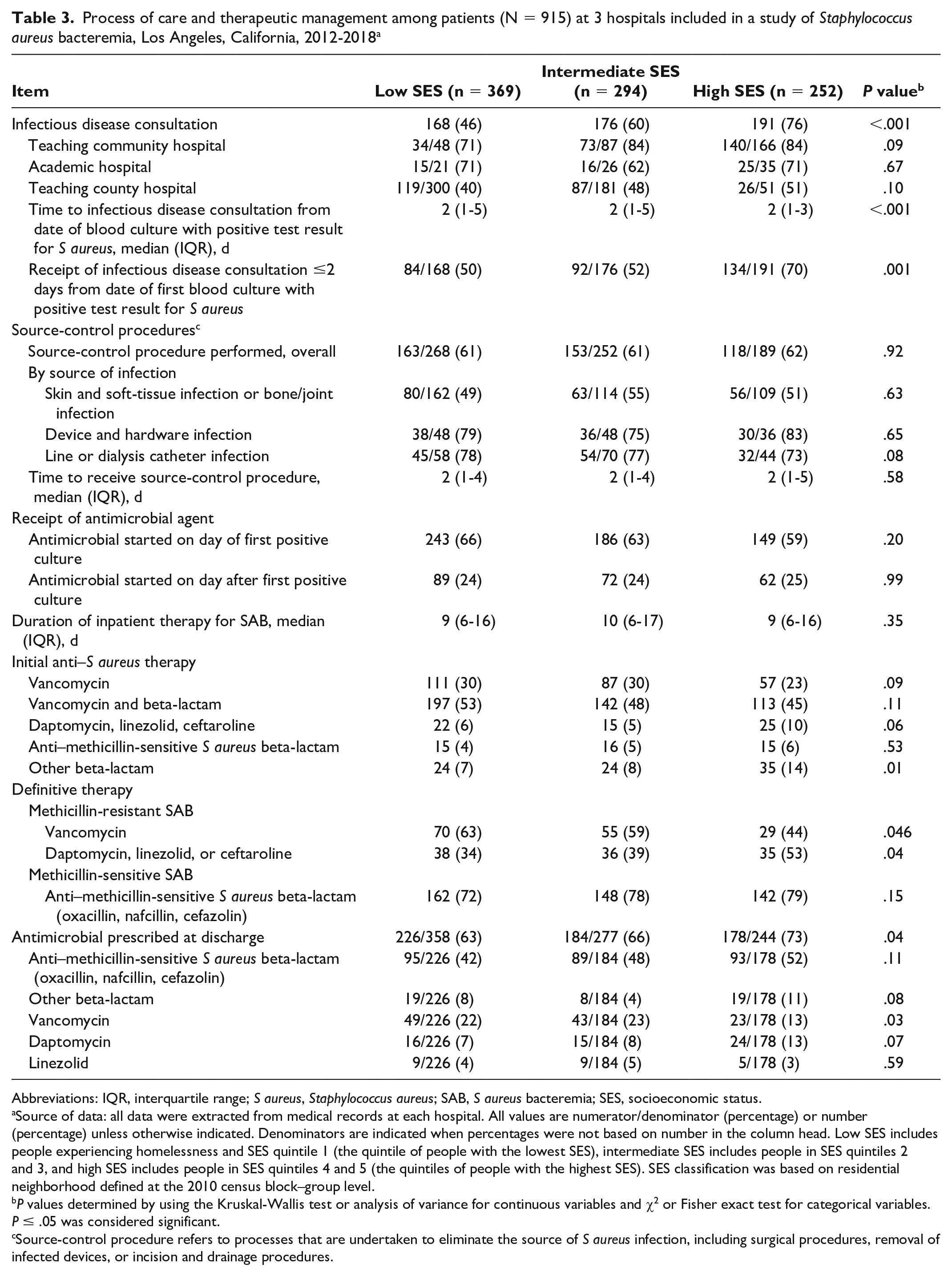
A significantly greater proportion of patients in the high-SES group received an infectious disease consultation (low SES, 46%; intermediate SES, 60%; high SES, 76%; P < .001; Table 3). The rate of infectious disease consultation was highest in the teaching community hospital (average rate, 80%) and lowest in the teaching county hospital (average rate, 46%). The intra-institutional rates of consultation were similar across the 3 SES groups. Overall, 61% (578 of 913) of patients received an in vitro–active antimicrobial on the day of a first positive blood culture. For definitive therapy for methicillin-resistant SAB, daptomycin, linezolid, or ceftaroline was significantly more common in the high-SES group (53%; low SES, 34%; intermediate SES, 39%; P = .04). The low-SES group was less likely than the intermediate-SES or high-SES group to be discharged from the hospital with antimicrobials (low SES, 63%; intermediate SES, 66%; high SES, 73%; P = .04). We observed this trend primarily among patients with endocarditis (low SES, 63% [26 of 41]; intermediate SES, 76% [22 of 29]; high SES, 94% [16 of 17]; P = .05) and among the population experiencing homelessness in the low-SES group (homeless, 40% [8 of 20] vs SES quintile 1, 86% [18 of 21]; P = .004).
Process of care and therapeutic management among patients (N = 915) at 3 hospitals included in a study of Staphylococcus aureus bacteremia, Los Angeles, California, 2012-2018 a
Abbreviations: IQR, interquartile range; S aureus, Staphylococcus aureus; SAB, S aureus bacteremia; SES, socioeconomic status.
Source of data: all data were extracted from medical records at each hospital. All values are numerator/denominator (percentage) or number (percentage) unless otherwise indicated. Denominators are indicated when percentages were not based on number in the column head. Low SES includes people experiencing homelessness and SES quintile 1 (the quintile of people with the lowest SES), intermediate SES includes people in SES quintiles 2 and 3, and high SES includes people in SES quintiles 4 and 5 (the quintiles of people with the highest SES). SES classification was based on residential neighborhood defined at the 2010 census block–group level.
P values determined by using the Kruskal-Wallis test or analysis of variance for continuous variables and χ2 or Fisher exact test for categorical variables. P ≤ .05 was considered significant.
Source-control procedure refers to processes that are undertaken to eliminate the source of S aureus infection, including surgical procedures, removal of infected devices, or incision and drainage procedures.
Clinical Outcomes
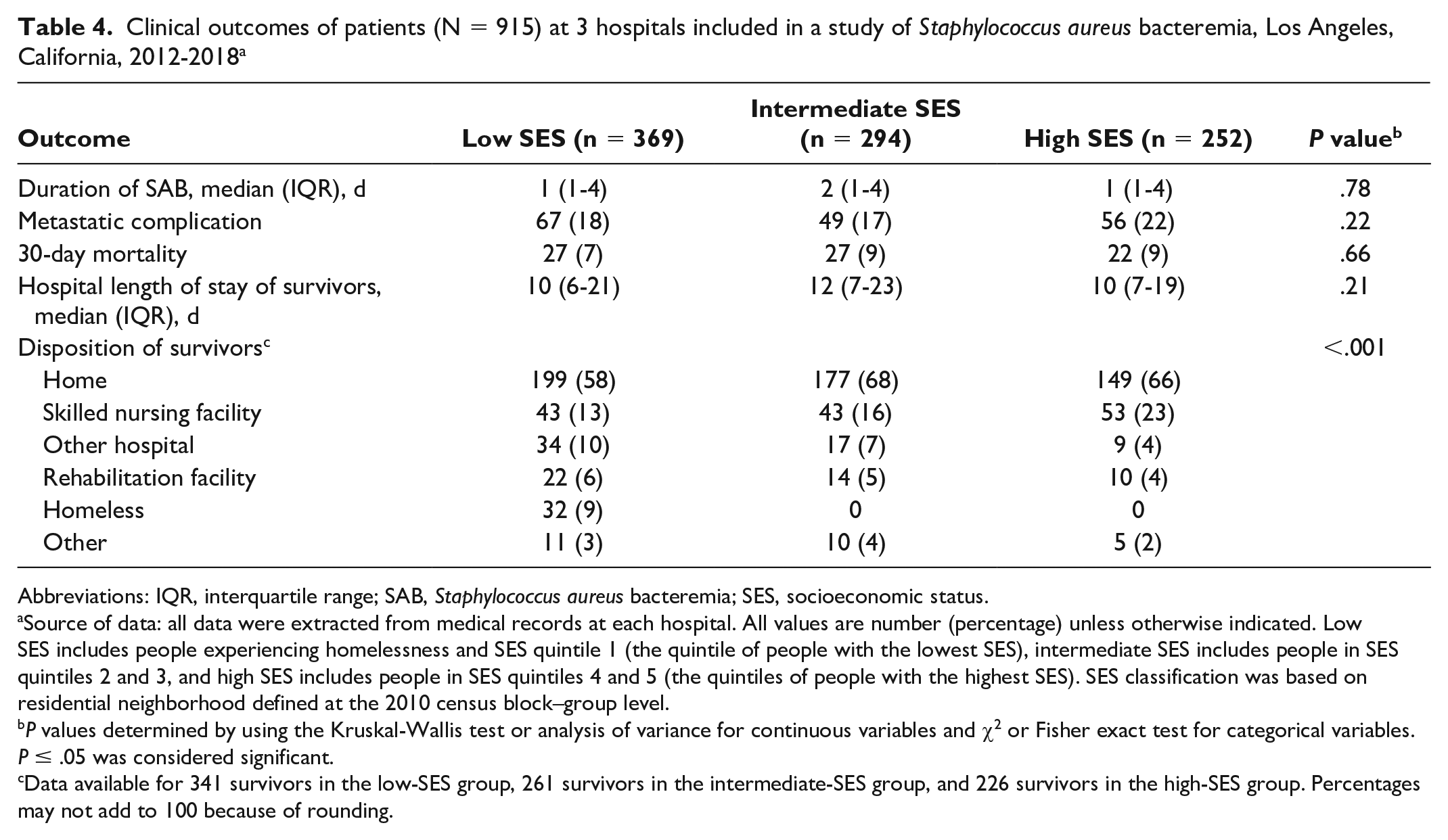
Among SAB survivors, the median length of hospital stay was similar across SES groups, at 11 days (Table 4). Length of stay was 3 days longer among patients experiencing homelessness (13 [interquartile range, 8-24] days) than among patients in SES quintile 1 (10 [interquartile range, 6-18] days; P = .01). The overall 30-day mortality rate was 8% (76 of 915). The most significant predictors of 30-day mortality in the Cox proportional hazards model were admission to an ICU (hazard ratio [HR] = 9.04; 95% CI, 4.27-19.14), having a Pitt bacteremia score ≥4 (HR = 4.30; 95% CI, 2.49-7.44), having ≥3 comorbidities (HR = 2.05; 95% CI, 1.09-3.85), and advanced age (HR = 1.03; 95% CI, 1.01-1.05; Table 5). Distance between residence and hospital was significantly associated with 30-day mortality in the low-SES group (HR = 1.02; 95% CI, 1.00-1.02) but not in the intermediate-SES group (HR = 0.99; 95% CI, 0.93-1.05) or high-SES group (HR = 1.01; 95% CI, 0.99-1.03). A sensitivity analysis (n = 805) that excluded patients experiencing homelessness had similar results. A sensitivity analysis that excluded patients with hospital-acquired SAB (n = 680) found the same significant factors as in the overall group. In addition, in this subset of patients with community-onset SAB, the distance between a patient’s residence and the hospital was significantly associated with 30-day mortality in both the high-SES group (HR = 1.02; 95% CI, 1.00-1.03) and the low-SES group (HR = 1.02; 95% CI, 1.01-1.03) but not the intermediate-SES group (HR = 0.96; 95% CI, 0.87-1.07). Among SAB survivors, patients in the high-SES group (23%) were more likely than patients in the low-SES group (13%) or intermediate-SES group (16%) to be discharged to a skilled nursing facility (P = .003).
Clinical outcomes of patients (N = 915) at 3 hospitals included in a study of Staphylococcus aureus bacteremia, Los Angeles, California, 2012-2018 a
Abbreviations: IQR, interquartile range; SAB, Staphylococcus aureus bacteremia; SES, socioeconomic status.
Source of data: all data were extracted from medical records at each hospital. All values are number (percentage) unless otherwise indicated. Low SES includes people experiencing homelessness and SES quintile 1 (the quintile of people with the lowest SES), intermediate SES includes people in SES quintiles 2 and 3, and high SES includes people in SES quintiles 4 and 5 (the quintiles of people with the highest SES). SES classification was based on residential neighborhood defined at the 2010 census block–group level.
P values determined by using the Kruskal-Wallis test or analysis of variance for continuous variables and χ2 or Fisher exact test for categorical variables. P ≤ .05 was considered significant.
Data available for 341 survivors in the low-SES group, 261 survivors in the intermediate-SES group, and 226 survivors in the high-SES group. Percentages may not add to 100 because of rounding.
Cox proportional hazards model for 30-day mortality among patients at 3 hospitals (n = 845) included in a study of Staphylococcus aureus bacteremia, Los Angeles, California, 2012-2018 a
Abbreviations: NA, not applicable; SES, socioeconomic status.
Source of data: all data were extracted from medical records at each hospital.
P values determined by using the Kruskal-Wallis test or analysis of variance for continuous variables and χ2 or Fisher exact test for categorical variables. P ≤ .05 was considered significant.
The Pitt bacteremia score is widely used to determine the severity of illness caused by Staphylococcus aureus bacteremia; it ranges from 0 to 14 points, and a score ≥4 is commonly used to indicate critical illness. 14
Low SES includes people experiencing homelessness and SES quintile 1 (the quintile of people with the lowest SES), intermediate SES includes people in SES quintiles 2 and 3, and high SES includes people in SES quintiles 4 and 5 (the quintiles of people with the highest SES). SES classification was based on residential neighborhood defined at the 2010 census block–group level.
The hazard ratio entries for terms involved in interactions are not applicable. The individual hazard ratio corresponding to each of these effects depends on other variables in the interaction term of the model. Because of the interaction term in the model, each term comprising that interaction (such as SES class and distance) is represented by specification of additional covariates in the Cox proportional hazards model.
95% Wald confidence limits.
Discussion
SES is a known factor that affects a person’s infection risk and health outcome; low SES has been reported to inversely correlate with incidence of SAB. 5 Our study, which involved 3 hospitals that serve a diverse population, gave us the unique opportunity to characterize the epidemiology, access to and process of care, and clinical outcomes of SAB using a validated SES model.
We observed significant epidemiologic differences across the SES groups. Compared with the low-SES group, the high-SES group was predominantly non-Hispanic White or Asian (69%) and more likely to have cardiovascular conditions, which may be explained by the significantly older patients in the high-SES group. In contrast, as compared with the other 2 SES groups, low-SES patients were significantly younger and had a greater percentage of Hispanic and non-Hispanic Black patients, a greater percentage of people who use intravenous drugs, and a higher incidence of end-stage organ disease involving the liver or kidneys. The higher rate of liver disease may be explained in part by social risk factors, such as intravenous drug use. 20 The higher incidence of end-stage renal disease requiring dialysis in the low-SES group is surprising because the rates of diabetes and hypertension were similar or lower in the low-SES group than in the other SES groups; however, this inconsistency could signify the underuse of health care resources to control chronic conditions. 21 Although end-stage renal or liver disease was not a significant factor in the Cox proportional hazards model (data not shown), having multiple comorbidities significantly contributed to 30-day mortality (HR = 2.05; 95% CI, 1.09-3.86). Because comorbid conditions are potentially modifiable risk factors, high priority should be placed on optimizing management of chronic conditions for all people.
Disparities in hospitalization-related care among adults with low SES have been shown to negatively affect their survival. 22 In our study, the need for ICU care or source-control procedures was not significantly different in the low-SES group than in the other 2 SES groups. However, differences in therapeutic management included a higher proportion of high-SES patients than low-SES patients receiving an infectious disease consultation (76% vs 46%, respectively). Previous studies showed that receipt of an infectious disease consultation was associated with better outcomes, because of earlier optimization of SAB management. 23 In addition, the choice of directed therapy against methicillin-resistant S aureus differed significantly, whereby the high-SES group was more likely than the low-SES and intermediate-SES groups to receive vancomycin alternatives. The differences in the rate of infectious disease consultation and receipt of vancomycin alternatives are likely explained by practice differences between hospitals. Low-SES patients were more frequently encountered at the county hospital, where the rate of infectious disease consultation was the lowest across all SES groups, whereas the high-SES group consisted of patients at the community hospital, where the rate of infectious disease consultation was the highest across all SES groups. Infectious disease consultation, hospitalization at a particular institution, or the choice of vancomycin were not found to be significant predictors of 30-day mortality by univariate analysis.
The disposition of survivors at discharge was significantly different, such that high-SES patients were more likely than low-SES or intermediate-SES patients to be discharged to a skilled nursing facility. Possible reasons for this difference include differences in health insurance coverage or differences in the functional status of older patients, who may require a higher level of care than can be provided at home. Having a history of intravenous drug use is associated with prolonged hospital stays to complete SAB treatment; discharging the patient with a catheter to receive outpatient parenteral therapy is not an acceptable option because these patients may use the catheter to administer illicit substances. 24 Options to facilitate the discharge of low-SES patients are to consider oral antimicrobial therapy after initial intravenous therapy 25 or, in selected patients with a history of intravenous drug use, to consider closely monitored outpatient parenteral antimicrobial therapy. 26
Previous research on SES and SAB showed varied results on mortality.5,27 -29 In our diverse population, overall mortality was 8%, and SES was not an independent risk factor for death. However, when we evaluated distance of residence to the hospital as a surrogate measure of access to care, we found that every mile of the patient’s residential distance from the admitting hospital added significant risk for 30-day mortality by the Cox proportional hazards model, but only in the low-SES group. Low-SES patients may not have had access to reliable and/or affordable transportation. Driving is the main source of transportation for Los Angeles County residents, yet 31% of our SES quintile-1 cohort lived in neighborhoods where an estimated quarter of residents lack access to a vehicle. 13 Previous reports similarly found higher mortality risk among patients with severe sepsis who lived far from care 30 or who resided in a medically underserved area. 31 Lack of access to ambulatory services may also lead to a high frequency of emergency department visits, especially in the homeless population. 32 Interestingly, in a sensitivity analysis that included only community-onset SAB, a longer distance from residence to the hospital negatively affected both the low-SES and high-SES groups. People in the high-SES group, because they were significantly older than people in the other SES groups and had multiple comorbidities, may have been unable to drive themselves to the hospital. Thus, the distance between the residence and health care facility must be considered a barrier to health care in the context of the individual. Possible solutions to overcome transportation barriers are expansion of telemedicine or mobile health clinics, which deploy health care teams to areas where low-SES patients congregate, to provide additional points of access.33,34
Limitations
Our study had several limitations. First, the SES measurement used an area-based aggregate approach, which was then assigned to patients. The validity of this approach relies on the homogeneity of a neighborhood population. The US Census Bureau designed census-block groups to be as homogenous as possible for population characteristics, household income, and living conditions. Therefore, by using smaller geographic units, we maximized the potential for an accurate SES measure, as previously validated in socioeconomic trials.15,18 Second, we preferentially assigned SES categorization based on SES quintiles to elucidate differentiation of SES in Los Angeles County. Nevertheless, a small number of patients fell outside Los Angeles County. These patients were given California-based SES quintile measurements and, therefore, their SES quintile ranking may be ±1 quintile relative to the county-based ranking. Third, data on several potential confounding variables could not be obtained, including detailed information related to patients’ access to care, to fully assess potential barriers other than distance of their residence from the hospital. Lastly, the availability of an outpatient parenteral antimicrobial therapy program varied by hospital, and this variability may have affected patients’ length of stay.
Conclusion
SAB is associated with significant disease and economic burden to our health care systems. SES of an individual did not significantly contribute to an individual’s risk of death. Importantly, we found that the distance between the patient’s residence and the admitting hospital significantly affected the mortality of patients in the low-SES group. These findings underscore the need to develop multipronged targeted and tailored public health efforts for vulnerable populations, given their distinct epidemiology, SES, and health risk factors. These efforts should consider transportation barriers and encompass improving access to preventive care, because having multiple comorbidities was an important contributor to poor outcomes in SAB.
Footnotes
Acknowledgements
This work was supported by grants UL1TR001855 and UL1TR000130 from the National Center for Advancing Translational Science of the National Institutes of Health (NIH). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.