
Abstract
From May through July 2020, Arizona was a global hotspot for new COVID-19 cases. In response to the surge of cases, local public health departments looked for innovative ways to form external partnerships to address their staffing needs. In collaboration with the Maricopa County Department of Public Health, the Arizona State University Student Outbreak Response Team (SORT) created and implemented a virtual call center to conduct public health case investigations for COVID-19. SORT officially launched a dedicated COVID-19 case investigation program after 3 weeks of program design and training. From June 29 through November 8, 2020, SORT recruited and trained 218 case investigators, completed 5000 case patient interviews, and closed 10 000 cases. Our team also developed process improvements to address disparities in case investigation timeliness. A strong infrastructure designed to accommodate remote case investigations, paired with a large workforce, enabled SORT to provide additional surge capacity for the county’s high volume of cases. University-driven multidisciplinary case investigator teams working in partnership with state, tribal, and local public health staff members can be an effective tool for supporting a diverse and growing public health workforce. We discuss the essential design factors involved in building a university program to complement local COVID-19 response efforts, including workflows for case management, volunteer case investigator recruitment and training, secure technology platforms for conducting case investigations remotely, and robust data-tracking procedures for maintaining quality control and timely case reporting.
In July 2020, Arizona emerged as a global pandemic hotspot, as it experienced the fastest growth of confirmed COVID-19 cases, reporting more cases per capita than any other state or country. 1 The combined burden of the state’s overwhelming case surge, a pared-down staffing model resulting from long-standing decreases in funding, and increases in community spread forced state and local public health departments to implement creative strategies to conduct case investigations and trace contacts of infected people. 2 A core function of public health assessment, case investigation allows for a review of a diagnosed person’s social history and identification of their contacts while still infectious. 3
Academic institution–public health agency partnerships (hereinafter, academic–agency partnerships) have existed since the 1970s in response to persistent disconnections between public health education and practice, and workforce development issues have been a common theme.4-6 The growing demands faced by public health systems, however, have highlighted the benefit of these models for providing auxiliary personnel to support emergency needs. 6 University partnerships can be an innovative solution for training, recruiting, and/or mobilizing a COVID-19 surge workforce to improve timeliness of case investigation and contact tracing. 7
The Student Outbreak Response Team (SORT) at Arizona State University (ASU), which has been in operation since 2017, is a service-learning and field epidemiology training program in partnership with state and local public health agencies, such as Maricopa County Department of Public Health (MCDPH). The goal of SORT is to promote future public health leadership by providing students with hands-on training and experiences in outbreak response, epidemiology, modeling, and public health preparedness.
During Arizona’s unprecedented summer 2020 surge in COVID-19 cases, SORT quickly pivoted from a small in-person public health training program to a large rapid response team composed of >200 faculty, staff members, students, and community volunteers working to mitigate the impact of the pandemic. These members represent a multidisciplinary team from fields of epidemiology, social work, anthropology, and other health-related disciplines. The long-standing programmatic infrastructure of SORT allowed for a rapid scale-up of operations, technology, and personnel in designing a virtual call center to address the county’s high volume of COVID-19 cases.
Although every external partnership has a unique structure based on local public health resources and needs, the success of any case investigation program requires case investigator recruitment, foundational and iterative training, technology platforms for conducting case investigations remotely, staffing structures, clear case-management workflows, and robust data-tracking procedures for maintaining quality control. 8 This case study discusses the infrastructure involved in operationalizing a partnered case investigation program, its adaptive potential in the face of emerging challenges, and its impact on addressing local COVID-19 case investigation capacity.
Methods
Recruitment and Training
MCDPH, the largest local health jurisdiction in the state, approached SORT in June 2020 requesting immediate support in addressing the county’s exponential surge in COVID-19 cases. In building a COVID-19 case investigation program, we focused recruitment of student and nonstudent case investigators from academic disciplines that prioritize cultural humility, strong interpersonal skills, adaptability and flexibility, and non–English-language ability. SORT developed a comprehensive training program, drawing from the multidisciplinary expertise of our core team to tackle the gaps in public health knowledge, communication, and interviewing skills among our workforce. Effective training for case investigators must explain the use of isolation and quarantine as public health tools and prepare case investigators for data collection and culturally sensitive risk communications. 9 SORT’s weeklong training involves both asynchronous and synchronous presentations, including the science of COVID-19, empathetic interviewing techniques, local public health reporting guidelines, ethical and professional conduct, and the Health Insurance Portability and Accountability Act (HIPAA). 10 Trainees also conduct role-plays and listen to mock interviews. 10 These trainings are continually updated in alignment with changing guidance from the Centers for Disease Control and Prevention (CDC) and state or local public health agencies. They are designed to improve case investigators’ levels of preparedness to confidently build rapport on the telephone and provide referrals to community resources for social support needs during isolation.
From June 29 through November 8, 2020, we recruited and trained 218 case investigators. One hundred sixty-eight (77.1%) were ASU affiliates, 93 of whom were enrolled in an associated ASU practicum course. The 50 (22.9%) case investigators who were non–ASU affiliates included AmeriCorps volunteers, retired nurses from the Arizona Nurses Association, and other community volunteers.
Technology Innovations
Technologies that provide the ability to accomplish greater feats in communication, workability, and output performance are a necessary component of rapidly implementing a case investigation program that can respond to pandemic case surges. 9 Our multilayered technology platforms—Microsoft Teams, Cisco Jabber, Twilio, Zoom, and Qualtrics Survey software—cover these criteria, enabling case investigators to perform HIPAA-aligned duties while working remotely from home without risk of infection in the workplace. 9
The foundational platform of our program is Microsoft Teams, which handles case storage, monitoring, management, and team communication. 11 All telephone communication between case investigators and case patients is conducted through Cisco Jabber, a softphone application that offers a local area code for caller identification and a voicemail box for case patients to leave messages. 12 Cisco Jabber is paired with Twilio, an instant messaging software that alerts case patients of an upcoming telephone call from our case investigators and supplies requested information on clinical and social support services. 13 Zoom is our team’s meeting hub, where case investigators sign in and work in private breakout rooms during their shifts. 14 This setup allows supervisors to quietly check on case investigators during or between calls and provide support to resolve case patient concerns promptly. The Qualtrics Survey software tool is the mechanism by which county health departments collect case information and is the main tool for communication of case investigation details between SORT and MCDPH. 15 The user-friendly features of this platform include language preference options that enable interviews to be conducted in either English or Spanish and an embedded script with key public health messaging that guides case investigators through common case investigation scenarios. These features are particularly useful because Maricopa County has 866 623 native Spanish speakers, representing 21% of the county’s overall population. 16 These interconnected technology platforms are the foundation for our work as a virtual call center and allow scale-up and flexibility as needed.
Structure of Shifts and Staffing
Scaling up a case investigation operation involves a large multidisciplinary team led by subject matter experts. 17 Our staffing structure includes a core team of principal investigators and program managers who work collaboratively to contribute to all areas of program development and operation, including training and data management systems. Case investigators sign up for 2-hour shifts to call case patients and collect case patient information. Each shift of 5-15 case investigators is monitored by 1 or 2 supervisors. Capacity is determined by constant monitoring of case investigator shift hours, productivity levels, and assigned caseloads by program managers. Our hours of operation, which started at 5 days per week from 9 AM to 8 PM before growing to 7 days per week, complements traditional business hours worked by public health partners while also improving case patient response rates.
Case Management
A working relationship between public health and academic partners requires accurate and traceable case management. MCDPH and Arizona Department of Health Services acquired partners with varying capabilities, requiring modifications to existing case management workflows to address COVID-19 case spikes from June to August 2020. As the largest county in the state, Maricopa has accounted for approximately 60% of all reported COVID-19 cases. 18 Therefore, MCDPH’s partnership objectives for external case management were 4-fold: (1) traceability of case patient progress from case assignment to case closure, (2) identification of case patients needing specialized follow-up by county official investigators, (3) updated investigation status, and (4) accurate case reporting in Arizona’s Medical Electronic Disease Surveillance Intelligence System. SORT and MCDPH had respective roles and responsibilities (Figure 1).
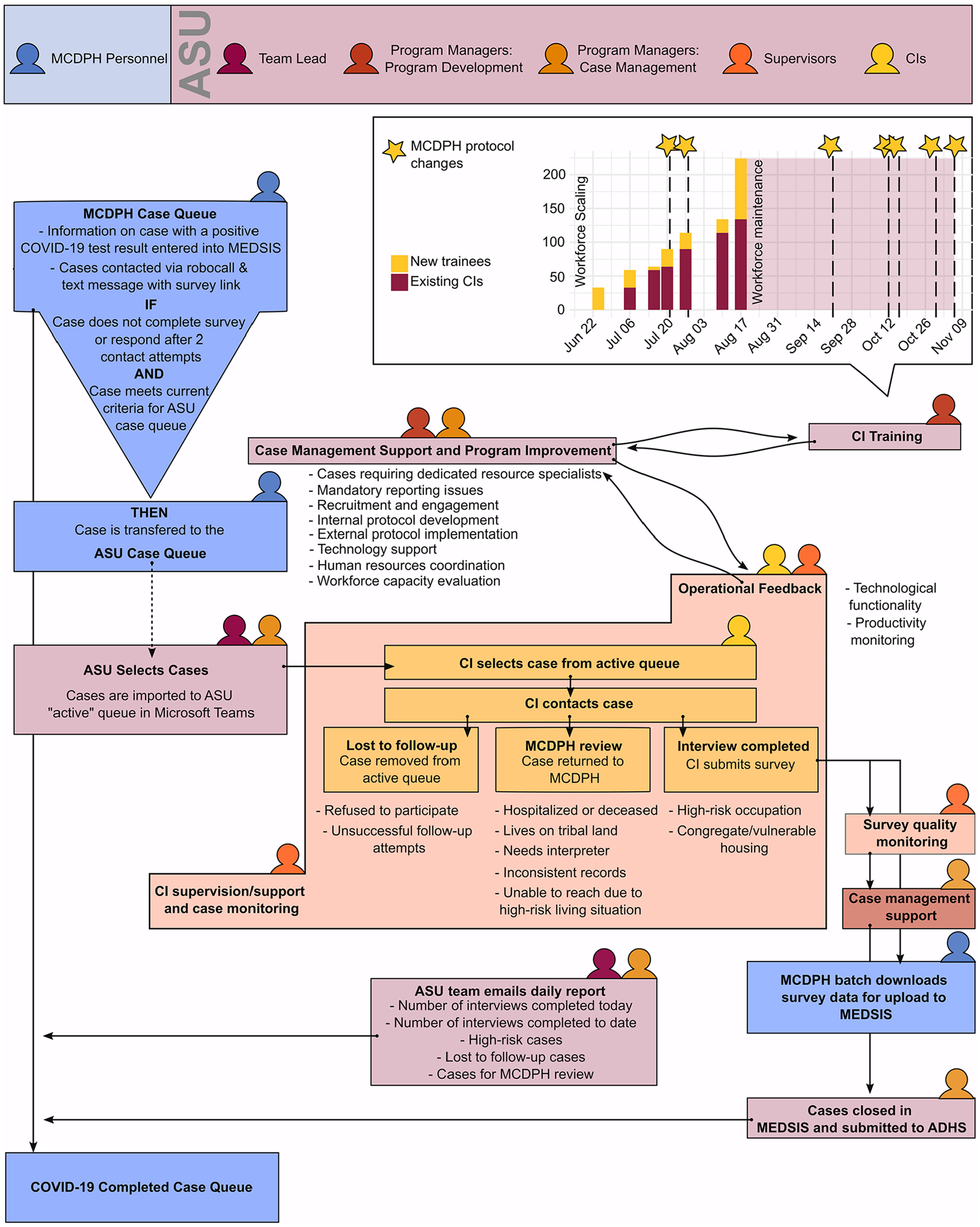
Programmatic structure of the Arizona State University (ASU) Student Outbreak Response Team case investigation program, including an organizational chart with participant roles and an overview of workforce scaling and protocol improvement implementation over time. Abbreviations: ADHS, Arizona Department of Health Services; CI, case investigator; MCDPH, Maricopa County Department of Public Health; MEDSIS, Medical Electronic Disease Surveillance Intelligence System.
Caseloads assigned to SORT have varied from low-risk case patients aged 18-65 years to school-aged case patients, to high-risk case patients aged ≥75 from non-congregate settings. Caseloads are decided by the prioritization workflows of MCDPH, availability of resources and personnel, and each partner’s core competencies. All contact attempts made by case investigators on shift are logged, including unsuccessful attempts, times to call back, voicemail histories, completed interviews, and pertinent case information that requires follow-up. Such case tracking by case investigators allows accurate case reporting, thus facilitating MCDPH’s goal of identifying case patients who require further review and provision of targeted public health messaging and guidance. Case patients are traced from the day our team receives the case report, throughout the investigation process, and to their final reporting status to MCDPH.
Data Quality and Assurance
Accurate data tracking and quality assurance helps ensure that SORT is reliable in its case reporting processes. Quality checks are conducted by 2 groups: shift supervisors who conduct on-shift case-by-case quality checks and program managers who examine all case patient interviews and special circumstances at the end of each day. Using the data analytic functions on Qualtrics, supervisors are instructed to verify that case patient information has been entered correctly, check for missing information or inconsistencies, edit response entries, and provide real-time feedback to case investigators on shift when follow-up or clarification is required. Program managers complete a final round of nightly quality checks consisting of the following procedures: (1) reconciling case investigation status between SORT and MCDPH, (2) tracing case patient progress from date of assignment to closure, and (3) confirming that Qualtrics surveys for high-risk case patients contain all necessary information for MCDPH to conduct specialized follow-up. These measures allow us to continuously monitor our adherence to our partnership objectives and identify areas for improvement in collecting timely and thorough case investigation data.
We illustrate an example of a process improvement project undertaken to reduce disparities in outcomes for Spanish-speaking case investigations, which comprise a large portion of our team’s assigned caseloads. COVID-19 has disproportionately affected the Hispanic/Latino community. 19 Our team’s original protocol for handling these case patients was to first identify Spanish-speaking case patients through the case investigation process and then flag them for follow-up by a Spanish-speaking case investigator. Although CDC recommends conducting a case investigation in a case patient’s native language, this approach can lead to longer cycle times (number of days from case assignment to case closure) if the number of case investigators with the appropriate language skills cannot meet demand. 20 The limited number of Spanish-speaking case investigators on our team posed a barrier to timely case investigation, causing the cycle time for these case patients to rise from an average of 2-4 days for English-speaking case patients to >7 days. In response, we implemented a new protocol on August 25, 2020, whereby any case investigator who encountered a Spanish-speaking case patient would ask the case patient for consent to complete the interview with a proxy or translator.
Outcomes
Implementation
SORT launched its case investigation program on June 29, 2020, after 3 weeks of program design and training. From June 29 through November 8, 2020, our team completed 5047 case patient interviews and closed out 10 543 cases (Figure 2). From October to November, we doubled our quantity of interviews completed from 2671 to 5047 and cases closed from 5340 to 10 543. During this same period, we recruited and trained 218 case investigators who contributed 5490 hours to case investigations.
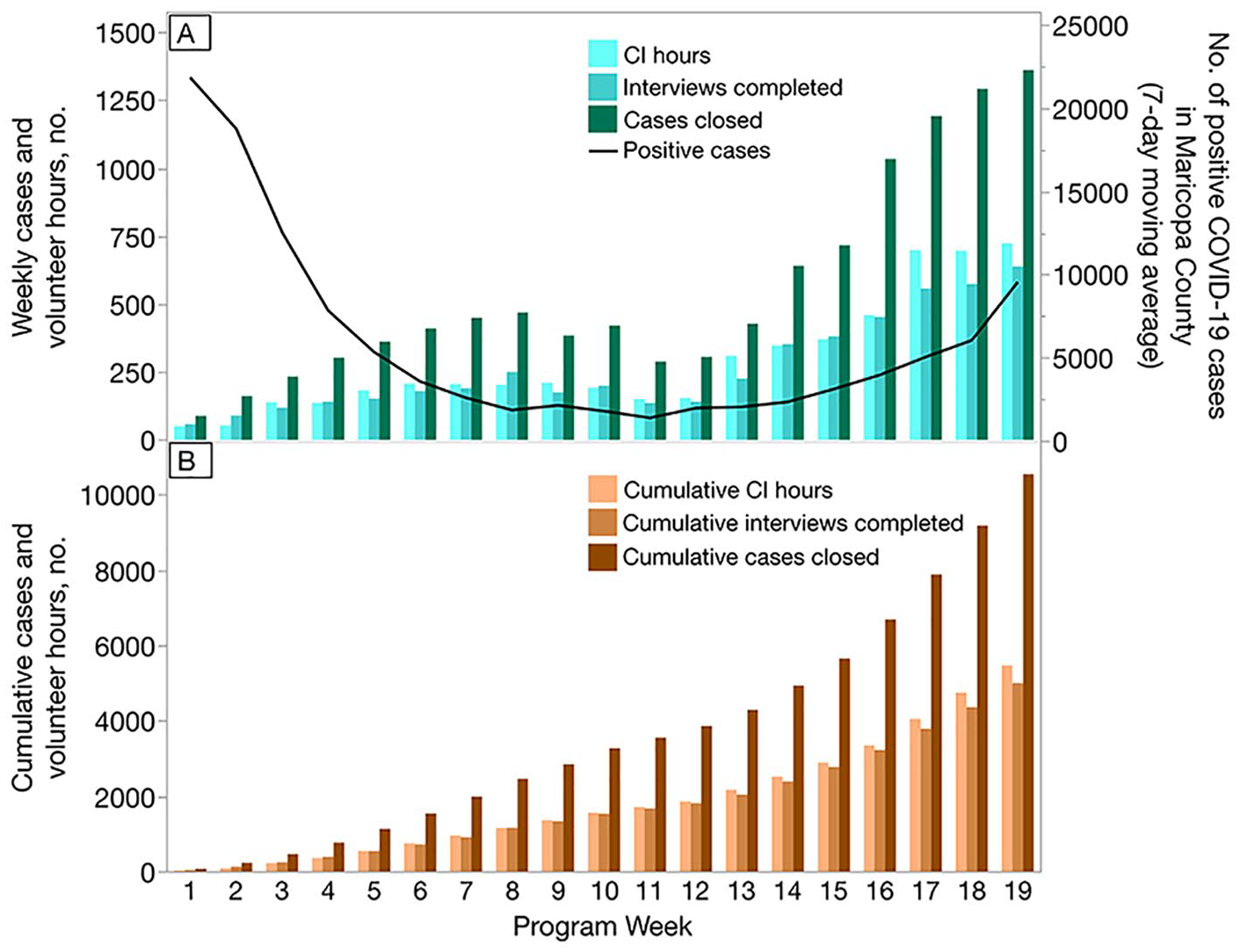
Rapid scaling of the Arizona State University Student Outbreak Response Team case investigation (CI) program, demonstrated by (A) weekly and (B) cumulative counts of completed interviews, cases closed, and case investigation hours during weeks 1-19 of the program (June 28–November 8, 2020). (A) Counts of weekly total case investigations included volunteer hours, completed interviews, and cases closed (including completed interviews and losses to follow-up). The line indicates the 7-day moving average of positive COVID-19 cases reported in Maricopa County during the same period, with the scale provided on the right y axis. (B) Counts of cumulative cases included case investigation volunteer hours, completed interviews, and cases closed, including completed interviews and losses to follow-up. Within 19 weeks, the program closed >10 000 cases.
Process Improvement Case Study Example
In response to the inequitable cycle times between English-speaking and non–English-speaking case patients, our team implemented a protocol change allowing case patients to consent to using a proxy or translator rather than waiting for a Spanish-speaking case investigator to call the patient back. Our team’s protocol change resulted in an approximately 50% reduction in cycle time, from a mean of 8.7 days to 3.6 days, leading to Spanish-speaking case patients being contacted more promptly, within fewer days of their testing and/or symptom onset date (Figure 3).
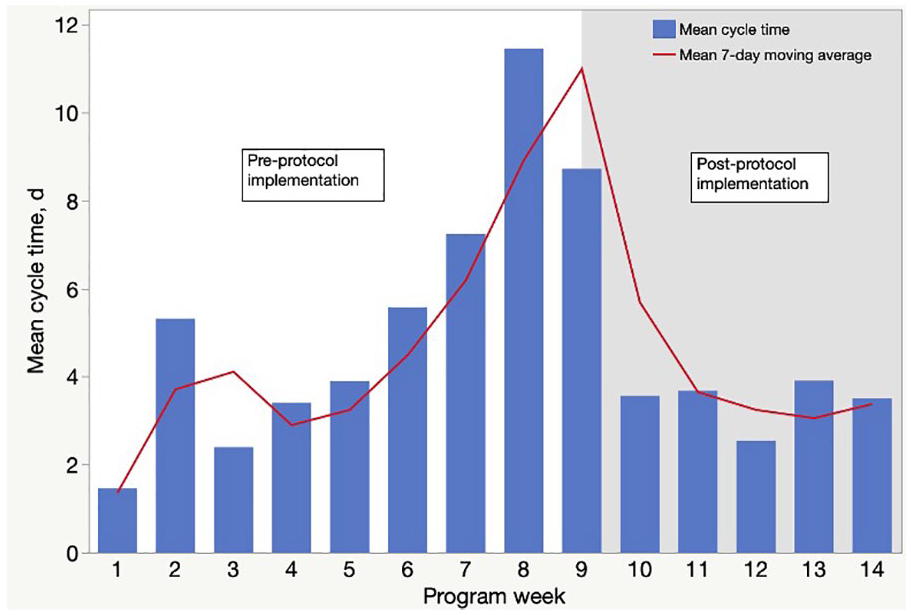
Mean cycle time for Spanish-speaking case patient management during weeks 1-14 of the Arizona State University (ASU) Student Outbreak Response Team case investigation program, showing decline in cycle time after implementation of a new communication protocol. The bars indicate the mean cycle time for Spanish-speaking case patients for weeks 1 through 14 of the program (June 28–September 28, 2020). Cycle time is the number of days a case patient spends in the ASU case queue from date of assignment to case closure, either because of interview completion or loss to follow-up. The line represents the 7-day moving average of cycle time for these case patients. The gray shaded area indicates the postprotocol implementation period. The new protocol was formed in response to the lengthy and inequitable cycle times of Spanish-speaking case patients in comparison with English-speaking case patients during weeks 1-8 and allowed investigators to offer the case patient the option of using a proxy or translator during the case investigation telephone call. This practice eliminated the bottleneck in case processing due to the abundance of Spanish-speaking cases and paucity of Spanish-speaking case investigators.
Lessons Learned
With an evolving pandemic, rapid swings in daily reported cases are known to occur, requiring creative strategies to maintain a flexible, on-demand workforce. Using productivity indicators such as the number of calls made per shift, number of interviews completed, number of high-risk case patients, and case cycle time, we can quickly estimate workforce needs and identify and prioritize areas for improvement, thus ensuring our ability to be an effective public health partner for the county. 21
From September 3 through September 27, 2020, SORT experienced a steady decline in the number of COVID-19 cases received from MCDPH, a trend consistent with statewide data from that time demonstrating the lowest incidence of positive test results for COVID-19 since the end of May 2020. During this same period, our team substantially grew as we trained an additional 93 students from an associated ASU practicum course. As a result, program managers adjusted the number and duration of case investigator shifts to better match the number of cases received each day. We assigned fewer cases to each shift so that more case investigators were able to gain at least some case investigation experience. Due to the decline in cases and truncated shifts, our team was concerned about the possibility of volunteer disengagement. Therefore, we proactively organized several virtual group activities: (1) COVID-19 journal clubs with ASU faculty, (2) guest speaker events, and (3) case investigator debriefing sessions, during which case investigators could share experiences and difficulties encountered on shift and build camaraderie.
A limitation of our wide recruitment strategy under rapid programmatic scale-up was the tradeoff between accepting volunteers with limited public health experience and offering a more diverse workforce. This tradeoff became evident through the challenges our case investigators reported facing during case investigation calls when asked technical questions about COVID-19 transmission, vaccination rollout, and contact tracing. We were able to respond to this limitation by creating supplemental frequently asked questions materials available to case investigators on shift.
Because a single-technology solution has yet to be developed, remote case investigation requires separate platforms for conducting calls, recording case information, and maintaining contact with program supervisors. 22 Simultaneous use of Zoom, Microsoft Teams, Qualtrics, and Cisco Jabber necessitates the investigator have a multitasking ability to successfully navigate all interfaces. A caveat to fully remote operations is the variability in technological competencies among case investigators. Self-reported difficulties with platform user friendliness and maneuvering efficiently between platforms by less technologically literate case investigators prompted us to embed demonstration shifts into our training program, which allowed trainees to freely practice operating the various platforms with simulated case information before their first case investigator shifts.
Slowing the spread of COVID-19 requires rapidly scaling our public health capacity at state, local, tribal, and federal levels. Early in the pandemic, national estimates suggested that the existing public health workforce was capable of providing only a fraction of the contact-tracing capacity required to meet the COVID-19 challenge. 2 In the wake of emerging infectious diseases and continued depletion of resources, academic–agency partnerships enable local public health systems to leverage an engaged and flexible workforce to readily respond to fluctuating capacity needs. 23 Virtual volunteer workforces are useful to remote public health efforts, but further research on the support offered by student outbreak response teams in conducting field epidemiology, such as door-to-door case investigation and community health assessments, is needed. 4 With a dedicated effort by multidisciplinary academic health partners, additional case patients can be reached, the effectiveness of contact tracing can be increased, and people at increased risk of infection can be prioritized.
Footnotes
Acknowledgements
The authors thank all the Arizona State University (ASU) students, community volunteers, and Maricopa County Department of Public Health (MCDPH) partners who have contributed their time and energy into helping slow the spread of COVID-19.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ASU Student Outbreak Response Team has been supported in part by the MCDPH.