
Abstract
Transgender women experience a disproportionate prevalence of HIV and barriers to linkage to care, retention in care, medication adherence, and viral suppression. As part of a national cooperative agreement funded by the Health Resources and Services Administration’s HIV/AIDS Bureau, we searched the literature from January 1, 2010, through June 1, 2020, for English-language articles on interventions designed to improve at least 1 HIV care continuum outcome or address 1 barrier to achieving HIV care continuum outcomes among transgender women diagnosed with HIV in the United States. To be included, articles needed to identify transgender women as a priority population for the intervention. We found 22 interventions, of which 15 reported quantitative or qualitative outcomes and 7 reported study protocols. Recent interventions have incorporated a range of strategies that show promise for addressing pervasive structural and individual barriers rooted in societal and cultural stigma and discrimination against transgender people. Cross-cutting themes found among the interventions included meaningful community participation in the design and implementation of the interventions; culturally affirming programs that serve as a gateway to HIV care and combine gender-affirming care and social services with HIV care; interventions to improve behavioral health outcomes; peer-led counseling, education, and navigation; and technology-based interventions to increase access to care management and online social support. Ongoing studies will further elucidate the efficacy and effectiveness of these interventions, with the goal of reducing disparities in the HIV care continuum and bringing us closer to ending the HIV epidemic among transgender women in the United States.
The term “transgender” describes a diversity of people whose gender identity and sex assigned at birth do not correspond according to traditional expectations. Although transgender people use a variety of terms to describe themselves, for the purposes of this review, we define transgender women as people assigned male sex at birth who have a feminine gender identity. This definition is commonly used for research on transgender women with HIV. 1 Transgender women experience a disproportionate prevalence of HIV compared with the general population. A 2019 systematic review estimated the prevalence of HIV among transgender women in the United States as 14.1%. 2 More than 80% of incident HIV among transgender women occurs among those who identify as Black/African American or Latina/Hispanic. 3
Transgender women with diagnosed HIV must overcome extensive challenges to progress along the HIV care continuum of linkage to HIV care, retention in care, adherence to antiretroviral therapy (ART), and viral suppression.1,4,5 Pervasive social stigma and discrimination against transgender women create vulnerability to unemployment, homelessness, food insecurity, lack of health insurance, engagement in survival sex, and incarceration.4,5 These social determinants and structural factors strongly contribute to adverse HIV health outcomes.6-8 Acute and daily exposure to abuse, harassment, bias, and discrimination among transgender women is associated with behavioral health comorbidities, such as depression, posttraumatic stress disorder (PTSD), and substance use disorders, all of which can further reduce medication adherence and engagement in HIV care.8-10 Transgender women often also mistrust health care institutions because of experiences of mistreatment and denial of services as a result of their gender identity.11-13 In addition, transgender women with HIV may prioritize gender-affirming hormone therapy over ART when they have insufficient time or finances, and some transgender women report concerns that ART will interfere with the effectiveness of hormones.14,15
To facilitate HIV care engagement for transgender women, research suggests that interventions integrate gender-affirming treatment with HIV care and use education, resources, navigation, emotional and social support, and tools to build self-efficacy, 8 reduce isolation, enhance trust with the health system, and minimize concerns of drug–drug interactions.15,16 Structural interventions are needed to create de-stigmatized and inclusive HIV clinical spaces with staff members who are transgender women themselves, health care providers trained in gender-affirming treatments, and services to meet legal, social, and behavioral health needs.17,18
Although HIV prevention studies with transgender women have been reviewed, 19 to our knowledge, no review of interventions for transgender women with HIV has been conducted. We searched the peer-reviewed literature from the past 10 years for interventions designed to help transgender women diagnosed with HIV progress along the HIV care continuum from linkage to care to viral suppression. We analyzed interventions for cross-cutting themes and public health implications related to research, implementation, replication, and scale-up. This work is part of a larger initiative, Using Evidence-Informed Interventions to Improve Health Outcomes Among People Living With HIV (E2i), which is funded by the Health Resources and Services Administration’s HIV/AIDS Bureau (HRSA HAB) of the US Department of Health and Human Services (grants U69HA31067; U90HA31099). E2i is working to eliminate disparities for transgender women and other priority populations in the Ryan White HIV/AIDS Program, which focuses on providing care and treatment services for people diagnosed with HIV. The initiative supports the identification, piloting, implementation science evaluation, and scale-up of interventions with demonstrated effectiveness at improving outcomes along the HIV care continuum for priority populations with HIV, such as transgender women, with the goal of eliminating HIV disparities and ultimately ending the HIV epidemic.20-22
Methods
We searched PubMed and PsycINFO for peer-reviewed articles published from January 1, 2010, through June 1, 2020. In our search, we used various combinations of the following terms: “transgender,” “trans,” “transsexual,” “gender identity,” “HIV,” “evaluat*,” “intervention,” “treatment outcome,” “medication adherence,” and “viral load.” To check for interventions missed by the search words, we also pursued relevant references from literature reviews. In addition, because transgender health is a growing field of research, we searched for protocols of ongoing studies in the National Institutes of Health US Library of Medicine’s clinical trials database (clinicaltrials.gov) using 2 search terms: transgender and HIV. Given the small number of completed studies of interventions for transgender women with HIV, we believed it valuable to search for and describe forthcoming intervention studies that thoroughly illustrate the scope of current research on transgender women’s HIV-related health. For similar reasons, we chose to include observational cohort studies in addition to evaluations of demonstration projects and clinical trials in instances when the study provided qualitative or quantitative data on a program developed to enhance HIV care continuum outcomes for transgender women with HIV.
Eligible studies met all of the following criteria: (1) identified transgender women as a priority population for the study and, if reported, had a sample of at least 10% transgender women with HIV; (2) described an intervention focused primarily on improving at least 1 HIV care continuum outcome for transgender women diagnosed with HIV (linkage to care, engagement/retention in care, ART adherence, or viral suppression) or 1 barrier to achieving HIV care continuum outcomes (eg, psychosocial factors, access-to-care barriers, stigma-related barriers); (3) the study was conducted in the United States, which is where most studies with this population have occurred; and (4) the article was written in English. After selecting intervention studies based on eligibility criteria, we reviewed the interventions for cross-cutting themes and strategies.
Results
Our search yielded 22 interventions, of which 15 reported outcome data or lessons learned (Table 1),18,23-36 and 7 published a study protocol (Table 2).37-43 One article reported on 2 interventions. 35 The participant populations of 11 interventions exclusively comprised transgender women with HIV.25,28,29,31-33,35,37,39,42 An additional intervention exclusively included transgender and nonbinary people. 40 Six interventions did not report a number or percentage of transgender women but explicitly recruited transgender women18,24,34,38,41,43; all other interventions reported sample populations of 11% to 45% transgender women with HIV.25,27,30,40 Five interventions came from a multisite demonstration project funded by the Special Projects of National Significance (SPNS) program, Enhancing Engagement and Retention in Quality HIV Care for Transgender Women of Color (2012-2017). 44
HIV care continuum interventions for transgender women with HIV in the United States, January 1, 2010, through June 1, 2020
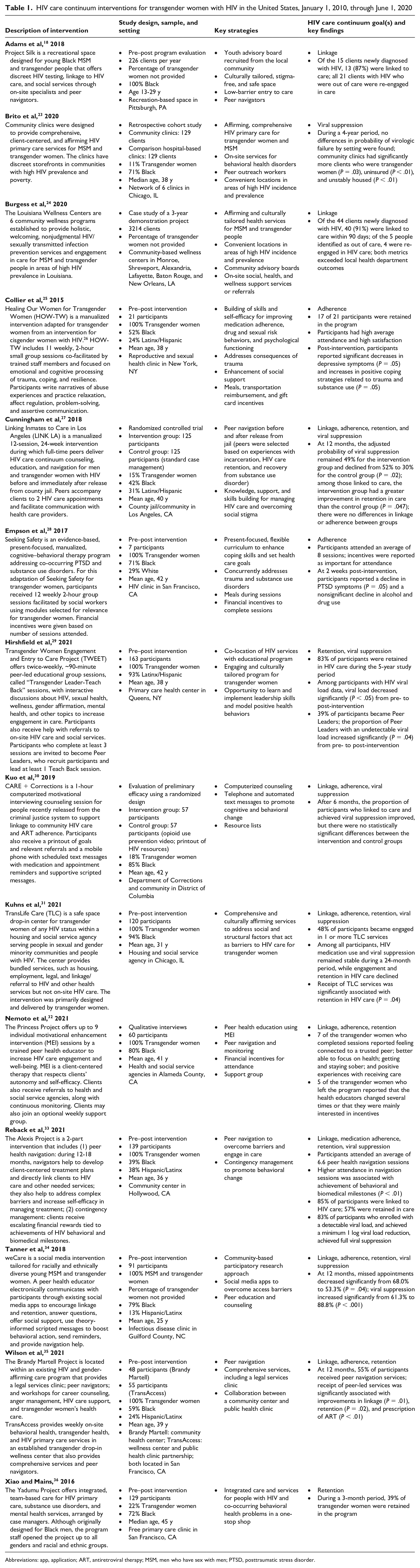
Abbreviations: app, application; ART, antiretroviral therapy; MSM, men who have sex with men; PTSD, posttraumatic stress disorder.
Study protocols of HIV care continuum interventions for transgender women with HIV in the United States
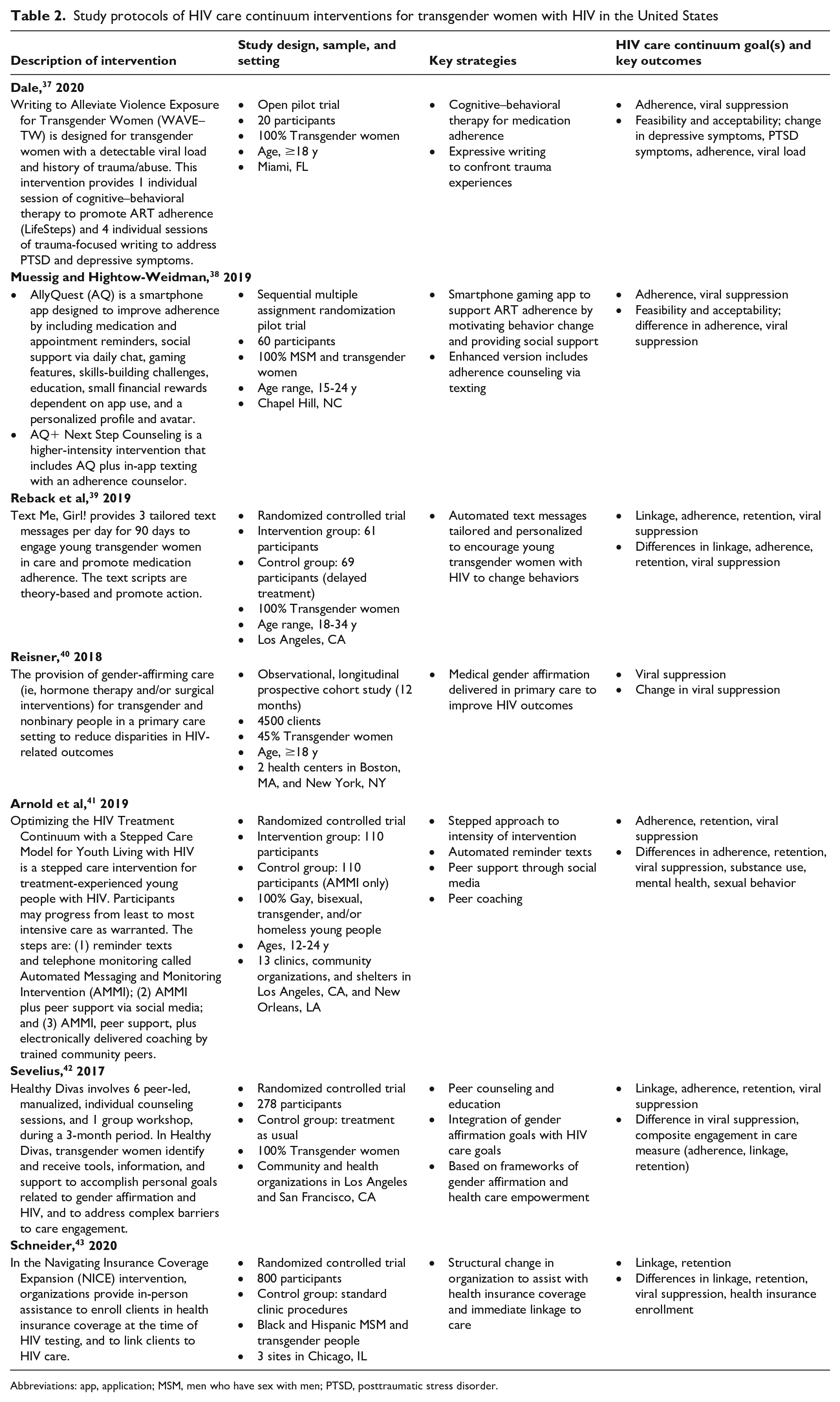
Abbreviations: app, application; MSM, men who have sex with men; PTSD, posttraumatic stress disorder.
Cross-cutting Themes
The 22 interventions implemented a range of strategies to overcome individual and structural barriers to linkage, retention, medication adherence, and viral suppression for transgender women with HIV. A common theme reported by most interventions was the formation of collaborative partnerships between transgender women community members and project staff members to overcome structural barriers and create culturally relevant programs that meet the most pressing needs of the local population of transgender women. Meaningful community participation gives voice to the concerns of priority populations, while increasing the potential for an intervention’s acceptability and sustainability. 45 Some interventions involved transgender women in the development of curricular topics and content29,32,33,38,39,42; other interventions formed community advisory boards or used community-based participatory research methods to assess needs and interests and to provide ongoing feedback as the intervention or program continued.18,24,34
Another common strategy across many interventions to overcome structural barriers involved the creation of programs, support groups, or recreational and drop-in spaces as a gateway for transgender women to engage in HIV care.18,23,24,29,31,32,35,42 These programs offered a low-barrier and appealing entry to health care institutions by providing opportunities for social connections, information on a range of health and wellness topics, legal assistance for name change and immigration, employment counseling, and other services that transgender women may prioritize over HIV care. Colocation of HIV care with these programs and services reduced transportation and other access barriers while increasing comfort with and trust in the organizations and health care providers and offering a continuum of services. HIV care interventions that combine gender-affirming care with HIV care, or that offer comprehensive services, have a similar advantage in that transgender women may initially come for gender-affirming medical care, housing, substance use disorder, or other services and eventually access HIV care. 46 Likewise, transgender women who initially come for HIV care may be more likely to remain in care if the same location offers support for psychosocial and subsistence services. Importantly, these organizations strived to offer welcoming and nonjudgmental services for transgender women, a critical need for a population that experiences high levels of stigma in health care and public services. 47
Several interventions trained transgender women peers to deliver education, counseling, social support, or navigation as an implementation strategy.18,23,27,29,32-35,41,42 Peer delivery is a method for boosting the efficacy and cultural relevancy of an intervention.46,48 Because peers have similar demographic characteristics to participants, they can serve as role models, develop caring relationships with clients, and provide culturally attuned communication and insight. 49 In 3 interventions, transgender women peers provided education and counseling during in-person individual or group sessions29,32,42; 2 interventions provided remote coaching and education through social media.41,43 Peer sessions were designed to motivate and build self-efficacy to engage participants in HIV care, while respecting and integrating the participant’s gender affirmation and other personal health and wellness goals. The Transgender Women Engagement and Entry to Care Project (TWEET) intervention implemented a unique strategy of having peer training and leadership as a core element, thus further enhancing the skills and agency of participants. 29 In several interventions, peers served as patient health navigators.18,27,32,33,35 Patient navigation is another strategy that leverages trusting and caring relationships with either peers or case manager social workers to support people who are newly diagnosed with HIV or who are out of care to connect to recommended services. 50
Four interventions focused primarily on addressing mental health and substance use as individual barriers to engagement in HIV care.25,28,36,37 A free clinic provided integrated care for people with co-occurring HIV, substance use, and psychiatric disorders but retained only 39% of transgender women. 36 The other 3 interventions adapted existing interventions to support transgender women with histories of trauma and, in 1 intervention, co-occurring substance use disorders.25,28,37 These interventions used evidence-based methods, such as expressive writing, cognitive processing, and cognitive–behavioral therapy, to increase coping skills and reduce symptoms of trauma and depression.
Behavioral economics theory purports that contingency-based financial rewards can motivate behavioral change. 51 The Alexis Project intervention augmented a peer health navigation intervention with escalating financial rewards tied to achievements along the HIV care continuum. Other interventions granted monetary incentives for attendance in program sessions. As noted previously, many transgender women with HIV experience dire economic hardships.25,28,32 Cash incentives, or small culturally relevant gifts, may motivate some transgender women to change health behaviors, although questions remain about the long-term sustainability of this strategy. 51
Technology-based health interventions are becoming increasingly common because of the nearly ubiquitous use of smartphones, tablets, social media applications (apps), and personal computers. Advantages include ease and low cost of scale-up, ability to reach people who otherwise may not access health venues, potential to support self-efficacy and self-management of HIV care, and social support from others with shared HIV status.52,53 Although smartphone interventions hold promise for reaching and engaging young transgender women as well as people in various sexual and gender minority groups, their feasibility and sustainability have come into question because young people often lose or change cell phones. 54 We found 5 technology-based interventions that primarily used scripted, automated, or personalized text or social media messaging to support medication and appointment adherence and to inspire behavioral change.30,34,38,39,41 Some interventions also included gaming features, rewards, calendar reminders, and peer social support,30,34,38 and one is testing a stepped method that adds on remote counseling for participants who did not respond to the more basic package. 41
Discussion
Because this narrative topical review was focused on thematic synthesis, we summarized but did not systematically evaluate the methods or outcomes of each study. Overall, we found that the study designs and methodologies were not robust. Two studies reported only qualitative and program evaluation data,24,32 and most studies with quantitative outcomes used nonrandomized designs, with the most frequent design being pre–post intervention.18,25,28,29,31,33-36 Although only 2 of the completed intervention studies were randomized controlled trials,27,30 5 study protocols described randomized designs,38,39,41-43 indicating that more rigorous research is forthcoming. In addition, several interventions were conducted as part of the Enhancing Engagement and Retention in Quality HIV Care for Transgender Women of Color multisite initiative with transgender women of color, from which additional findings will be published in 2022.44,55
All studies with pre–post designs found at least 1 positive, significant effect on an HIV care continuum outcome or mediator of HIV care continuum outcomes, indicating their potential for randomized trials and broader scale-up.18,25,28,29,31,33-36 Given the variation and weaknesses in study designs and measurement of outcomes, as well as variations in strategies, settings, and populations, it would not be possible to derive conclusions about the efficacy of the interventions, even with a systematic or meta-analytic approach. Moreover, because many of the interventions were holistic interventions with multiple components, their complexity makes it difficult to isolate the factors that contributed to an intervention’s success. Given the practical challenges of evaluating multilevel and holistic interventions for transgender women with traditional study designs, using an implementation science evaluation framework may prove helpful for understanding which interventions are effective for transgender women with HIV. 20 In addition, mixed-method study designs with both quantitative and qualitative components could help to disaggregate broader findings about effectiveness.
Another challenge for researchers is the recruitment of enough transgender women with HIV to achieve sufficient sample size. Reasons why transgender women may not participate in research include a lack of time or transportation, concerns about stigma related to being transgender and having HIV, mistrust in the motivations of researchers, and possibly low levels of acceptance of randomized trials that deny control groups an opportunity to engage in an intervention.56,57 It is therefore notable that 5 studies in our review recruited more than 100 transgender women.29,31,33,39,42 These relatively large sample sizes suggest that interventions for this population are feasible, acceptable, and desired. It is also worth noting that most studies were conducted in clinics or community-based organizations rather than research facilities, making their findings potentially relevant to organizations with similar resources and populations of focus.18,23-35,40-43
Public Health Implications
Interventions for transgender women must overcome complex structural, systems-level, and individual-level barriers, yet still be feasible to implement. Through the E2i initiative and other projects funded through SPNS, HRSA HAB is applying insights from implementation science to accelerate the identification and scale-up of interventions for transgender women and other priority populations across the Ryan White HIV/AIDS Program.20-22 The goal of these projects is to widely disseminate best practices, findings, and lessons learned through publications and broadly accessible implementation toolkits to guide replication and adaptation at Ryan White HIV/AIDS Program sites and other direct service organizations. The TWEET and Healthy Divas interventions have recently been piloted and evaluated at 6 Ryan White HIV/AIDS Program–funded sites in diverse geographic areas as part of HRSA HAB’s E2i initiative.21,22 The initiative is using an evaluation plan adapted from the Proctor Model 58 that allows simultaneous assessment of HIV health outcomes along with the implementation strategies that drive successful uptake and organizational integration of the interventions. Future products from this and other SPNS initiatives will help to eliminate persistent gaps in outcomes along the HIV care continuum for transgender women.
To achieve HIV health equity for transgender women in the United States, it is critical to develop, implement, and disseminate interventions that break down pervasive structural barriers rooted in societal and cultural stigma and discrimination toward transgender people, while supporting empowerment of transgender women to make choices that improve their health and well-being.46,49 The findings of this topical review suggest that recent interventions have incorporated strategies that show promise for addressing barriers to engagement of transgender women along the HIV care continuum. Forthcoming publications from ongoing studies will further elucidate the efficacy and effectiveness of these interventions, with the goal of reducing disparities and ending the HIV epidemic among transgender women in the United States.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alex S. Keuroghlian and Sari L. Reisner will receive royalties as editors of a McGraw Hill textbook on transgender and gender diverse health care.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work and this study were supported by the US Department of Health and Human Services, Human Resources and Services Administration grant no. U69HA31067.
Disclaimer
The views expressed in this article are solely the opinions of the authors and do not necessarily reflect the official policies of the US Department of Health and Human Services or the Health Resources and Services Administration, nor does mention of the department or agency names imply endorsement by the US government.