
Abstract
Objectives:
Given several efforts to improve health care access in California and nationally, we studied whether linguistic and socioeconomic disparities in health care access changed from 2011 to 2019 among Asian and Pacific Islander American (APIA) people in Los Angeles, California.
Methods:
We analyzed survey responses from APIA health fair participants (n = 5032) in the Greater Los Angeles area from May 15, 2011, through October 20, 2019. To assess the effect of socioeconomic factors on and shifts in health care access (ie, health insurance status/regular doctor), we used a logistic regression model. Covariates included English proficiency, year, age, sex, ethnicity, income, employment, and education. We also ran an interaction analysis between English proficiency and year.
Results:
Health insurance access increased and doctor access remained stable throughout the study period; however, disparities in health insurance status widened by a factor of 1.08 per year between participants with high English proficiency (HEP) and participants with low English proficiency (LEP) (P = .01). People with HEP were 2.02 times more likely to have a regular doctor than people with LEP (P < .001), and this disparity persisted from 2011 to 2019 (P = .58). Participants who were young (P < .001) and male (P = .005) were significantly less likely to have health insurance and a regular doctor (P < .001) than participants who were older and female. Chinese participants were significantly more likely than Thai (P = .002) and Korean (P < .001) participants to be insured but not more likely to have a regular doctor, when controlling for health insurance.
Conclusions:
Policy changes targeting language and cultural barriers to care for APIA people with LEP may address the disparities observed.
Keywords
The Asian and Pacific Islander American (APIA) population is among the fastest growing in the United States, increasing 72% from 2000 to 2015. 1 Furthermore, the APIA population constitutes large portions of the population of people with low English proficiency (LEP), composing 20% of people with LEP in Los Angeles, California. 2 APIA people with LEP are less likely than their counterparts with high English proficiency (HEP) to have health insurance and a regular source of care, resulting in poor health outcomes and unmet mental health needs.3-7 Notably, even after enrolling in health insurance, APIA people with LEP have faced difficulty accessing care compared with APIA people with HEP. 8 In the last decade, considerable efforts have been made to improve health care access in the United States. Studies have shown a narrowing in health care access disparities resulting from language barriers during this period; however, these studies included only non-APIA people.9,10 Therefore, it is unclear if this trend also applies to APIA people. Given that previous studies have shown the effect that LEP has on health care access in the APIA community, it is important to examine how these disparities resulting from language barriers have changed in this population.
In addition to English proficiency, other socioeconomic factors (eg, age, sex, income, race, ethnicity) have been shown to predict health care access.11-14 In particular, men, young people, and those with low income are less likely to have health insurance and doctor access than women, older people, and those with high income.11-14 Although these characteristics are well researched, many studies aggregate the APIA population into 1 racial category despite a large diversity of ethnicities with differential health care access within this group. 15 This aggregation has led to an incomplete appreciation of the status of health care access among some APIA groups. A better understanding of differential health care access among APIA subgroups is key to inform policies and programs aimed at improving population health.
We sought to fill the gap in the literature by examining annual changes in health insurance and health care access between APIA people with LEP and APIA people with HEP in the context of recently implemented public policies, such as the Affordable Care Act. We also evaluated the role other social factors play in health insurance status and regular doctor access. We hypothesized that health insurance and doctor access would increase during the study period for both APIA people with LEP and APIA people with HEP and that disparities in health care access resulting from English proficiency would decrease.
Methods
Data Collection and Study Population
The data used for our study were provided by the University of California, Los Angeles (UCLA), organization APA Health CARE and collected through surveys administered at community health fairs from May 15, 2011, through October 20, 2019, in the Greater Los Angeles area. Methods of data collection and handling are detailed elsewhere. 16 The health fairs provided basic health screenings and were mainly conducted at cultural festivals and places of worship within APIA ethnic enclaves. The UCLA Institutional Review Board deemed this retrospective analysis of data collected to be exempt from review. All participants provided informed written consent.
Variables of Interest
Our outcomes of interest were participants’ health insurance status and regular doctor access. We determined the binary value (1 = yes, 0 = no) for each variable by using participant responses to survey questions. For health insurance status, participants answered the question, “What health insurance?” and had the option to either state their type of health insurance in free response format or answer “no insurance.” Participants who stated health insurance were grouped into the yes category. For regular doctor access, participants responded yes or no to the question, “Do you have a regular doctor?”
We grouped participant self-reported English proficiency into either HEP or LEP based on responses to the survey question on English level according to criteria developed by Yang et al. 16 We placed participants who responded “very well” or “well” in the HEP category and participants who responded “not well” or “not at all” in the LEP category.
We also included several covariates related to participant demographic characteristics and socioeconomic status, including age, sex, ethnicity, education level, employment status, and annual household income. We included the year of the health fair visit to gauge temporal changes.
Statistical Analysis
Data imputation
During the 9-year study period, 6260 survey responses were collected. We excluded 1140 responses because they were not completed by members of the APIA population (Figure 1). To ensure that each observation was independent, we removed 88 second occurrences from participants who visited a health fair twice during the study period, leaving 5032 responses for analysis. To curtail the bias introduced by incomplete data, we used multiple imputation. 17 Based on the formula by van Buuren 18 for selecting the number of imputations to perform, we imputed 40 completed datasets. Before fitting the analytical model on the imputed datasets, we excluded participants who were originally missing a response for the outcome variable of interest in that model. We pooled the results of the statistical analyses on all imputed datasets.
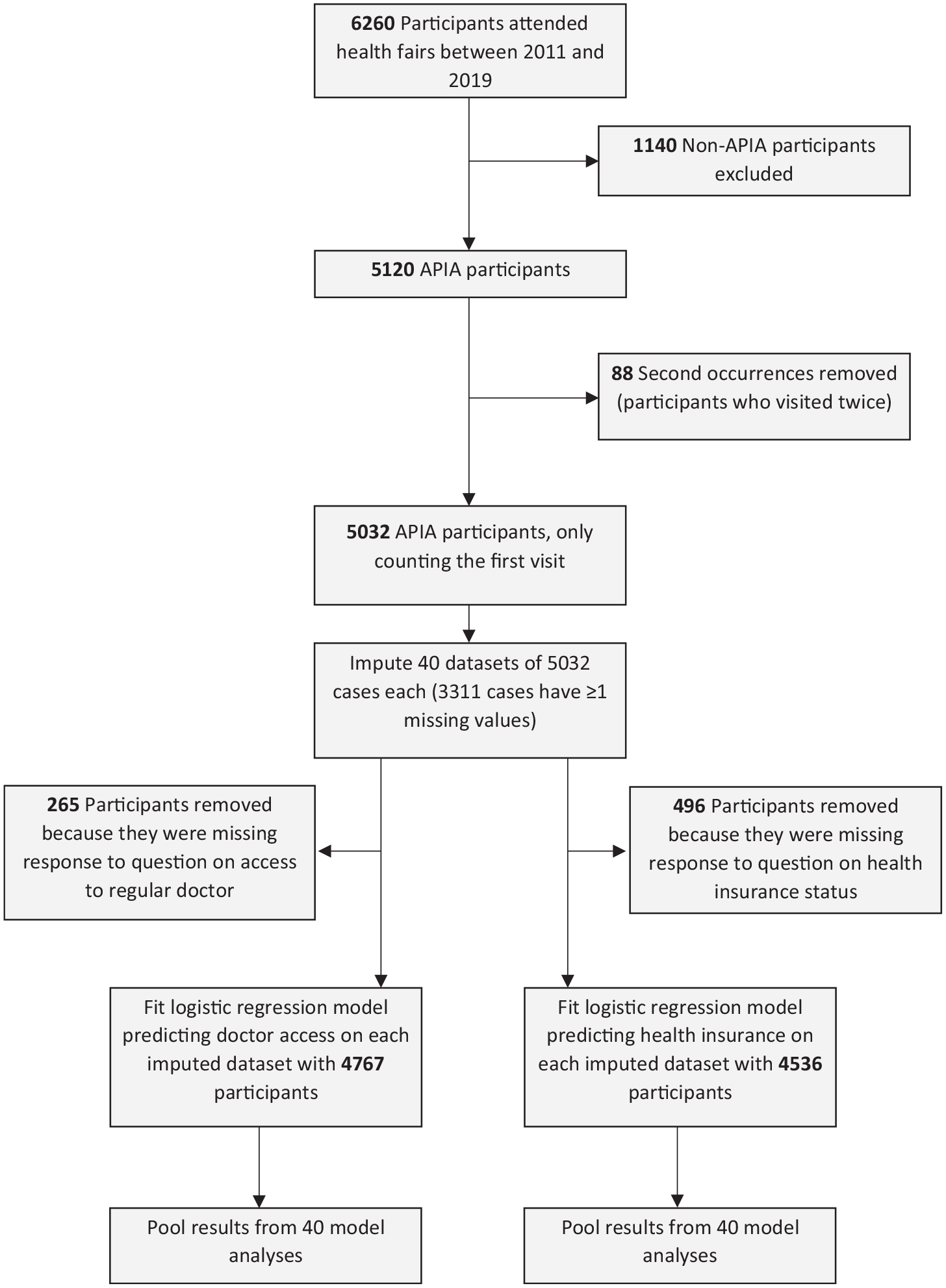
Flowchart detailing exclusion criteria and progression of analysis for the aggregate logistic regression model of health care access for APIA health fair participants in Los Angeles, 2011-2019. Abbreviation: APIA, Asian and Pacific Islander American.
Logistic Regression Analysis
We investigated 2 main study areas: (1) shifts in participant health care access during the 9-year study period and (2) the relationship between participant socioeconomic factors and health care access. Because the 2 outcome variables of interest were binary, we used a logistic regression model for each.
To investigate predictors of health care access, we used a logistic regression model with health insurance as the outcome variable and socioeconomic characteristics (age, sex, income, employment, ethnicity, English proficiency, education) and year of visit as covariates. We repeated the same procedure with doctor access as the outcome variable and health insurance added as a covariate. In preliminary analysis, we found that treating year as a categorical variable did not significantly improve our model’s predictive ability. Therefore, we included year as a continuous variable for all analyses.
To assess the persistence of health care access disparities resulting from English proficiency, we also conducted an analysis that included an interaction variable between English proficiency and year of visit for both models. For this part of the analysis, we modeled each outcome variable as a function of year and English proficiency. Using a logistic regression, we found significant interaction (P = .01) between English proficiency and year in the health insurance model; we found no such significant interaction in the regular doctor access model; thus, we removed the interaction term from the latter model. We considered P < .05 to be significant. We performed all analyses in R version 4.0.2 (RStudio).
Results
Most participants were aged 51-64 years (48.6%), Chinese (50.4%), and female (62.3%), and earned <$20 000 per year (57.9%) (Table 1). Participants’ incomes increased during the study period.
Demographic characteristics of Asian and Pacific Islander American (APIA) health fair participants, Los Angeles, 2011-2019 a
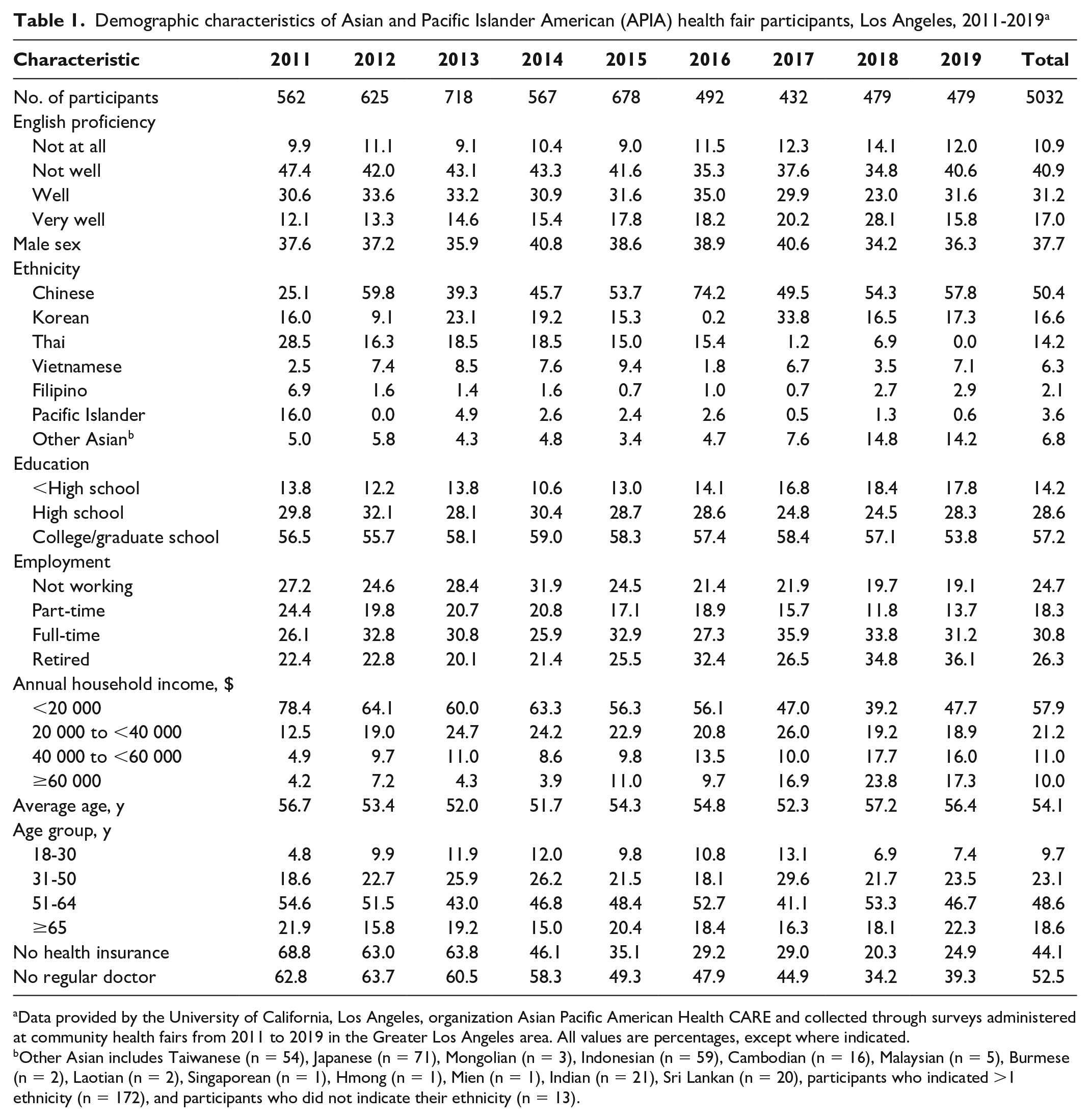
Data provided by the University of California, Los Angeles, organization Asian Pacific American Health CARE and collected through surveys administered at community health fairs from 2011 to 2019 in the Greater Los Angeles area. All values are percentages, except where indicated.
Other Asian includes Taiwanese (n = 54), Japanese (n = 71), Mongolian (n = 3), Indonesian (n = 59), Cambodian (n = 16), Malaysian (n = 5), Burmese (n = 2), Laotian (n = 2), Singaporean (n = 1), Hmong (n = 1), Mien (n = 1), Indian (n = 21), Sri Lankan (n = 20), participants who indicated >1 ethnicity (n = 172), and participants who did not indicate their ethnicity (n = 13).
Socioeconomic Factors Associated With Health Care Access
Using pooled logistic regression analyses, we found that all socioeconomic variables evaluated were independently associated with health care access (Table 2). Compared with participants with LEP, participants with HEP were 2.13 times more likely to be insured (P < .001) and 2.02 times more likely to have a regular doctor (P < .001). Although only participants aged ≥65 years were significantly more likely to be insured than participants aged 18-30 years (P < .001), participants aged 31-50 years (P = .04), 50-65 (P < .001), and ≥65 years (P < .001) were all significantly more likely to have a regular doctor than participants aged 18-30 years. Compared with male participants, female participants were significantly more likely to be insured (P = .01) and have a regular doctor (P < .001). Compared with participants who earned <$20 000 per year, participants with an annual household income ≥$20 000 were significantly more likely to have access to health insurance (P < .001), and participants with an annual household income of $40 000-$60 000 (P = .01) and >$60 000 (P < .001) were significantly more likely to have a regular doctor. Finally, although Thai (P = .002) and Korean (P < .001) participants were significantly less likely to have access to health insurance than Chinese participants, Thai (P = .002), Vietnamese (P < .001), Filipino (P = .04), and Pacific Islander (P < .001) participants were all significantly more likely to have a regular doctor than Chinese participants when controlling for health insurance status.
Multivariate logistic regression showing adjusted relative odds of health insurance and regular doctor access in Los Angeles, 2011-2019 a
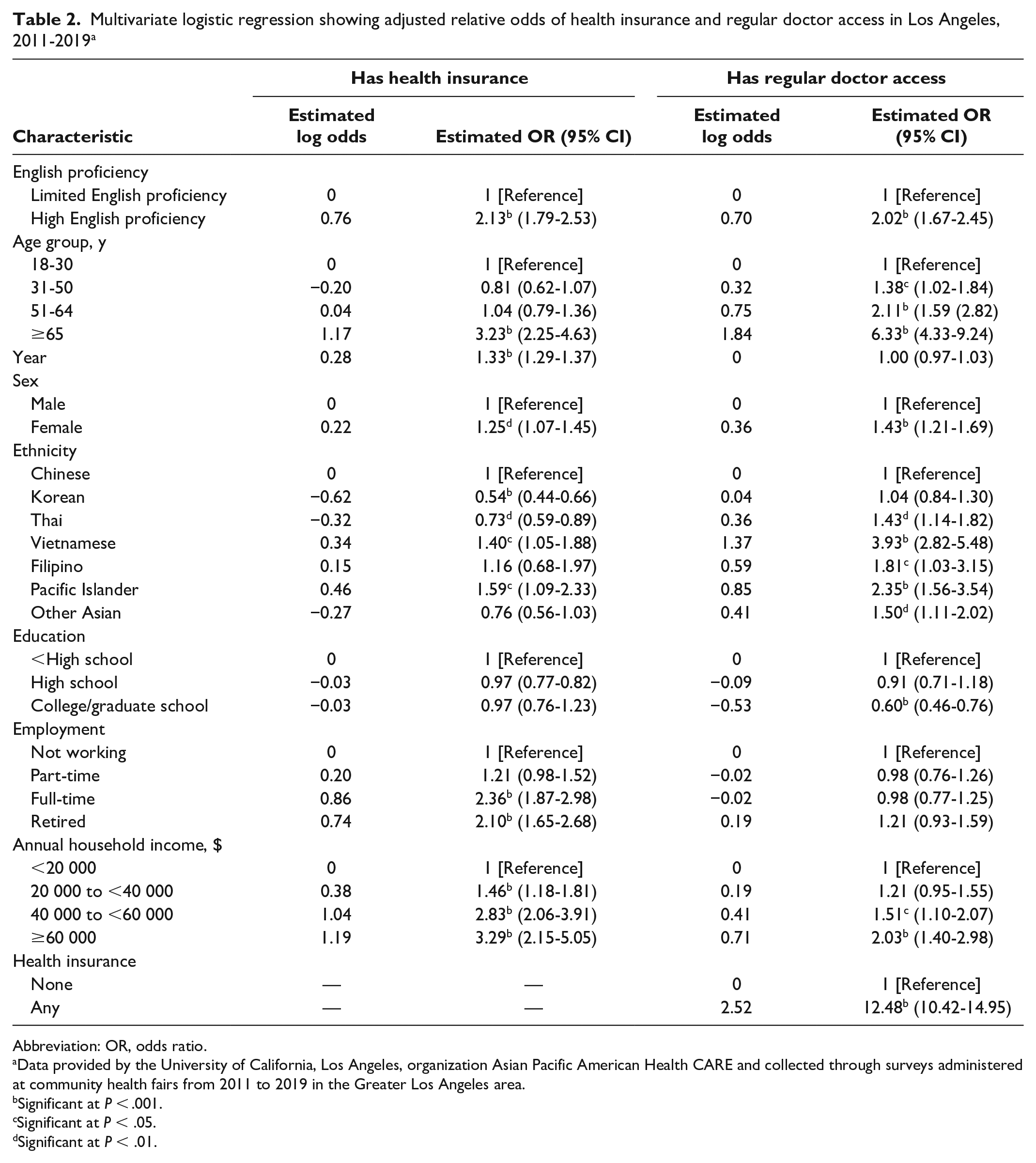
Abbreviation: OR, odds ratio.
Data provided by the University of California, Los Angeles, organization Asian Pacific American Health CARE and collected through surveys administered at community health fairs from 2011 to 2019 in the Greater Los Angeles area.
Significant at P < .001.
Significant at P < .05.
Significant at P < .01.
We observed a significant increase during the study period for health insurance rates (odds ratio [OR] = 1.33; 95% CI, 1.29-1.37) but not for regular doctor access (OR = 1.00; 95% CI, 0.97-1.03) (Table 2).
Health Insurance Status and Doctor Access
We found a positive interaction (adjusted OR [aOR] interaction coefficient = 1.08; P = .01) between English proficiency and year in the health insurance model (Figure 2, Supplemental Table). Throughout the study period, the adjusted odds of participants with LEP being insured increased by a factor of 1.31 (P < .001) per year compared with 1.41 for participants with HEP (P < .001). The disparity in health insurance access between participants with HEP and participants with LEP widened by a factor of 1.08 annually.
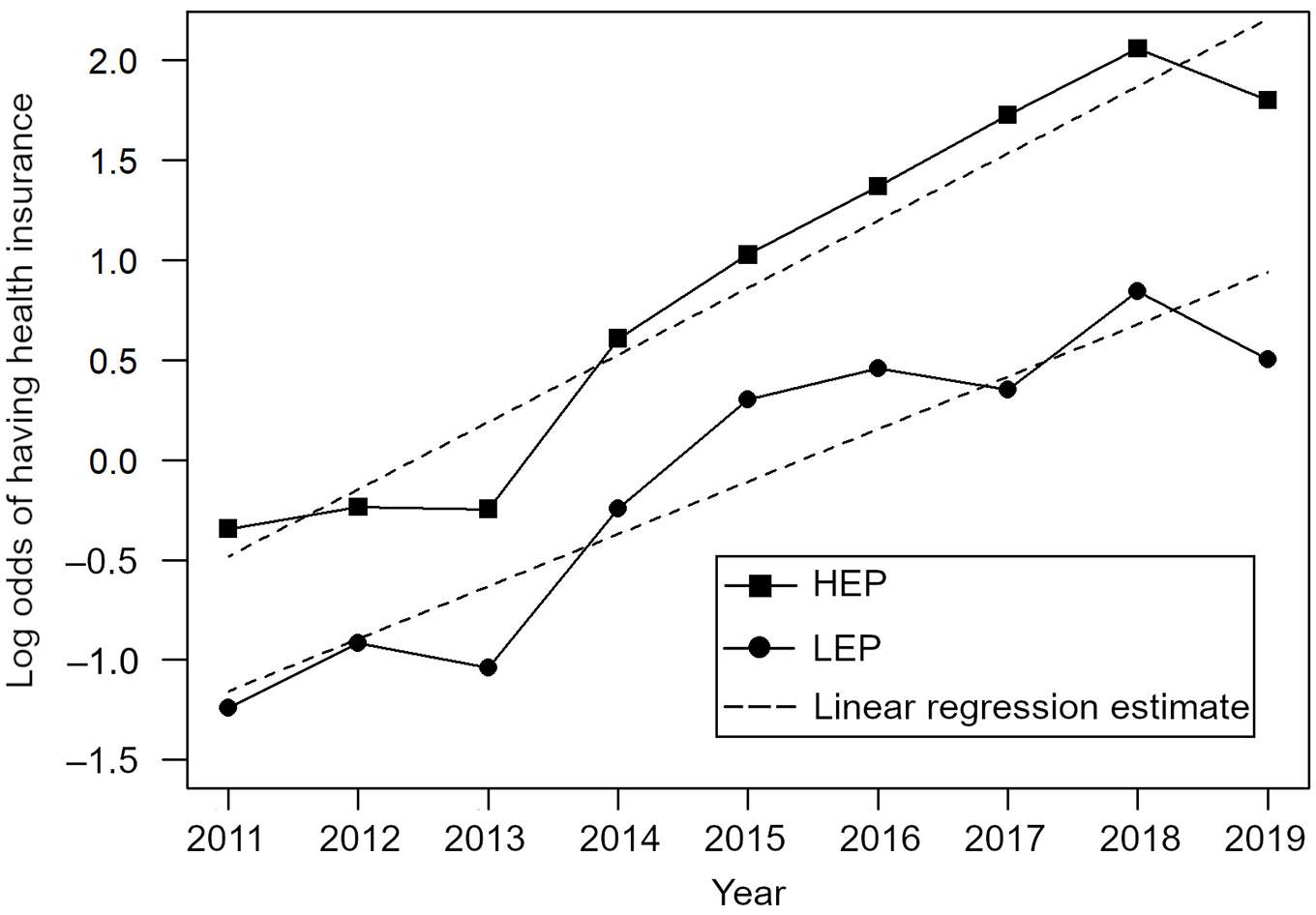
Log odds of having health insurance coverage among Asian and Pacific Islander American health fair attendees in Los Angeles, 2011-2019. For each year, the adjusted odds of participants with low English proficiency (LEP) having health insurance coverage increased by a factor of 1.308 (log odds = 0.269, P < .001). In comparison, the adjusted odds of participants with high English proficiency (HEP) having health insurance increased by a factor of 1.408 each year (log odds = 0.343, P < .001). Using a logistic regression, we found a significant positive interaction effect between English proficiency level and year (estimated interaction coefficient = 0.0745, P = .01), indicating that the adjusted odds ratio (HEP/LEP) widened by a factor of 1.08 each year.
In contrast, we found no significant interaction between English proficiency and year in the doctor access model (aOR interaction coefficient = 0.99; P = .58) (Figure 3, Supplemental Table). The disparity in doctor access between participants with HEP and participants with LEP was stable.
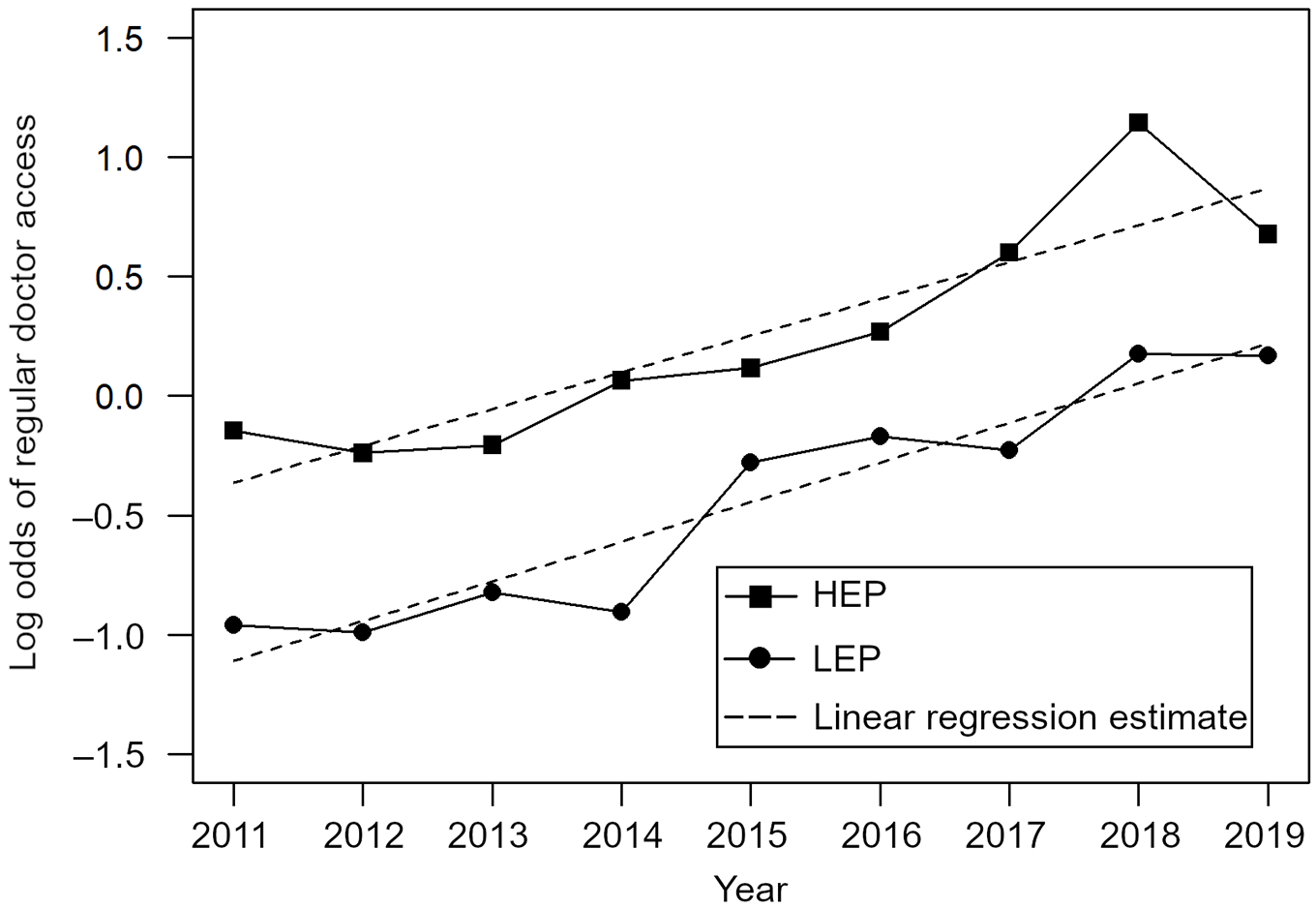
Log odds of having regular doctor access among Asian and Pacific Islander American health fair attendees in Los Angeles, 2011-2019. Using logistic regression, we found no significant interaction between English proficiency level and year (estimated interaction coefficient = −0.0144, adjusted odds ratio = 0.99, P = .58). For both groups of participants (low levels and high levels of English proficiency), the adjusted odds of regular doctor access increased by a factor of 1.166 each year (log odds = 0.153, P < .001).
Discussion
During the 9-year study period, health insurance status among APIA health fair attendees increased and doctor access rates stayed the same. However, participants with LEP were less likely than participants with HEP to have health care access during the study period, which was counter to our a priori hypothesis. In fact, the disparities in health insurance rates widened. Participants who were male, were younger, had LEP, and had a low income were less likely to have health insurance and a regular doctor than their female, older, HEP, and high-income counterparts. Compared with Chinese participants, Thai and Korean participants were significantly less likely to have health insurance, but Thai, Vietnamese, Filipino, and Pacific Islander participants were significantly more likely to have a regular doctor. These findings are invaluable in identifying APIA people with low health care use to inform and target local policy decisions to reduce disparities.
Socioeconomic Status and Health Care Access
Our findings demonstrate that young men with low income are less likely to have health insurance and a regular doctor compared with older women with high income, which is in concordance with previous literature.11-13,19 In addition, Chinese people have been shown to be more likely to have health insurance and a regular doctor than other APIA groups. 15 However, a 2019 study showed that Chinese people may not have greater access to a doctor despite being more likely than their APIA counterparts to have health insurance. 20 Although our findings confirm that Chinese people are more likely to have health insurance than Korean and Thai people, it also does not show they are more likely to have access to a regular doctor when controlling for health insurance. These findings suggest that improved numbers on health care access for Chinese people may be the result of increases in rates of having health insurance that do not translate to increased access to health care services. In fact, once the health insurance advantage is taken away, Chinese participants in our study were less likely to have a regular doctor than their counterparts. It may be beneficial, then, to target some APIA groups, such as Thai and Korean people, for health insurance enrollment efforts, while also connecting Chinese people to a regular source of care. Further efforts to investigate these interethnic disparities via disaggregation of data among APIA groups may help inform ethnic-specific policy interventions to improve health care access.
Language Disparities in Health Insurance Status
We found an increase in health insurance status during the study period for participants with LEP and participants with HEP. Part of this increase could be related to the Affordable Care Act, which other studies have demonstrated to be successful in increasing health insurance status for the APIA population.21-23 We found a small, nonsignificant decrease in health insurance status for both APIA participants with LEP and APIA participants with HEP in our sample from 2018 to 2019. This decrease coincided with the elimination of the individual mandate through the Tax Cuts and Jobs Act, 24 which was projected to reduce health insurance coverage, although no direct policy analysis was performed in our work to confirm this speculation. 25
Despite these trends, disparities in health insurance status between APIA people with LEP and APIA people with HEP not only persisted but widened during the study period, suggesting that participants who spoke English well benefited more from policies that increased health insurance access than participants who did not speak English well. A study conducted on non–APIA people based on the Medi-Cal Expenditure Panel Survey found that disparities in health insurance status because of language proficiency narrowed in the years after passage of the Affordable Care Act. 10 Another study found an uptake in Medicaid insurance among Spanish-speaking and non–Spanish-speaking LEP patients in California after the implementation of language access policies. 9 Our findings suggest that the narrowing of language disparities during the study period did not hold for the disadvantaged APIA participants at our health fairs.
Language Disparities in Regular Doctor Access
The broader literature has consistently identified disparities in doctor access between APIA people with HEP and APIA people with LEP. Kim and Keefe 26 found poorer self-rated health, higher psychological distress, and lower health care service use among APIA people with LEP compared with APIA people with HEP. Cook et al 8 demonstrated difficulty in accessing care for APIA people with LEP after Medicaid expansion, even after enrolling in health insurance. Our study adds to these findings using repeated cross sections from a multiyear large-scale database, demonstrating that the disparities between health fair participants with HEP and health participants with LEP in doctor access persisted throughout most of our study period, as well as in our pooled regression model, even after controlling for health insurance status. This finding suggests that insuring APIA people with LEP is not sufficient to significantly decrease the gap in health care access resulting from a lack of English proficiency. Instead, a comprehensive policy approach that provides more robust language-appropriate and culturally competent services is necessary to fully close the observed gap in health care access.
Section 1557 of the Affordable Care Act attempted to address language disparities by requiring federally funded organizations to provide medical interpreters and notices of the availability of these interpreters for people with LEP. 27 At the state level, the 2017 California Senate Bill No. 223 attempted to improve access to language services for people with LEP by requiring Medi-Cal–funded organizations to provide medically qualified interpreters and notify patients of the availability of these language services, annually, through notices and regular communication. 28 However, in our sample, health care access disparities resulting from language barriers persisted from 2011 to 2019. Although this finding cannot be directly ascribed to any particular policy, it suggests that more needs to be done to fully address the impact of language disparities among our APIA health fair participants.
Narrowing the Gap in Health Care Access Between APIA People With HEP and LEP
Persistent disparities in health care access between APIA people with LEP and APIA people with HEP are often driven by informational barriers, such as inadequate translated materials and culturally competent personnel to provide guidance on health insurance enrollment and referral to appropriate clinics.8,29,30 One model that could increase health insurance enrollment for health fair participants would be to incorporate culturally competent employees in health insurance agencies that serve APIA-dense communities. Such a program has been implemented on a small scale in Illinois, making use of culturally competent health care navigators who guide Asian participants with LEP through the enrollment process, and was successful in increasing the number of insured Asian people with LEP. 31 Organizing health fairs at APIA cultural festivals in which culturally competent navigators help connect APIA people with LEP to clinics with language services may also be beneficial. Health fairs conducted by the UCLA student group APA Health CARE using this model have shown promise in increasing health insurance coverage and doctor access for people with LEP. 16 Local and state policy makers may consider increasing funding streams to support culturally competent community outreach activities to narrow the gap in health care access resulting from a lack of English proficiency in the APIA population.
Limitations
This study had several limitations. First, our data were self-reported; thus, recall bias may have affected responses. To address this bias, we included a “don’t remember” response option in our surveys to minimize the likelihood of participants providing incorrect information. Second, the surveys relied on participants’ ability to self-assess English proficiency, with no clear guidelines on the definition of proficiency levels. To reduce this variability in definition, we stratified the 4 response types into 2 broad groups: participants with HEP and participants with LEP.
Third, study participants differed from year to year; thus, annual demographic shifts could have affected rates of having health insurance or a regular doctor. We addressed this limitation by performing logistic regressions controlling for all demographic variables each year.
Finally, sampling bias is an area of concern because surveys were administered at free health screenings. Our sample was 50.4% Chinese, a group that tends to fare better than other APIA subgroups on many socioeconomic indicators.32,33 We addressed this potential for bias by controlling for socioeconomic factors, such as income, to ensure that these factors did not confound our results. Although the sampling bias decreased the generalizability of our findings to the APIA population, our study has value because it analyzed repeated cross sections during the study period of a subset of APIA people with LEP who may traditionally be left out of longitudinal studies. Future longitudinal studies using cohorts that more broadly represent the APIA population would be strong additions to research in health care disparities and health policy.
Conclusions
From 2011 to 2019, although rates of health insurance status increased, doctor access rates remained relatively low and did not improve among our sample of APIA health fair participants. Furthermore, disparities in health care access resulting from differences in English proficiency persisted; participants with LEP were consistently less likely to have health insurance and a regular doctor than participants with HEP, even when controlling for socioeconomic covariates. We also found significant differences in health care access by age, sex, income, and ethnicity. Although such disparities should have declined because of various policies implemented nationally and in California, our findings showed that omnibus policies to improve health care access, mainly focused on increasing access to health insurance, did not eliminate disparities in health care access because of language barriers. Systemic efforts advocating for culturally competent and language-concordant interventions that connect groups at risk of inadequate health care access to appropriate resources may improve health care disparities highlighted in our study.
Supplemental Material
sj-docx-1-phr-10.1177_00333549211061328 – Supplemental material for Trends in Health Care Access Disparities Among Asian and Pacific Islander Health Fair Participants in Los Angeles, 2011-2019
Supplemental material, sj-docx-1-phr-10.1177_00333549211061328 for Trends in Health Care Access Disparities Among Asian and Pacific Islander Health Fair Participants in Los Angeles, 2011-2019 by Suraj Avinash Dhanjani, Hong-Ho Yang, Shuchi Goyal, Kevin Zhang, Gilbert Gee and Burton Cowgill in Public Health Reports
Footnotes
Acknowledgements
The authors thank Asian Pacific American Health CARE, the University of California, Los Angeles (UCLA) David Geffen School of Medicine, and UCLA School of Nursing for the health fairs they organize in the community to help connect the Asian and Pacific Islander American population to long-term care and for providing us with the data to conduct this study. Finally, we thank Yidan Sun for providing statistical advice on research methods and analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.