
Abstract
For more than 30 years, the network of Centers for Disease Control and Prevention (CDC)–funded Prevention Research Centers (PRCs) has worked with local communities and partners to implement and evaluate public health interventions and policies for the prevention of disease and promotion of health. The COVID-19 pandemic tested the PRC network’s ability to rapidly respond to multiple, simultaneous public health crises. On April 28, 2020, to assess the network’s engagement with activities undertaken in response to the early phase of the pandemic, PRC network leadership distributed an online survey to the directors of 34 currently or formerly funded PRCs, asking them to report their PRCs’ engagement with predetermined activities across 9 topical areas and provide case studies exemplifying that engagement. We received responses from 24 PRCs, all of which reported engagement with at least 1 of the 9 topical areas (mean, 5). The topical areas with which the greatest number of PRCs reported engagement were support of frontline agencies (21 of 24, 88%) and support of activities related to health care (21 of 24, 88%). The mean number of activities with which PRCs reported engagement was 11. The PRCs provided more than 90 case studies exemplifying their work. The results of the survey indicated that the PRCs mobilized their personnel and resources to support the COVID-19 response in less than 6 weeks. We posit that the speed of this response was due, in part, to the broad and diverse expertise of PRC personnel and long-standing partnerships between PRCs and the communities in which they work.
The COVID-19 pandemic has underscored the critical role of strong public health infrastructure, multisector collaboration, and community engagement in mobilizing national and local responses to a public health emergency. The national network of Prevention Research Centers (PRCs), composed of researchers and staff members at academic institutions and the Centers for Disease Control and Prevention (CDC) and funded by CDC for more than 30 years, implements and evaluates public health interventions, programs, and policies for the prevention of disease, promotion of health, and mitigation of health care expenditures, particularly in communities with a disproportionate burden of disease.1-4 The scope of the network’s activities was previously highlighted in a special issue of the American Journal of Preventive Medicine, celebrating the 30th anniversary of the PRC program. 5
Long-standing relationships between PRCs and the communities they serve foster trust among PRC researchers, community members and leaders, and organizations. 6 As a result, PRCs are positioned to quickly and effectively respond to urgent health needs, coordinating the provision of health and social services and collecting data to inform efforts in health promotion and disease prevention.7-10 By understanding community priorities and assets before a crisis and leveraging community partnerships, PRCs can mobilize resources to understand the challenges and quickly collaborate with local communities to facilitate a response.
In the wake of the COVID-19 pandemic, the need for a rapid response to social and health concerns was more urgent than ever, presenting an opportunity for the PRC network to address the myriad public health emergencies that the pandemic exacerbated or created. This unprecedented moment tested the PRC network’s ability to rapidly identify research needs, exchange information among its members, and disseminate evidence-based interventions in collaboration with community partners.
Purpose
The purpose of this study was to (1) assess the breadth of the PRC network’s response to the early phase (March–May 2020) of the COVID-19 pandemic and (2) identify case studies exemplifying the network’s engagement with activities undertaken in response to the pandemic.
Methods
Study Design and Sample
On April 28, 2020, when the number of confirmed COVID-19 cases in the United States surpassed 1 million, 11 the PRC executive committee, composed of academic leaders in the network, distributed an online survey via email to the directors of the 34 PRCs funded during the current (2019-2024) or previous (2014-2019) funding cycles. We asked representatives from each PRC to assess and provide examples of their PRCs’ engagement with activities undertaken in response to the COVID-19 pandemic, encouraging them to seek input from other staff members and researchers at their centers to elicit a comprehensive report. We sent reminder emails on May 6 and 14. The survey closed on May 19. We created the survey in Qualtrics (Qualtrics). This study was determined non–human subjects research by the Committee for the Protection of Human Subjects in Research at the University of Massachusetts Medical School.
Engagement With COVID-19 Response Activities
We asked respondents to assess the degree to which their PRC engaged with each of 36 distinct activities related to the COVID-19 response. The study leaders and PRC executive committee selected these activities based on their knowledge of the network’s scope of work, with the objective of capturing all activities with which any PRC might have engaged.
The study leaders and executive committee identified 9 topical areas into which the activities were categorized: (1) support of frontline agencies, (2) food provision, (3) agriculture, (4) health care, (5) employment, (6) mental health, (7) education, (8) community health workers, and (9) support of community partners. The number of activities included in each topical area ranged from 2 (agriculture and mental health) to 8 (food provision). For each activity, we asked respondents to report the degree to which their PRCs engaged with the activity on a scale of 1 to 4, where 1 = none, 2 = limited, 3 = moderate, and 4 = substantial engagement. We coded missing values as none after observing that many respondents left blank the questions related to topical areas in which their PRCs were not working. In addition to reporting engagement with the predetermined activities, respondents could report their PRC’s engagement with up to 3 other activities in each topical area. However, we excluded these activities from later analysis because of heterogeneity in responses across the PRCs.
Case Studies and Network Research Collaboration
For each topical area, we asked respondents to provide a brief case study of their PRCs’ engagement in the topical area. For inclusion in this article, the study leaders and executive committee selected 5 case studies that reflected the breadth of the network’s response, and we identified and reported common themes across the 5 case studies.
Finally, we asked each respondent to report on any COVID-19–related research activity within the PRC network’s actively funded thematic research networks: Cancer Prevention and Control Research Network, Managing Epilepsy Well Network, Nutrition and Obesity Policy Research and Evaluation Network, and Physical Activity Policy Research and Evaluation Network. 12 The PRCs in each thematic network interact regularly to discuss ongoing research, collaborate on research projects, and disseminate findings.13-16
Statistical Analysis
We recoded the PRCs’ self-reported engagement with each activity in a topical area as none (1) or any engagement, where any engagement was defined as limited (2), moderate (3), or substantial (4) engagement. We similarly recoded engagement in each of the 9 topical areas (none vs any), with each PRC reporting limited, moderate, or substantial engagement with any activity in a given topical area considered to have engaged in that topical area. We counted the number of PRCs that reported any engagement with each of the predetermined activities and the number of PRCs that reported any engagement in each topical area.
For each activity, among the PRCs that reported any engagement, we also calculated the number and proportion of PRCs that reported limited, moderate, and substantial engagement, respectively. We made calculations in Microsoft Excel 2019 (Microsoft Corporation).
Outcomes
Engagement With COVID-19 Response Activities
Of the 34 PRCs that received the survey, 24 (71%) responded, including 21 currently funded PRCs. All 24 PRCs reported engagement in at least 1 of the 9 topical areas, and the mean number of topical areas in which a PRC reported engagement was 5.
The topical areas in which the greatest number of PRCs reported any engagement were support of frontline agencies (21 of 24, 88%) and health care (21 of 24, 88%). The topical areas in which the fewest number of PRCs reported any engagement were agriculture (5 of 24, 21%) and employment (6 of 24, 25%) (Figure).
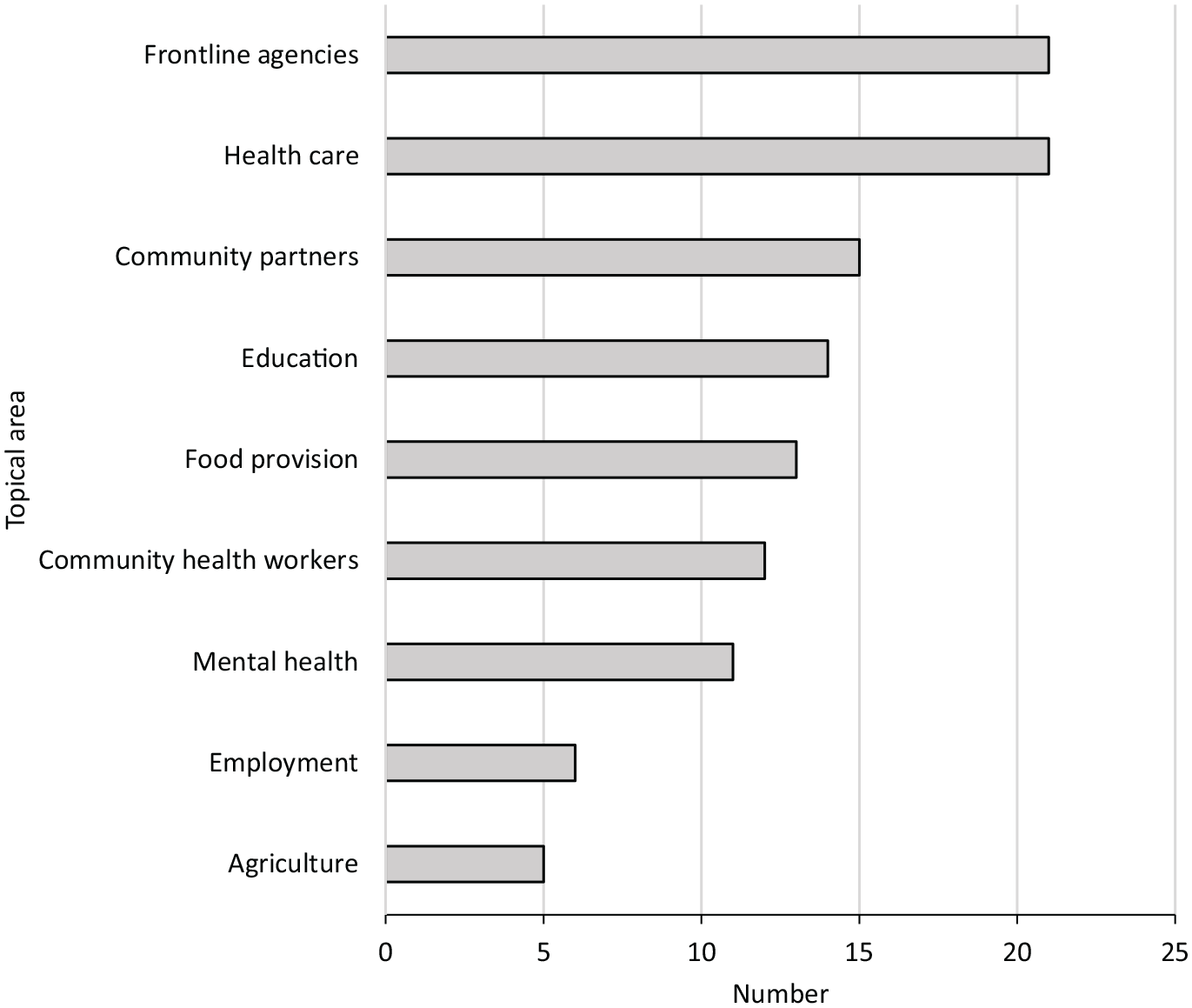
Number of Prevention Research Centers (PRCs) that reported any engagement with COVID-19 response activities, by topical area (n = 24), United States national PRC network, March–May 2020. Data were from responses to an online survey distributed to the directors of the 34 PRCs funded during the current (2019-2024) or former (2014-2019) funding cycles. Responses were collected from April 28 to May 19, 2020, and reflected the engagement of PRCs with COVID-19 response activities during the period of early March through mid-May 2020. Twenty-four PRCs responded to the survey, including 21 currently funded PRCs. The PRC network comprises researchers and staff members at academic institutions and the Centers for Disease Control and Prevention. The purpose of the PRC program is to implement and evaluate public health interventions, programs, and policies for the prevention of disease, promotion of health, and mitigation of health care expenditures.1-4
The mean number of activities with which each PRC reported any engagement was 11. The mean number of activities with which each PRC reported limited, moderate, and substantial engagement was 4, 3, and 4, respectively. For each activity, at least 2 PRCs reported any engagement. The activities with which the greatest number of PRCs reported any engagement were support of social service organizations (18 of 24, 75%), support of local health departments (16 of 24, 67%), support of health care organizations (16 of 24, 67%), and improving risk communication (16 of 24, 67%). The activities with which the fewest number of PRCs reported any engagement were providing meals to health care workers (2 of 24, 8%) and reducing food waste (2 of 24, 8%) (Table 1).
Engagement with activities related to the COVID-19 response among 24 Prevention Research Centers (PRCs), overall and according to degree of engagement, United States national PRC network, March–May 2020 a
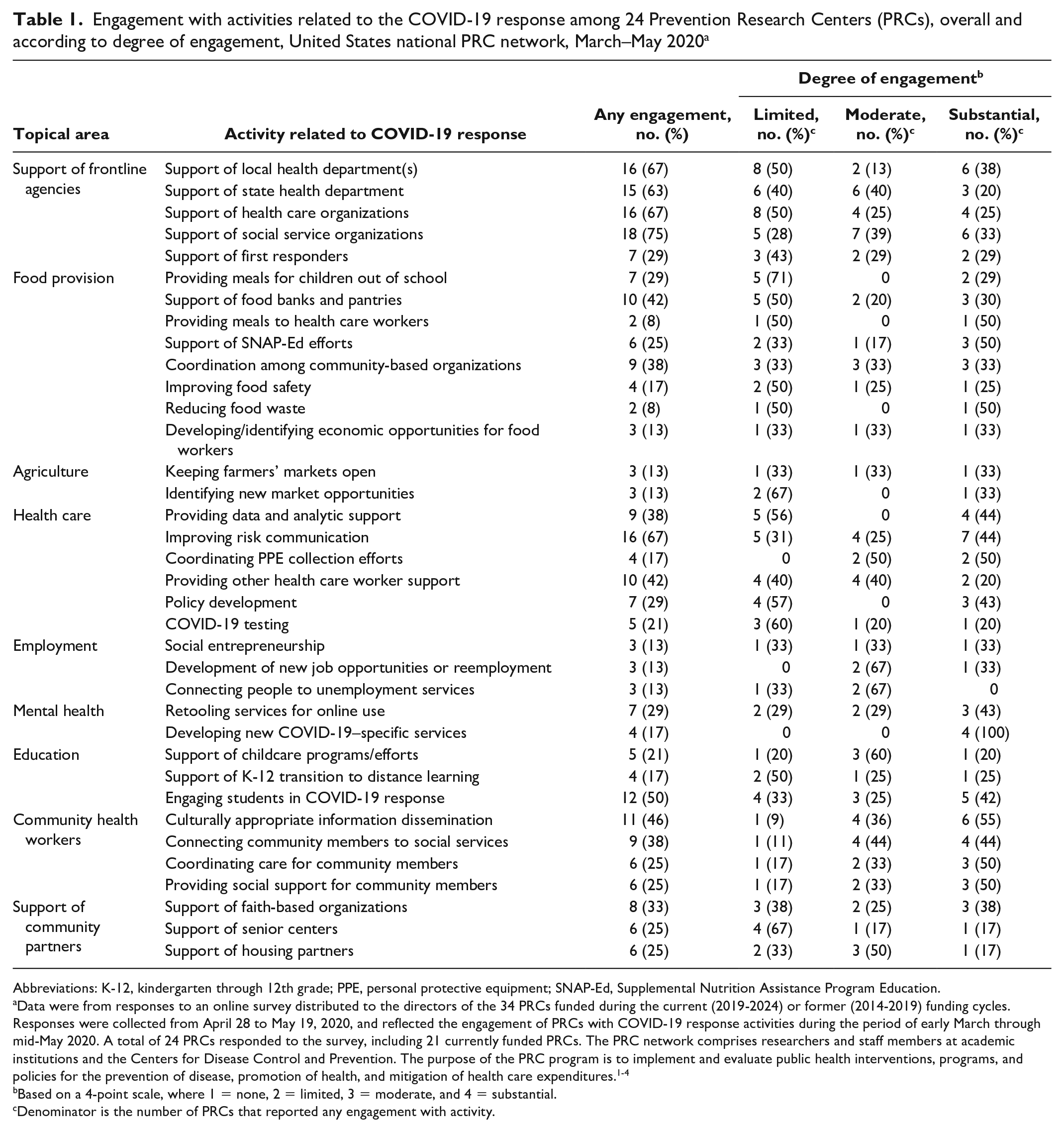
Abbreviations: K-12, kindergarten through 12th grade; PPE, personal protective equipment; SNAP-Ed, Supplemental Nutrition Assistance Program Education.
Data were from responses to an online survey distributed to the directors of the 34 PRCs funded during the current (2019-2024) or former (2014-2019) funding cycles. Responses were collected from April 28 to May 19, 2020, and reflected the engagement of PRCs with COVID-19 response activities during the period of early March through mid-May 2020. A total of 24 PRCs responded to the survey, including 21 currently funded PRCs. The PRC network comprises researchers and staff members at academic institutions and the Centers for Disease Control and Prevention. The purpose of the PRC program is to implement and evaluate public health interventions, programs, and policies for the prevention of disease, promotion of health, and mitigation of health care expenditures.1-4
Based on a 4-point scale, where 1 = none, 2 = limited, 3 = moderate, and 4 = substantial.
Denominator is the number of PRCs that reported any engagement with activity.
Case Studies
The 24 PRCs reported more than 90 case studies, with at least 4 reported in each topical area. Common themes among the 5 selected case studies included long-standing partnerships, deployment of trusted community leader/spokesperson, multisector partnerships, and broad expertise and centralization of expertise in a university setting (Table 2).
Common themes identified in COVID-19 response case studies reported by 24 Prevention Research Centers (PRCs), United States national PRC network, March–May 2020 a
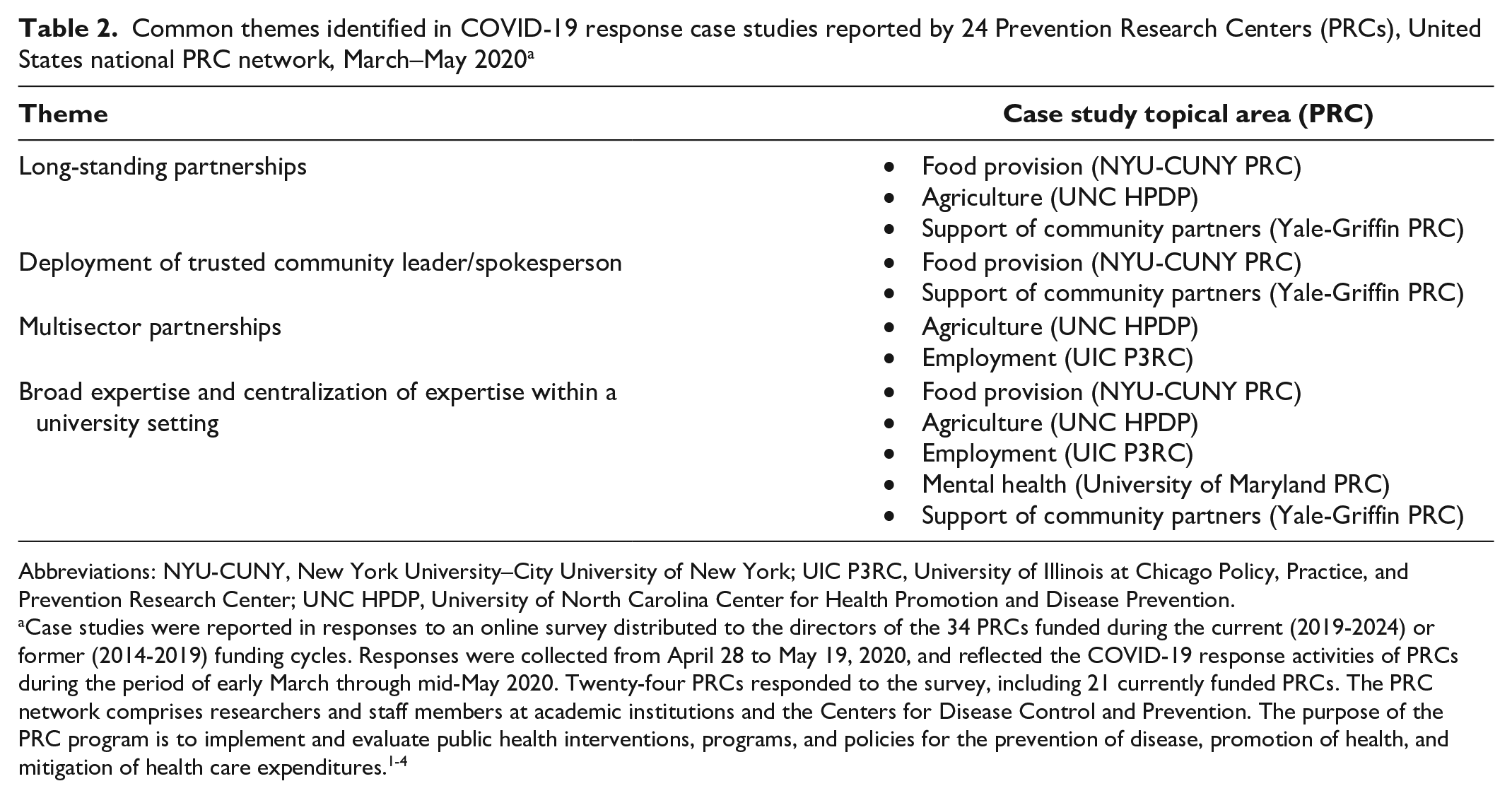
Abbreviations: NYU-CUNY, New York University–City University of New York; UIC P3RC, University of Illinois at Chicago Policy, Practice, and Prevention Research Center; UNC HPDP, University of North Carolina Center for Health Promotion and Disease Prevention.
Case studies were reported in responses to an online survey distributed to the directors of the 34 PRCs funded during the current (2019-2024) or former (2014-2019) funding cycles. Responses were collected from April 28 to May 19, 2020, and reflected the COVID-19 response activities of PRCs during the period of early March through mid-May 2020. Twenty-four PRCs responded to the survey, including 21 currently funded PRCs. The PRC network comprises researchers and staff members at academic institutions and the Centers for Disease Control and Prevention. The purpose of the PRC program is to implement and evaluate public health interventions, programs, and policies for the prevention of disease, promotion of health, and mitigation of health care expenditures.1-4
Food Provision
Through an existing community health worker program, researchers at New York University–City University of New York PRC conducted a survey to assess the impact of COVID-19 on immigrant families in New York City, identifying food insecurity and unemployment as the most pressing concerns. To address these concerns, the PRC’s cohort of community health workers, working with faith-based organizations, connected community members with food-delivery and food-bank services.
Agriculture
Working with community-based organizations in Chatham County, North Carolina, researchers affiliated with the University of North Carolina Center for Health Promotion and Disease Prevention and University of North Carolina Health designed a drive-through food hub in a rural town to coordinate the sale or donation of food by local restaurants, farmers, charitable food programs, and small-scale artisans. This community experienced unique challenges during the COVID-19 pandemic because of widespread transmission at a poultry-processing plant that employed a large proportion of the community’s Latino population. The objectives of the food hub were to increase access to healthy, affordable food for low-income and food-insecure residents and to generate revenue for vendors whose sales declined during the COVID-19 pandemic.
Employment
To address a lack of comprehensive guidance for Illinois workers during the COVID-19 pandemic, the University of Illinois at Chicago Policy, Practice, and Prevention Research Center partnered with the University of Illinois at Chicago Center for Healthy Work and the Great Lakes Center for Occupational Health and Safety to create a comprehensive COVID-19 Guide for Workers in Illinois, 17 which included information on federal and state protections and benefits for workers, as well as resources tangentially related to work, such as housing and food security. The guide also provided resources for specific communities, such as undocumented workers, sex workers, and caretakers.
Mental Health
Following the abrupt transition of mental health services to virtual formats during the COVID-19 pandemic, researchers at the University of Maryland PRC identified that mental health organizations and providers were overwhelmed. To assess the influence of this transition on therapists’ mental health and practices, the PRC created and distributed an online survey to mental health providers, assessing 3 main areas: the mental well-being of mental health providers themselves, changes to the practices of providers, and changes in the composition of providers’ clients. In their responses to the survey, mental health providers reported that their own mental well-being had suffered as a result of the COVID-19 pandemic. The PRC researchers who conducted the survey reported their findings in a 2021 commentary published in Public Health Reports. 18
Support of Community Partners
Early in the COVID-19 outbreak, the Yale-Griffin PRC leveraged its partnerships with 5 food pantries serving towns in the Lower Naugatuck Valley of Connecticut and several nonprofit organizations to provide food to community members. The Yale-Griffin PRC temporarily assumed responsibility for the coordination of a church-based pantry unable to continue operations as a result of the COVID-19 pandemic. In addition, to address increased food insecurity in New Haven, Connecticut, the PRC coordinated the work of more than 40 food pantries in the city.
Network Research Collaboration
The PRCs reported ongoing research collaborations in 2 thematic networks. Early in the pandemic, in collaboration with Healthy Eating Research (HER), members of the Nutrition and Obesity Policy Research and Evaluation Network established the HER Nutrition and Obesity Policy Research and Evaluation Network COVID-19 School Nutrition Implications Working Group. Composed of >380 researchers, advocacy organization representatives, and practitioners and >185 students, this group examined impacts of the COVID-19 pandemic on food security and dietary intake. Members of this group published an article, “Feeding Low-Income Children During the COVID-19 Pandemic,” in the March 2020 issue of the New England Journal of Medicine. 19 Shortly after the onset of the COVID-19 pandemic, in response to reports of delays in cancer therapy resulting from closed clinics and patients’ concerns about COVID-19 exposure, members of the Cancer Prevention and Control Research Network developed a framework for cancer survivorship care during COVID-19. 20
Lessons Learned
The results of this survey provide evidence of a rapid, multifaceted response to the COVID-19 pandemic across the PRC network. All 24 PRCs that participated reported engagement with at least 1 activity related to the COVID-19 response; on average, each PRC reported engagement with nearly a dozen activities.
The survey was intended to capture the COVID-19 response activities of the PRC network in the period after the pandemic had begun to spread widely in the United States, and the resulting economic and social consequences had become manifest. On March 13, 2020, the federal government declared a state of emergency and, on March 19, 2020, California issued the first statewide stay-at-home order, 21 the same date on which the number of confirmed cases of COVID-19 in the United States surpassed 10 000. 11 Considering the timing of these events, which may indicate the onset of a period of more widespread transmission, the results of the survey suggest that many of the PRCs mobilized their personnel and resources to support the COVID-19 response in a period of less than 6 weeks. Historically, such a short period between the onset of a crisis and the response of researchers has been uncommon among health and biomedical research institutions, which have a reputation of long delays between research discovery and the translation of that research into practice. 22
We posit that the speed of the network’s response to the pandemic was made possible, in part, through long-standing relationships and trust between PRCs and their community partners, 6 which include schools, local and state health departments, religious institutions, and social service organizations, among others.7,8,23 Equally important was the broad expertise of PRC researchers and staff members. This expertise, which includes data analysis and program evaluation, intervention development and adaptation, and synthesis and dissemination of public health research, is invaluable to the community partnerships that PRCs maintain.
This nimble response to health crises differentiates PRCs from other academic units within large research universities, where research priorities are more often driven by available funding than by community collaboration, and the application and review process may exceed a year. 24 These factors may limit researchers’ meaningful engagement with community members and organizations and inhibit their response to emerging community health concerns. Although PRCs are subject to similar constraints, long-term community partnerships make navigating them more feasible.
Through this work, we learned 3 important lessons. First, the identification of case studies served as an inventory of the expertise that exists among the network’s researchers and practitioners. As a result of this work, members of the network will be able to quickly identify those to whom they might go for help in addressing specific community health concerns. Second, the survey highlighted many of the shared priorities of PRCs, and it generated suggestions for novel research that might be addressed collaboratively, using the full extent of the network’s resources. A recent analysis of co-authorship among PRC-affiliated researchers found “room for improvement” despite intranetwork collaboration. 25 We hope that our approach to assessing the COVID-19 response will be a mechanism that the PRC network can use to stimulate future collaboration. Third, the survey responses demonstrated that the work of PRCs goes far beyond conducting federally funded research. PRCs serve critical roles in their communities, strengthening local and national public health infrastructure, 9 which, as was demonstrated in response to the pandemic, can be quickly leveraged in the event of a public health emergency to deliver support and relief to communities.
Conclusions
In its response to the COVID-19 pandemic, the PRC network demonstrated its unique ability to leverage long-standing partnerships and to mobilize its resources to support vulnerable communities and to conduct critical public health research. After more than 30 years since its founding, the PRC network continues to fulfill its mission of developing and rigorously evaluating programs and policies to prevent disease and promote health. The history of collaboration with community partners, in combination with strong research expertise, positions PRCs to respond rapidly to emerging public health crises such as the COVID-19 pandemic.
Footnotes
Acknowledgements
The authors thank the members of the executive committee of the PRC network for their insights during the development of the survey; all staff members and researchers who contributed to their PRCs’ survey responses; and the community leaders and organizations that partner with PRCs to address the many serious health challenges facing our communities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.R.B. was supported by a National Heart, Lung, and Blood Institute National Research Service Award predoctoral traineeship (grant #T32HL129969).