
Abstract
The COVID-19 pandemic created unprecedented strain on the personal protective equipment (PPE) supply chain. Given the dearth of PPE and consequences for transmission, GetMePPE Chicago (GMPC) developed a PPE allocation framework and system, distributing 886 900 units to 274 institutions from March 2020 to July 2021 to address PPE needs. As the pandemic evolved, GMPC made difficult decisions about (1) building reserve inventory (to balance present and future, potentially higher clinical acuity, needs), (2) donating to other states/out-of-state organizations, and (3) receiving donations from other states. In this case study, we detail both GMPC’s experience in making these decisions and the ethical frameworks that guided these decisions. We also reflect on lessons learned and suggest which values may have been in conflict (eg, maximizing benefits vs duty to mission, defined in the context of PPE allocation) in each circumstance, which values were prioritized, and when that prioritization would change. Such guidance can promote a values-based approach to key issues concerning distribution of PPE and other scarce medical resources in response to the COVID-19 pandemic and related future pandemics.
The first wave of the COVID-19 pandemic led to high demand for, and ensuing scarcity of, personal protective equipment (PPE). 1 The need for specialized PPE (N95, FFP2 respirators) in virus-rich environments such as hospitals was underscored by Cheng and colleagues, 2 who showed infection probability remained close to 1 with use of face masks alone.
The literature describes the ethical allocation of medical resources such as ventilators and vaccines,3,4 as well as overarching principles to consider in general resource allocation during a crisis, such as obligations to community and good preparedness practice. 5 However, discussions on ethical PPE distribution in the literature are limited. This dearth is evidenced in an article by Binkley and Kemp, 6 which focuses narrowly on allocation to health care providers rather than on acquiring and distributing PPE beyond that context.
Cheng and colleagues 2 demonstrated the effectiveness of wearing a face mask to prevent large-droplet transmission, particularly in areas of low virus abundance. In alignment with this goal of reducing transmission, GetMePPE Chicago (GMPC), established by medical students to combat the PPE shortage, disseminated 886 900 units of PPE to 274 institutions from March 2020 to July 2021. 2 We operationalized the ethical principles presented by Emanuel and colleagues, 3 a more adequate framework than that of Binkley and Kemp and others, for PPE distribution. 7 In a volunteer-led effort, GMPC secured PPE donations from local manufacturers and companies and used crowdfunding to purchase PPE.
Purpose
This study aims to recount GMPC’s experience with 3 key issues: (1) building a PPE reserve and (2) donating to and (3) receiving donations from other states. We expand on the aforementioned ethical principles we operationalized (Table) by suggesting which values to consider in approaching the 3 key issues and what factors, if any, would change their prioritization to help guide future PPE allocation. These recommendations, in turn, may inform decisions about managing inventory and sharing other medical resources across state lines.
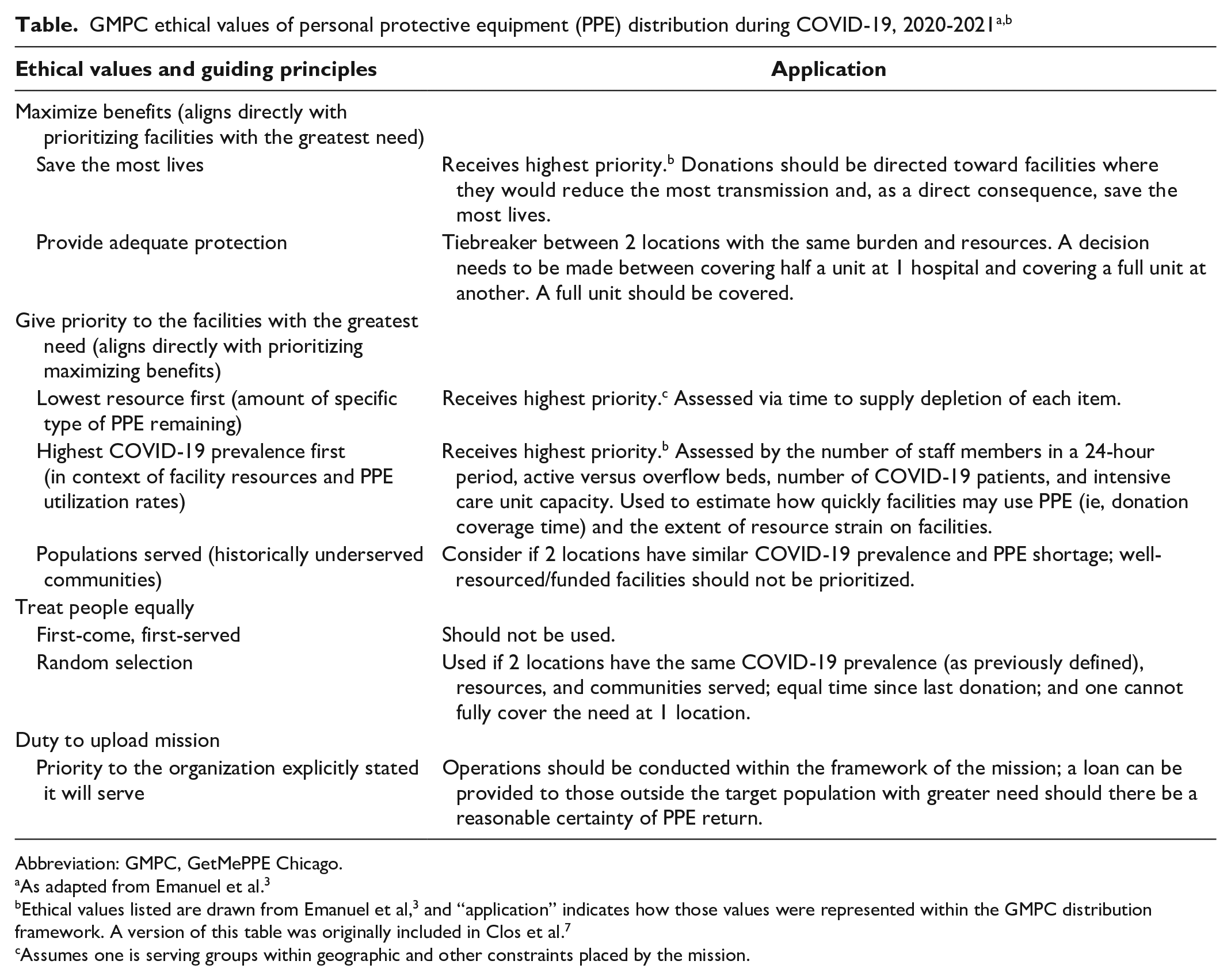
Abbreviation: GMPC, GetMePPE Chicago.
As adapted from Emanuel et al. 3
Ethical values listed are drawn from Emanuel et al, 3 and “application” indicates how those values were represented within the GMPC distribution framework. A version of this table was originally included in Clos et al. 7
Assumes one is serving groups within geographic and other constraints placed by the mission.
Methods
In the first weeks of operation, GMPC consulted bioethicists to create a decision-making aid to guide the distribution of PPE (Table). These experts encouraged us to prospectively quantify institutional PPE need and stratify organizations into tiers based on clinical acuity, which informs the risk of transmission to both patients and health care workers. Beyond clinical acuity, we prioritized serving facilities with the greatest need, namely poorly resourced hospitals and clinics (ie, with limited access to PPE, no or few dedicated COVID-19 units, and fewer clinical staff members than other institutions), which serve many of Chicago’s most vulnerable patient populations, and had a high prevalence of COVID-19.
Outcomes
Building a PPE Reserve
During the first wave of the pandemic in spring 2020, when demand for PPE by hospitals and other institutions with high COVID-19 exposure/transmission rates was high and need was quantitatively assessed daily, GMPC decided against creating a separate PPE reserve. 7 An increase in incoming PPE donations, coupled with stabilization of hospital supply chains, decreased the need for GMPC donations at Tier 1 facilities (ie, hospitals that have emergency departments and intensive care units) toward the start of June 2020. The quantity of PPE required by these facilities in any given donation was much larger than the needs of Tier 2 and Tier 3 facilities (ie, nursing homes, long-term care facilities, community health clinics). This situation, coupled with public health experts predicting a second wave in fall/winter 2020, prompted GMPC to begin reserving inventory. Reserving PPE would allow GMPC to respond to a resurgence of larger Tier 1 PPE needs and be prepared in the event of repeated PPE supply chain disruptions that slowed access to PPE during the first wave of the pandemic.
Donating to Other States
GMPC worked closely with similar organizations in neighboring states throughout the COVID-19 pandemic. These areas had outbreaks during times when Illinois had low case rates. We chose to share inventory and/or provide financial support with groups in neighboring states. In each circumstance, we evaluated the needs of these groups through the lens of our own distribution. For example, we chose to give masks to an organization because it knew of facilities (hospitals in need) that were of higher acuity than where we were distributing (long-term care facilities) at that time. When possible, these donations were returned at a later time as either funds or PPE.
For those groups with financial resources, GMPC orchestrated large-quantity PPE orders by pooling funds among several groups to improve our buying power for acquiring PPE. Finally, GMPC’s ethical distribution strategy was reproduced by many of these groups. In sum, combining funds with out-of-state organizations allowed GMPC to increase purchasing power and decrease per-unit cost, while loaning funds or PPE helped GMPC meet needs at higher-acuity facilities just across the border or beyond.
Receiving Donations From Out of State
Initially, we decided that our volunteers would not request PPE donations from out of state (eg, contacting PPE manufacturers, groups that manufacture PPE) to prevent resources from being funneled from states that may have had greater PPE needs. This decision was admittedly not based on numerical comparison of needs in each state but, rather, on a more general awareness that needs could exist in other parts of the country. Furthermore, it would be most efficient, particularly for newly established organizations, to build local infrastructure and meet local needs first.
We made an exception when the opportunity arose to receive a large donation from outside the state. The donor had more PPE than it could distribute on its own in its state. GMPC distributed 203 200 face shields from this out-of-state supplier. This donation was shared with 9 states throughout the Midwest by GMPC and partner organizations.
We later chose to expand the opportunity to receive donations from out of state using a more quantitative and, thereby, accurate approach, in alignment with our goal. We assessed the COVID-19 case rates of the state the donation was coming from and accepted donations if case rates were lower than those in Illinois.
Lessons Learned
By choosing to build a reserve, GMPC prioritized the future maximization of benefits (ie, reduce transmission, save the most lives) and gave priority to facilities with the highest need rather than to facilities that had less need or risk of viral transmission. GMPC justified this prioritization when (1) Chicagoland hospitals had sufficient PPE and (2) reasonable certainty existed of substantially greater need at Tier 1 facilities in the foreseeable future rather than at present (eg, Illinois Department of Public Health’s prediction of an imminent second wave).
A key barrier to meeting PPE demand for many high-acuity facilities early in the first wave of the pandemic was the time between order and receipt of these items. GMPC was able to fill this gap for many institutions through agile purchasing with crowdsourced funds. To abate such delays during a second wave, GMPC reasoned that preserving some inventory could allow rapid deployment in the event that Tier 1 facilities faced renewed shortages. Therefore, given the challenge and uncertainty of ensuring sufficient PPE needs were met for Tier 1 facilities early in the pandemic, the predictions of subsequent waves of disease spread, and the nonlinear consequences of a pandemic, we justified our transition into reserving inventory for the impending second wave.
As we expanded our efforts to serve a range of health care acuity settings, we carefully considered the balance of maximizing the overall benefit (saving lives) and prioritizing facilities with the greatest need. Because an evaluation of the facility resources and populations served were cornerstones of our effort (Table), we were often able to simultaneously maximize benefit while prioritizing disadvantaged patient populations, independent of which tier of clinical acuity was in most demand for a given stage of the pandemic.
In hindsight, we learned, through our experiences later distributing PPE to facilities with less need than hospitals that had high transmission rates and high prevalence of COVID-19, that partnering with lower-tier facilities (ie, nursing homes, homeless shelters) would likely have been a more effective strategy to pursue earlier in the pandemic. This strategy would ensure supplies were distributed to meet these facilities’ more acute needs to theoretically reduce spread and mitigate the initial spike in cases. This conclusion stems from later observations at a time when GMPC had continuing incoming funds, a PPE surplus wherein we could comfortably provide PPE to meet immediate needs, and Chicago showing a stronger-than-expected adaptation to providing PPE through the second wave. However, this course of action (ie, reserve creation) could only be justified if GMPC had relative certainty that we had the financial capability and partnerships to replicate our success during the first wave and meet the needs of its Tier 1 hospital constituents in the future.
We recommend that organizations faced with similar challenges move to meet immediate needs at facilities with lower rates of disease transmission after a decrease in need at Tier 1 facilities, while reserving a smaller amount of PPE in planning for reversal of pandemic trends, as GMPC did. This reserve should be proportioned such that if subsequent waves occur, an organization should be able to quickly meet the same percentage of original donation capacity to high-acuity facilities (hospitals). The organization can therefore take into account how many PPE donations are typically acquired within a specific period, need during the high-acuity period (eg, second wave), time to that high-acuity period, and present demand, to determine how much inventory to keep in reserve.
Donating to Other States
Donations to other states pit GMPC’s duty to our mission/donors (ie, to use funds toward purchasing and distributing PPE in the Chicagoland region, as well as human resources such as time) against the values of maximizing benefits (ie, saving the most lives, reducing transmission) and giving priority to facilities with the greatest need. Although some donors may have expected their financial support to be restricted to Chicagoland need, it is not unreasonable to assume others, if asked, would trust the organization to use funds to prioritize facilities with the greatest need and maximize benefits independent of geography.
GMPC prioritized maximizing time-sensitive benefits of PPE and prioritizing facilities with the greatest need when:
(1) Needs out of state were quantitatively greater than needs within Chicago, from facilities in a tier above Chicago need. For example, a facility such as a hospital that has greater transmission risk and a higher utilization rate of PPE could be prioritized over a primary care clinic in Chicago where aerosolizing procedures would not be performed.
(2) Our forecast for needs in Chicago Tier 1 facilities could be sufficiently met during the time in which we expected to replace the inventory sent across state lines (through either new purchases or donations).
(3) A reasonable expectation existed that the PPE or monetary loan would be returned.
If these criteria were not fulfilled, duty toward donors and the mission would take precedent.
Taking a similar approach for other readily transportable, scarce medical resources with established tiers (eg, vaccines) may reduce further transmission.
The values prioritized here are maximizing benefits and giving priority to facilities with the greatest need, regardless of state borders and mission. GMPC recommends that similar organizations, with a specific geographic area designated within their mission, operate with an awareness of other states’ needs and avoid diverting resources from areas with greater transmission (and, therefore, greater need for transmission reduction). The most accurate way to do so is to quantify PPE prospectively and compare needs across state lines. Volunteers should therefore be trained to verify degree of transmission in other states as an initial step before outreach to prospective out-of-state donors.
Working across state lines promoted substantial benefits in reducing transmission within, and beyond, the Chicagoland area. Time spent forging partnerships and supporting other regional organizations not only allowed GMPC to pool financial resources, providing a benefit to our community in terms of reduced unit costs, but also provided the opportunity for large-scale PPE distribution. An illustrative example of this benefit occurred early in the pandemic, when we distributed 203 200 face shields to 9 states throughout the Midwest. In addition, as of December 7, 2020, GMPC had donated 34 420 3M VFlex 1804 N95 masks to 18 states, Puerto Rico, and Indigenous Tribes. These masks were then distributed by our partner organizations.
Although GMPC’s goals to maximize overall benefits and prioritize facilities with the greatest need have been implemented smoothly thus far, we have not yet faced a situation where this approach brought tension in choosing one over the other. Our framework led us to focus on donating PPE to facilities that accomplished both ethical objectives, particularly by prioritizing facilities that were poorly resourced, which largely overlapped with facilities serving Chicago’s most vulnerable populations. We recognize that our solution to resolving conflict between these ethical principles may not always exist in other communities or with other public health crises. To alleviate potential conflicts, we recommend fostering strong relationships and communication with other groups with similar missions to coordinate efforts that may be able to address both ethical guidelines. For example, a number of times during the pandemic, we knew of other groups securing PPE that were in some manner affiliated with well-resourced medical institutions in more immediate need of PPE. Through our communication and awareness of the efforts of this and other groups, we were able to continue prioritizing our guiding principles of serving facilities with the greatest need. Other scenarios may require different methods of resolving conflict of these ethical issues.
Footnotes
Acknowledgements
The authors thank Josh Hauser, MD, and Erin Paquette, MD, JD, MBe, for their guidance on how to construct our overall distribution paradigm ethically. We also acknowledge and thank all previous and current members of the GetMePPE Chicago leadership and volunteer team, especially the donors and partners that made our efforts possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Northwestern University, Feinberg School of Medicine’s Center for Bioethics & Medical Humanities: COVID-19 Ethics & Humanities Grant.