
Abstract
Objectives
National data on the health of children and adolescents exposed to commercial sexual exploitation (CSE) are lacking, during both adolescence and adulthood. Using nationally representative data, we examined the health of male and female adolescents in grades 7-12 who experienced CSE exposure and subsequent adult health outcomes and access to health care.
Methods
Our retrospective cohort study used data from Waves I-IV of the National Longitudinal Study of Adolescent to Adult Health (1994-2008) to characterize relationships between CSE exposure before or during adolescence and health during adolescence and adulthood. The analytic sample included 10 918 adult participants aged 24-34 in Wave IV. We performed bivariate analyses, stratified by sex, to quantify the relationship between CSE exposure before or during adolescence and adolescent and adult health outcomes.
Results
Four percent of participants reported having a CSE exposure before or during adolescence (5% of males, 3% of females). Factors associated with CSE exposure among adolescents included race/ethnicity, parental education level, previous abuse, same-sex romantic attractions, history of ever having run away from home, and substance use. During adolescence, exposure to CSE was associated with worse overall health, depressive symptoms, and suicidal thoughts for both males and females. In adulthood, adolescent CSE exposure was associated with depression among males and functional limitations among females. A higher percentage of males with CSE exposure before or during adolescence, compared with their non–CSE-exposed peers, used the emergency department as their usual source of care during adulthood.
Conclusions
CSE exposure before or during adolescence was associated with poor adolescent and adult health outcomes and health care access. Observed differences between males and females warrant further exploration.
Adolescents exposed to commercial sexual exploitation (CSE) face intersecting vulnerabilities and heightened risks for poor health outcomes. 1,2 The term CSE overlaps with child sex trafficking and is defined as the exchange of sexual activity for anything of value. 3 CSE among children and adolescents aged <18 years is a form of child sexual abuse and a human rights violation. 3 The exact prevalence of CSE among children and adolescents in the United States is unknown but is believed to be considerable. 1,3 Common risk factors for CSE among young people include a history of previous abuse, child welfare involvement, justice involvement, parental incarceration, familial rejection, unstable housing, mental health disorders, and substance use disorders. 3-5 Young people who belong to a racial/ethnic minority group, are of low socioeconomic status, are female, or identify as lesbian, gay, bisexual, or transgender also have increased risk for CSE. 1,2,4 Together, risk factors for and sequelae of CSE portend heightened risk for poor health during adolescence 1 and potentially into adulthood. 3,4
Emerging literature on CSE documents substantial health effects of CSE. 1,2,4,6,7 Adverse health outcomes of CSE among young people include unplanned pregnancy, sexually transmitted infections, and violence-related injury. 2,7 Mental health implications are also profound: young people affected by CSE often have underlying mental health conditions and trauma that develop because of or become exacerbated by CSE. 1,2,7,8 Furthermore, substance use disorders may develop or worsen as a result of CSE, because many exploiters use alcohol or drugs to lure adolescents into exploitation or keep them exploited. 8,9 Yet, despite the high health needs of young people exposed to CSE, substantial barriers to health care access exist, including fear of police in health care settings, fear of retribution from exploiters, and lack of transportation or means to pay for care. 10,11
Although the treatment needs of young people exposed to CSE are believed to be high, national studies of CSE among young people tend to focus on a small number of health outcomes. Furthermore, it is unclear how the health needs of young people exposed to CSE translate across the life course. To date, most studies on CSE among young people have involved small cohorts, and longitudinal data are sparse, in part because of practical and ethical concerns that arise with longitudinal follow-up. 1,12
Studies of nationally representative databases show that, compared with peers who do not have a history of CSE exposure, young people with a history of CSE exposure are more likely to have a physical or cognitive disability; engage in sexual risk behaviors; use illicit substances and engage in delinquent acts; have high rates of sexually transmitted infections; have mental health challenges, including depression, posttraumatic stress disorder, and suicidality; and have lower academic performance and attainment. 5,13 -16 National studies indicate differences by sex, with odds of CSE twice as high among males than among females in the United States, contradicting previous beliefs and research suggesting that CSE is more common among females. 5,15 Differences in risk factors by sex have also been demonstrated in studies involving young adults, with a higher risk of CSE noted among males with a history of child sexual abuse or sexually transmitted infections compared with females. 5,15
Comprehensive measurement of health and health care access and use patterns among males and females with a history of CSE exposure in the United States is lacking in the literature. Furthermore, most national studies do not adequately frame analyses within the CSE literature (eg, they use outdated terminology that lacks reflection of victimization [eg, “traded sex,” “prostitution”]) and do not examine adult health or health care access and use. Thus, to better understand experiences of CSE among males and females, to examine large samples, and to move beyond cross-sectional analyses, 7 we describe health-related characteristics of males and females who were exposed to CSE before or during adolescence and examine their subsequent adult health outcomes and health care access and use patterns using nationally representative data.
Methods
Study Design
We used data from Waves I-IV of the National Longitudinal Study of Adolescent to Adult Health (Add Health, 1994-2008) to conduct a retrospective cohort study examining the relationship between CSE exposure before or during adolescence and adolescent and adult health. We investigated the influence of CSE exposure on males and females, examining 5 aspects of health: overall health, mental health, substance use, social health, and health care use.
Data and Study Population
Wave I (1994-1995 school year) included 20 745 adolescents in grades 7-12 recruited from junior high and high schools (primary sampling unit), who completed in-home interviews and then were invited to participate in follow-up waves. Wave II occurred in schools 1 academic year later (1996). Waves III and IV included in-home interviews that were conducted in 2001-2002 and 2008-2009, respectively. Wave IV included 15 701 respondents aged 24-34 from Wave I. Written informed consent was obtained from participants. The sampling procedures and study design are described elsewhere. 17 Our analytic sample (N = 10 918) included Wave IV participants with CSE data in Wave I or Wave II and a valid sample weight.
Measures
Adolescent CSE exposure
Respondents were asked in Wave I if they had ever exchanged sex for drugs or money. A second item asked participants to report the frequency with which they had exchanged sex for drugs or money (ie, the number of times). In Wave II, participants were asked to report the number of times since the Wave I interview they had exchanged sex for drugs or money. Respondents who reported any history of CSE exposure during Wave I or Wave II were included in the adolescent CSE exposure group. In addition, responses to the Wave I and Wave II survey on the number of times respondents had exchanged sex for drugs or money were combined to create a “frequency of CSE” measure.
Adolescent health–related characteristics and adult outcomes
Adolescent health–related characteristics and adult health outcomes were drawn from Waves I and IV, respectively, except for retrospective items on childhood abuse, which were drawn from Wave III. We examined adolescent sociodemographic characteristics collected during Wave I, including age, sex (male, female), race/ethnicity (White, African American, Hispanic, “Other” [ie, Asian/Pacific Islander, American Indian/Native American, other, and multiracial]), annual household income (<$25 000, $25 000-$49 999, $50 000-$74 999, ≥$75 000), highest level of parental educational (<high school diploma, high school diploma, some college, ≥college degree), family structure (2 biological parents, 2 parents, single parent, other), and geographic region (Midwest, Northeast, South, West). We also examined other factors associated with adolescent CSE exposure, 13 including ever having had a same-sex romantic attraction and ever having run away from home. In Wave III, participants were asked retrospectively how often they had experienced parental physical abuse (slapped/hit/kicked), parental sexual abuse (inappropriate sexual touching or forced sexual relations), or emotional neglect by a parent or caregiver before sixth grade. We used participant responses to create 4 measures of abuse/neglect (never, once, twice, ≥3 times). At the time of the Wave III Add Health survey, child and adolescent CSE exposure was not commonly recognized as a form of sexual abuse. 18
Overall health
During Waves I and IV, respondents self-rated their health (poor, fair, good, very good, excellent) using a well-validated single-item general health measure associated with morbidity and mortality. 19 Aligned with previous studies and based on the distribution of responses in the relatively young and healthy Add Health cohort, we classified respondents as having poor overall health if they rated their health as poor, fair, or good. 20
Substance use
We used Wave I responses to single items (frequency of alcohol use, number of times drunk within the last year, age of initiation of marijuana use, frequency of marijuana use) to indicate adolescent alcohol and marijuana use. Adult substance abuse was defined based on responses to 4 items that asked about life problems related to substance use in the previous 12 months at Wave IV: problems at work or school, endangering self or others, legal problems, and problems involving interpersonal relationships. Participants who reported ≥2 occurrences of life problems attributed to alcohol use were considered to have adult alcohol abuse. 21 Likewise, participants who indicated ≥2 occurrences of life problems attributed to marijuana or other drug use were considered to have adult marijuana or other drug use, respectively.
Mental health
Respondents were asked in Waves I and IV whether they had had depressive symptoms in the previous 7 days and whether they had had suicidal thoughts within the past year. Depressive symptoms were measured using the short-form Center for Epidemiologic Studies Depression Scale, a validated 10-item scale. Aligned with previous studies, a cutoff of ≥11 was used to identify respondents at high risk of depression. 22 Suicidal ideation was measured via an item asking whether they had seriously considered suicide within the previous 12 months.
Functional limitations
Wave I respondents reported on difficulty using limbs because of a permanent physical condition, and Wave IV respondents reported on difficulty with climbing flights of stairs. We categorized participants as having functional limitation if they responded yes in Waves I and IV, respectively.
Social health
In Wave IV, participants were asked where they would rank their standing on a ladder with 10 rungs, with the top rung being for people with the most money, education, and respected jobs and the lowest rung for people with the least money, education, and respected jobs or no job. Responses were considered a continuous measure of social standing. In addition, respondents were asked the number of times they had been married (0, 1, ≥2), their educational attainment (<high school diploma, high school diploma, some college, and ≥college degree), and if they had ever been incarcerated (yes/no).
Health care access and use
During Wave I, respondents were asked whether they had had a physical examination in the past year and whether they had received counseling or mental health therapy in the past year. In Wave IV, participants were asked if they had health insurance and the location of usual care during adulthood. Usual care was categorized as a primary care setting (hospital-based clinic; community health clinic; health maintenance organization; private medical office; school, college, or work clinic; military hospital; or clinic), emergency department or non–primary care site, or respondent “never gets sick.”
Statistical Analysis
We performed bivariate analyses, stratified by sex, to quantify the relationship between CSE exposure before or during adolescence and adolescent and adult health outcomes (ie, poor overall health, substance use, depression, suicidality, functional limitations, social health, health care access and use). We used the Rao–Scott χ2 test to determine significant associations between CSE (exposure/no exposure) and categorical variables. We used the adjusted Wald F test to determine significant differences in means across CSE (exposure/no exposure) for the following variables: age, age when first tried marijuana, number of times used marijuana, and social standing. We considered P < .05 to be significant. We conducted analyses using Stata version 14 (StataCorp LLC). Analyses, including prevalence percentages, accounted for the clustered, stratified survey design and used survey weights (provided with the dataset) to generate national population estimates. The University of California, Los Angeles, Institutional Review Board approved this study.
Results
Of 10 918 participants, 411 (weighted prevalence, 4%) reported CSE exposure during childhood or adolescence (5% of males, 3% of females). Of the 411 participants who disclosed having a CSE exposure before or during Wave I or Wave II, 4 disclosed having had a CSE exposure by age 20, 2 by age 21, and 405 by age ≤19. Of participants who reported no CSE exposure, 50% were female and 50% were male. Of participants who reported having had 1 episode of CSE exposure before or during adolescence, 39% were female and 61% were male. Of participants who reported repeat CSE exposure before or during adolescence, 29% were female and 71% were male.
Adolescent Health–Related Characteristics
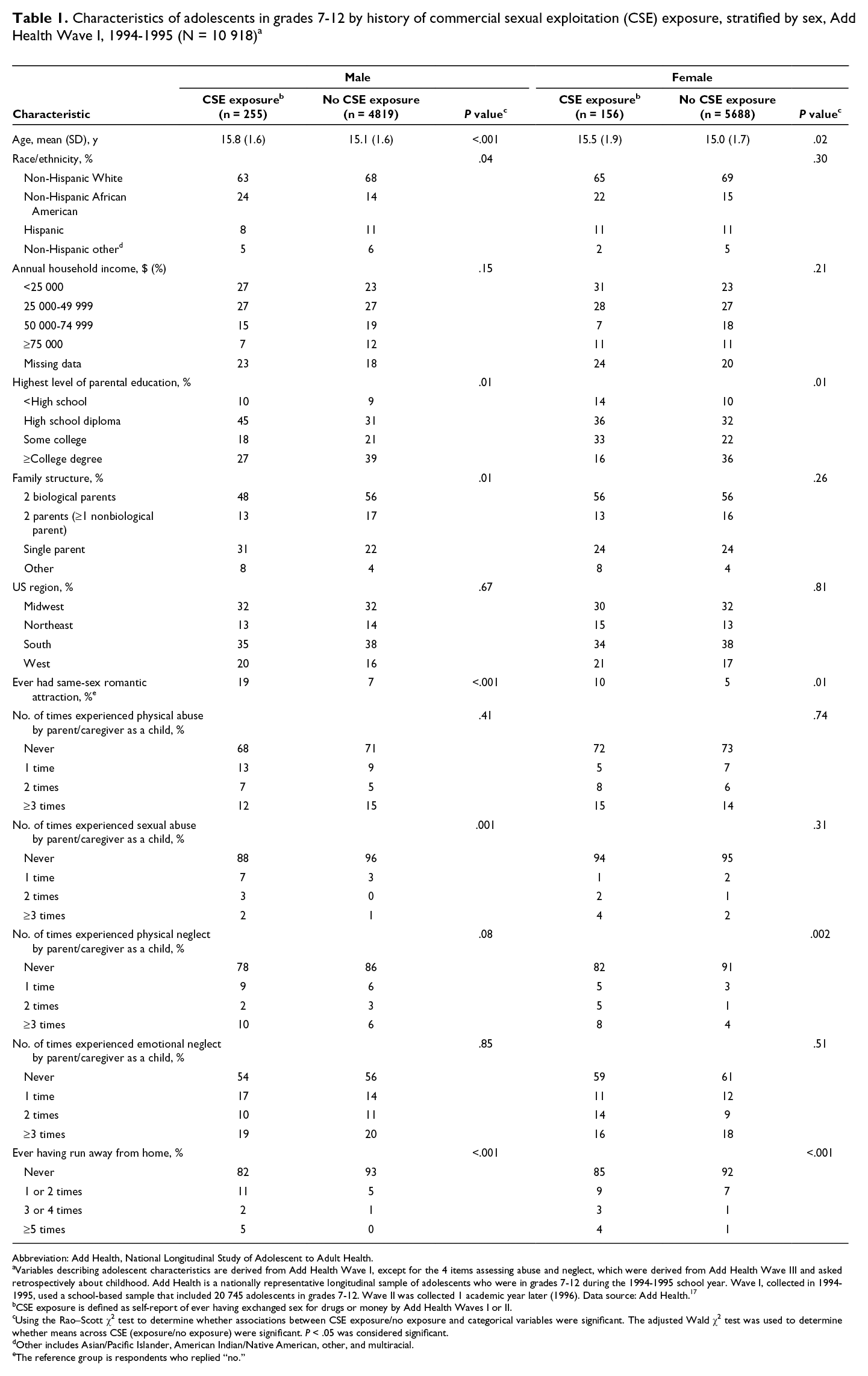
In our analysis of weighted sociodemographic characteristics of the sample by history of adolescent CSE exposure, adolescent factors that were significantly associated with CSE exposure included age, race/ethnicity (males only), parental education level, family structure (males only), same-sex romantic attraction, previous abuse or neglect, and a history of ever having run away from home (Table 1). A higher percentage of adolescents with CSE exposure, compared with their same-sex peers, reported parents with less than a college degree. A higher percentage of male respondents with a history of CSE exposure, compared with male respondents with no history of CSE exposure, were African American and lived in single-parent households.
Characteristics of adolescents in grades 7-12 by history of commercial sexual exploitation (CSE) exposure, stratified by sex, Add Health Wave I, 1994-1995 (N = 10 918) a
Abbreviation: Add Health, National Longitudinal Study of Adolescent to Adult Health.
aVariables describing adolescent characteristics are derived from Add Health Wave I, except for the 4 items assessing abuse and neglect, which were derived from Add Health Wave III and asked retrospectively about childhood. Add Health is a nationally representative longitudinal sample of adolescents who were in grades 7-12 during the 1994-1995 school year. Wave I, collected in 1994-1995, used a school-based sample that included 20 745 adolescents in grades 7-12. Wave II was collected 1 academic year later (1996). Data source: Add Health. 17
bCSE exposure is defined as self-report of ever having exchanged sex for drugs or money by Add Health Waves I or II.
cUsing the Rao–Scott χ2 test to determine whether associations between CSE exposure/no exposure and categorical variables were significant. The adjusted Wald χ2 test was used to determine whether means across CSE (exposure/no exposure) were significant. P < .05 was considered significant.
dOther includes Asian/Pacific Islander, American Indian/Native American, other, and multiracial.
eThe reference group is respondents who replied “no.”
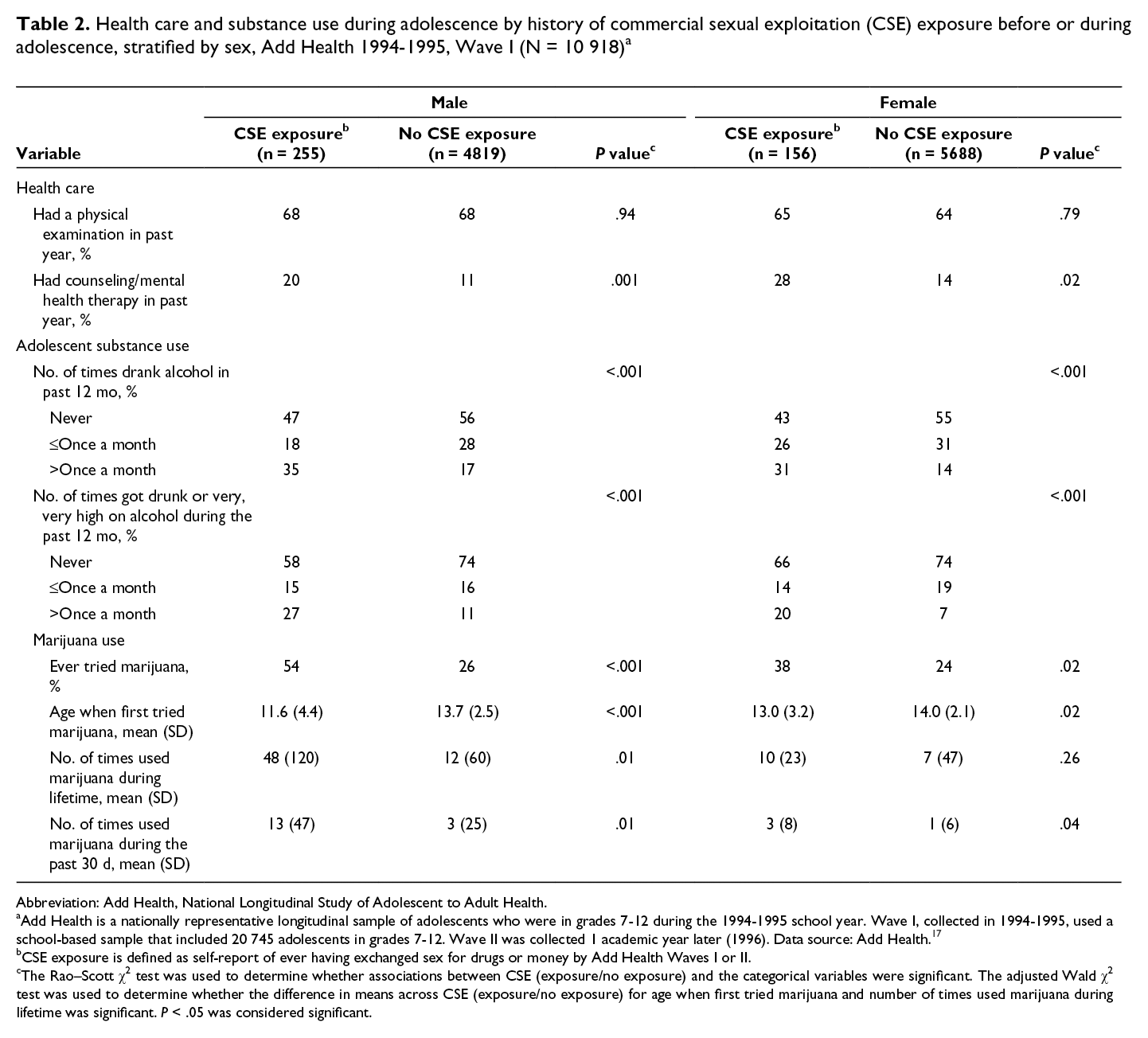
Compared with adolescents with no history of CSE exposure, adolescents with a history of CSE exposure were significantly more likely to access counseling or mental health therapy, had a higher prevalence and frequency of adolescent alcohol and marijuana use, and were younger at first marijuana use (Table 2).
Health care and substance use during adolescence by history of commercial sexual exploitation (CSE) exposure before or during adolescence, stratified by sex, Add Health 1994-1995, Wave I (N = 10 918) a
Abbreviation: Add Health, National Longitudinal Study of Adolescent to Adult Health.
aAdd Health is a nationally representative longitudinal sample of adolescents who were in grades 7-12 during the 1994-1995 school year. Wave I, collected in 1994-1995, used a school-based sample that included 20 745 adolescents in grades 7-12. Wave II was collected 1 academic year later (1996). Data source: Add Health. 17
bCSE exposure is defined as self-report of ever having exchanged sex for drugs or money by Add Health Waves I or II.
cThe Rao–Scott χ2 test was used to determine whether associations between CSE (exposure/no exposure) and the categorical variables were significant. The adjusted Wald χ2 test was used to determine whether the difference in means across CSE (exposure/no exposure) for age when first tried marijuana and number of times used marijuana during lifetime was significant. P < .05 was considered significant.
Adolescent to Adult Health by CSE Exposure
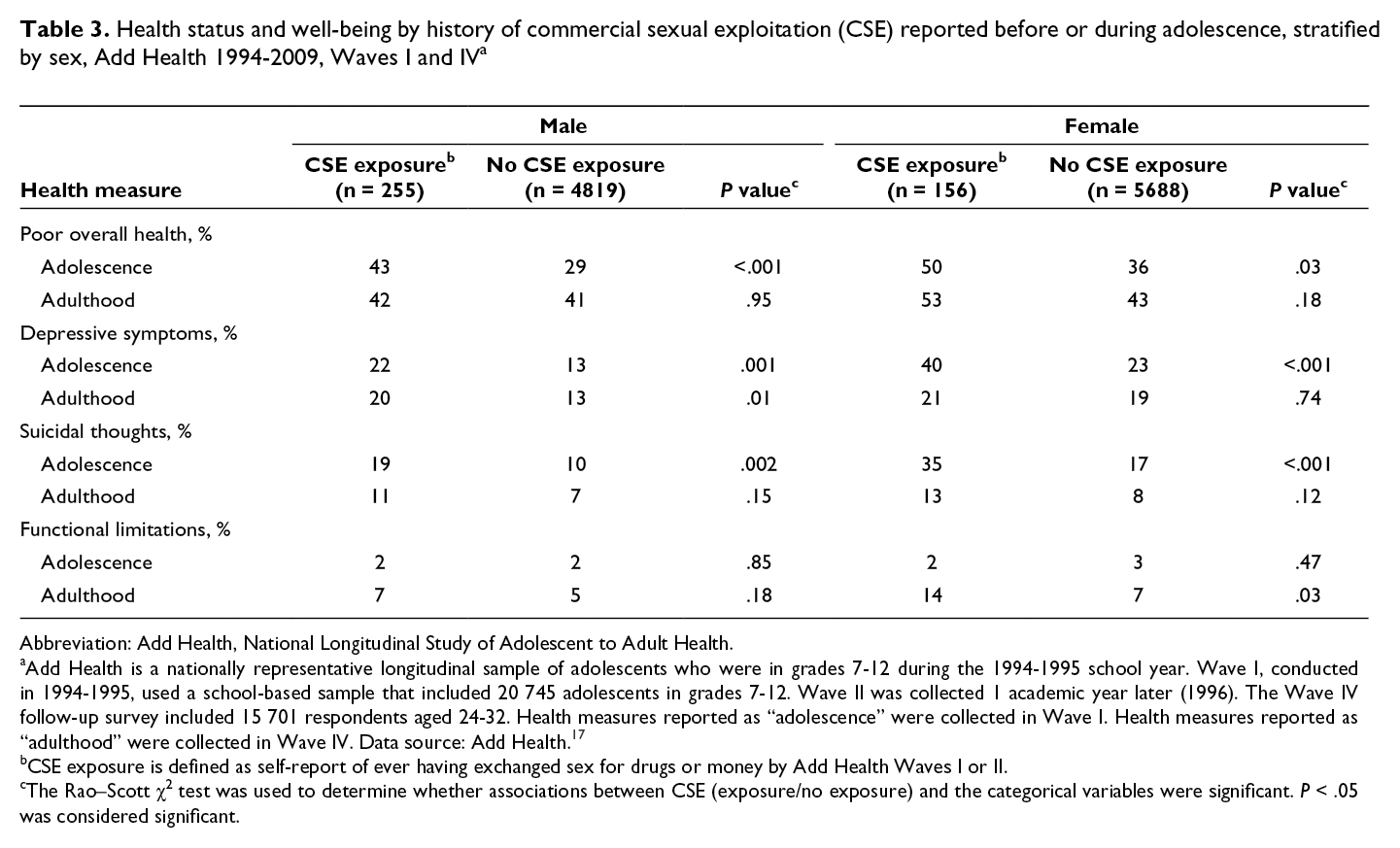
Compared with adolescent males and females with no history of CSE exposure, males and females with a history of CSE exposure were more likely to report worse overall health, depressive symptoms, and suicidal thoughts during adolescence (Wave I; Table 3). In addition, compared with males with no history of CSE exposure before or during adolescence, males with a history of CSE exposure before or during adolescence were more likely to report depressive symptoms in adulthood, and females were more likely to report functional limitations in adulthood (Wave IV).
Health status and well-being by history of commercial sexual exploitation (CSE) reported before or during adolescence, stratified by sex, Add Health 1994-2009, Waves I and IV a
Abbreviation: Add Health, National Longitudinal Study of Adolescent to Adult Health.
aAdd Health is a nationally representative longitudinal sample of adolescents who were in grades 7-12 during the 1994-1995 school year. Wave I, conducted in 1994-1995, used a school-based sample that included 20 745 adolescents in grades 7-12. Wave II was collected 1 academic year later (1996). The Wave IV follow-up survey included 15 701 respondents aged 24-32. Health measures reported as “adolescence” were collected in Wave I. Health measures reported as “adulthood” were collected in Wave IV. Data source: Add Health. 17
bCSE exposure is defined as self-report of ever having exchanged sex for drugs or money by Add Health Waves I or II.
cThe Rao–Scott χ2 test was used to determine whether associations between CSE (exposure/no exposure) and the categorical variables were significant. P < .05 was considered significant.
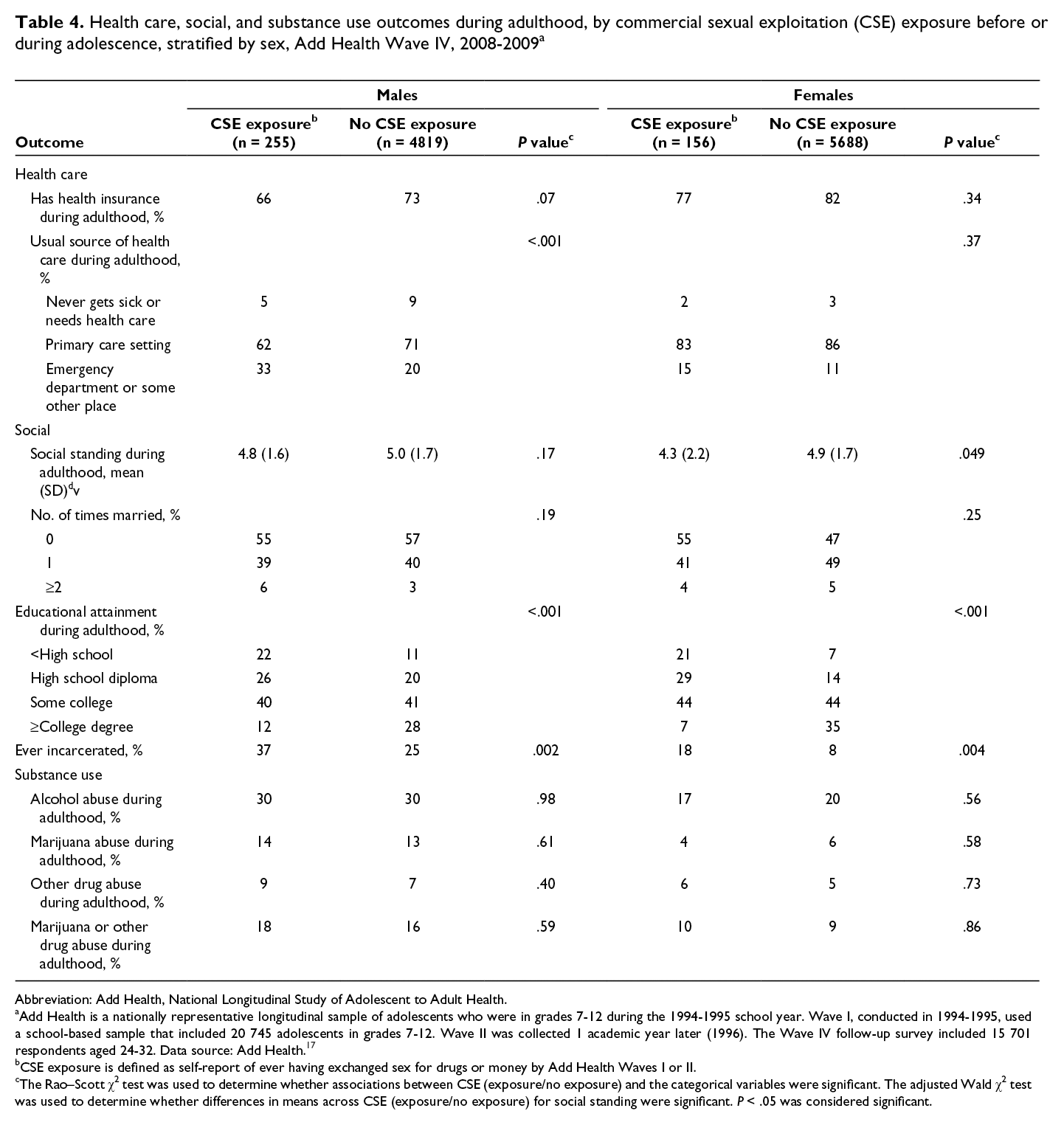
Compared with males with no history of CSE exposure before or during adolescence, males with a history of CSE exposure were more likely to report using the emergency department as their usual source of care in adulthood (Table 4). Compared with females with no history of CSE exposure before or during adolescence, females with a history of CSE exposure before or during adolescence reported a significantly lower perceived social standing. By adulthood, compared with same-sex peers, males and females with a history of CSE exposure before or during adolescence were more likely to have ≤high school diploma and to have ever been incarcerated. Health insurance status, marital history, and substance use outcomes did not differ significantly among adults by CSE exposure history.
Health care, social, and substance use outcomes during adulthood, by commercial sexual exploitation (CSE) exposure before or during adolescence, stratified by sex, Add Health Wave IV, 2008-2009 a
Abbreviation: Add Health, National Longitudinal Study of Adolescent to Adult Health.
aAdd Health is a nationally representative longitudinal sample of adolescents who were in grades 7-12 during the 1994-1995 school year. Wave I, conducted in 1994-1995, used a school-based sample that included 20 745 adolescents in grades 7-12. Wave II was collected 1 academic year later (1996). The Wave IV follow-up survey included 15 701 respondents aged 24-32 years. Data source: Add Health. 17
bCSE exposure is defined as self-report of ever having exchanged sex for drugs or money by Add Health Waves I or II.
cThe Rao–Scott χ2 test was used to determine whether associations between CSE (exposure/no exposure) and the categorical variables were significant. The adjusted Wald χ2 test was used to determine whether differences in means across CSE (exposure/no exposure) for social standing were significant. P < .05 was considered significant.
Discussion
To our knowledge, this is the first study to examine a broad set of adolescent and adult health associations with childhood and adolescent CSE exposure using nationally representative data. We found that CSE exposure before or during adolescence was common—1 in 25 young people reported experiencing CSE during adolescence—confirming findings from previous Add Health studies, 1,23 and the prevalence and frequency of adolescent CSE exposure was higher among males than among females. Males face many barriers to identification and access to health care and social services in the community, 3 some of which may have been overcome by the confidential format of the Add Health survey. 17 We could not determine whether adolescent health risks emerged before, during, or after the exploitation; however, heightened health vulnerability for both US males and females with a history of child or adolescent CSE exposure was apparent. Although some health outcome differences disappeared by adulthood, poorer outcomes were observed in physical, behavioral, and social health domains, with important differences between males and females.
Adolescent Health and CSE Exposure
Consistent with literature on risk factors for CSE, 1,3 identified adolescent factors associated with CSE exposure included parental education level, same-sex romantic attractions, and ever having run away from home, a marker of familial rejection and/or being unstably housed. 3 Several expected factors were significant only for males, although these factors may not have been significant for females because of smaller sample size of females with a history of CSE exposure. Overall, our findings support the factors associated with CSE recognized in the literature. 1 Our findings underscore the need to address underlying structural factors, such as marginalization of sexual minority young people and the importance of understanding intersectional aspects of identity, which may portend vulnerability for child or adolescent CSE exposure, with attention paid to males, an often overlooked portion of the CSE-exposed population 3 that we now understand is quite large.
A higher percentage of males and females with a history of CSE exposure, compared with their same-sex peers, reported alcohol and marijuana use, as well as recent receipt of mental health care. These findings align with existing literature indicating access to mental health treatment among young people with a history of CSE exposure—which may relate to high levels of involvement in juvenile justice and child welfare systems—without necessarily using or engaging in treatment. 8,24 Of note, access to treatment does not necessarily imply uptake of treatment services, because young people exposed to CSE have unique needs and a strong preference for self-determination in their care. 10,24 In addition, both males and females with CSE exposure were more likely than their same-sex peers to report worse overall health, depressive symptoms, and suicidal thoughts during adolescence. Our findings align with literature documenting high mental health needs among young people with a history of CSE exposure, which is especially important given that mental health may contribute to cycles of exploitation and ongoing health risks. 8
Adult Health
To our knowledge, adult health trajectories of people with CSE exposure before or during adolescence have rarely been described. Associations of CSE exposure with poor overall health and substance use and suicidality observed during adolescence, compared with same-sex non–CSE-exposed peers, leveled off by adulthood. However, the prevalence of depression was elevated among adult males exposed to CSE before or during adolescence compared with males not exposed to CSE before or during adolescence. In addition, adult women had higher rates of functional limitations than their same-sex peers, which may reflect adult physical and/or mental health status. Levels of access to primary care among males exposed to CSE were lower than among males not exposed to CSE. Finally, compared with their same-sex peers, males and females exposed to CSE before or during adolescence had lower educational attainment and a higher likelihood of having been incarcerated, and CSE-exposed females had lower perceived social standing. These findings indicate vulnerability related to factors influencing adult success, such as educational achievement, and ongoing health risks into adulthood for both males and females. Our findings also suggest that the experience of CSE and its potential effect on health may differ among males and females. In addition, our findings highlight the need to better understand life-course trajectories of CSE-exposed adolescents and the need for prevention of child and adolescent CSE, ideally by addressing antecedent childhood and adolescent factors associated with CSE.
Limitations
Our study had several limitations. First, the adolescent data were collected in the 1990s, and only a binary definition of sex was available in the dataset. The gender identity of young people with a history of CSE exposure is an area for further inquiry. 1 Second, the definition of CSE exposure was based on a single item asking about the history of having traded sex for drugs or money. Thus, the CSE exposure variable does not include survival sex or exploitation for other items of value (eg, housing, food, medicine), and not all victims acknowledge having traded sex, 3 which may have led to underreporting of the exposure variable. Other variables have limited definitions; for example, the abuse variables considered only abuse by parents or caregivers, and additional impairments exist beyond the impairments captured in the variable on functional limitations. Adult trafficking and intersection with labor trafficking were not considered. Also, the legal conceptualization and awareness of CSE as abuse rather than as child prostitution has changed, as have perceptions about substance use, 18 although the nonjudgmental self-report items may have mitigated social desirability bias. Third, the analyses did not allow us to identify mechanisms for observed relationships. Future studies that examine differences in CSE exposure (eg, among non-Hispanic African American males) and potential causal pathways are needed to shed light on longer-term health effects of CSE exposure. Nevertheless, the findings provide an understanding of adolescent to adult health among people with a history of CSE exposure as children or adolescents that can inform further research and policy, indicating potential pathways for intervention, particularly with regard to the gendered aspect of CSE.
Conclusions
CSE exposure before or during adolescence was associated with adolescent and adult health outcomes and health care access. Differences in CSE exposure among male and female adolescents warrant further exploration to identify mechanisms for observed differences in prevalence, health outcomes, and access to care by sex; to develop and test effective prevention interventions for males and females; and to bolster young people’s resilience by promoting their health after CSE exposure.
Footnotes
Acknowledgments
The authors thank the University of California, Los Angeles, Pediatrics Health Services Research Longitudinal Data Group for their conceptual contributions to the analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Barnert’s time was funded by the National Institute on Drug Abuse (K23-DA04747) and the University of California, Los Angeles, Children’s Discovery and Innovation Institute.