
Abstract
Objectives
Disparities in substance use disorder (SUD) treatment use persist across groups, including gender. Using a gender-informed approach to expand treatment capacity and reduce barriers to treatment engagement is vital. We examined SUD treatment need and receipt among people with SUD in the United States, by gender, and assessed gender-specific sociodemographic factors associated with unmet need for SUD treatment and reported treatment barriers.
Methods
We conducted an analysis of data among adults aged ≥18 with a past-year SUD from the National Survey on Drug Use and Health (2015-2018). We computed population-adjusted frequencies and proportions for SUD treatment need and receipt and assessed gender differences. Multivariate logistic regression assessed gender-specific sociodemographic variables associated with SUD treatment receipt.
Results
Among adults with a past-year SUD, 63.4% were men and 36.6% were women (P < .001), only 10.6% received SUD treatment, and a greater percentage of women than men needed treatment for opioid use disorder (11.9% vs 9.9%; P = .002). Receipt of SUD treatment was lowest among women with alcohol use disorder followed by men with alcohol use disorder (7.5% vs 8.9%; P = .052). Non-Latinx Black men had fewer than half the adjusted odds of receiving SUD treatment than non-Latinx White men (adjusted odds ratio [aOR] = 0.44; 95% CI, 0.27-0.71). Latinx women (aOR = 0.37; 95% CI, 0.18-0.73) and non-Latinx Black women (aOR = 0.51; 95% CI, 0.27-0.94) had significantly lower odds of receiving SUD treatment than non-Latinx White women.
Conclusions
As public health efforts target expanding SUD treatment capacity and addressing disparities in use of SUD treatment, interventions informed by gender and culture should be prioritized.
In 2017, the US Department of Health and Human Services called for increased access to prevention, treatment, and recovery support services to combat the overdose crisis. 1 Despite increased attention to treatment for opioid use disorder (OUD) along with other substance use disorders (SUDs) in recent years, large disparities in SUD treatment use persist nationally. Although 20.7 million people needed SUD treatment in 2017, only 4 million received services. 2 Even with policy changes, such as Medicaid expansion, the unmet treatment need remains. 3
The overdose crisis has brought changes in epidemiologic patterns of SUD treatment need by sex and gender. 4,5 For example, although adult men are more likely than adult women to have OUD, the rates of OUD diagnoses and overdose events increased more rapidly among women than men during the past decade. 4,5 Deaths related to alcohol use have followed a similar trend, indicating a substantial female disadvantage. 5 Gender affects SUD risk, disease course, and treatment. 6 Women typically progress more quickly from substance use to addiction than men 7 as well as have more severe disease and more medical and psychosocial comorbidities at treatment initiation. 8 However, once engaged in SUD treatment, women and men tend to have similar treatment outcomes. 9 Thus, evidence supports the need for careful evaluation of the evolving gender makeup of SUDs in the United States to guide public health efforts aimed at combatting the opioid crisis and addressing SUDs.
Gender likely also modifies SUD treatment access and use. Historically, the literature reliably supported the idea that women with SUD were less likely than men with SUD to enter SUD treatment. 10 However, more recent work examining unmet SUD treatment need by gender highlights inconsistencies across groups, such as race and ethnicity. 11,12 In addition, studies have found various barriers to treatment that likely contribute to gender disparities in receipt of SUD treatment, including (for women) pregnancy, child care responsibilities, fear of child welfare report, stigma, financial limitations, psychiatric comorbidities, and negative attitudes toward treatment. 10
Adopting a gender-informed approach is vital to effective public health strategies that target the expansion of treatment capacity and the reduction of barriers to treatment engagement. Planning and implementation of a gender-informed approach require guidance from national data stratified by gender. 13 Presenting data in this manner aligns with the greater call for more gender-based research on SUD. 14 The primary objective of our study was to report on the unmet needs and receipt of SUD treatment by gender and substance type (ie, illicit drugs, alcohol) among people with a past-year SUD using data from the National Survey on Drug Use and Health (NSDUH) for 2015-2018. In doing so, we analyzed outcomes separately for OUD, given its increased attention as a result of the current opioid crisis. We also assessed gender-specific sociodemographic factors associated with unmet SUD treatment need and reported barriers to SUD treatment.
Materials and Methods
NSDUH is an annual survey of the civilian, noninstitutionalized US population conducted by the Substance Abuse and Mental Health Services Administration. 15 It is a core source of epidemiologic data on behavioral health conditions and their treatments, including SUD, and its data are routinely used to inform national and state public health initiatives. NSDUH uses a stratified multistage area probability sampling technique to capture data representative of the entire United States. People experiencing homelessness, active-duty military, and institutional residents (eg, residents of jails, nursing homes) are not included. The target sample size during the study period was 67 500 interviews per year. Surveys are conducted face-to-face in the respondent’s household using audio computer-assisted self-interviewing. 16 For our study, we aggregated publicly available data from NSDUH 2015-2018 to facilitate robust gender-stratified analyses.
Study Sample
During 2015-2018, a total of 171 766 adults participated in NSDUH, equivalent to a population of 245 838 163 adults when NSDUH sampling weights were applied. Approximately 19.2 million people, or 7.8% (95% CI, 7.7%-8.0%), had a past-year SUD. Men and women aged ≥18 with past-year SUD treatment need composed the study sample. We classified respondents as having SUD treatment need if they either met criteria for SUD and/or expressed need for SUD treatment during the past year. We classified respondents as having an SUD if they met criteria for dependence or abuse for any of the following substances: alcohol or an illicit drug, which included marijuana, hallucinogens, inhalants, methamphetamine, tranquilizers, cocaine, heroin, pain relievers, stimulants, and/or sedatives. NSDUH uses the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) 17 criteria survey questions to assess dependency and abuse. 15 Respondent self-reported data determined expressed treatment need. Nicotine addiction was not included. OUD was defined as meeting SUD criteria for either heroin and/or pain relievers. Hereinafter, we refer to all respondents with a past-year SUD treatment need as “with SUD.”
Although sex (biological constructs) and gender (social constructs) are separate variables that interact to influence health, 13 NSDUH only captures data on a single self-reported dichotomous variable (rather than 2 variables to capture both sex and gender). Given these limitations of NSDUH as well as our study objective to assess sociodemographic variables associated with SUD treatment receipt (and that gender is a vital sociocultural variable), 18 we refer to men and women throughout the study.
Measurement of Study Outcomes
NSDUH respondents self-report data on treatment receipt using a broad definition. SUD treatment could have been received at a specialty clinic (ie, drug or alcohol rehabilitation or mental health center) or any other treatment center (ie, hospital, emergency department, private physician’s office, prison or jail, self-help group). Because of limitations in NSDUH, we could not collect data on length or type (eg, medication) of treatment received. The proportion of men and women with SUD who did not receive SUD treatment composed the population with unmet SUD treatment need. In addition, we collected data on SUD treatment receipt among the subgroup that expressed a past-year need for SUD treatment for the total sample and by gender.
Among men and women with an expressed SUD treatment need, we collected data on reported barriers to treatment. We subclassified barriers into the following categories: financial (could not afford treatment/no health insurance/health insurance did not cover cost of treatment), transportation or time (did not have transportation to treatment/did not have time for treatment), desired treatment unavailable or full (did not know where to go for treatment/no openings in desired treatment program/desired treatment not offered), negative opinion about treatment (could handle substance use problem without treatment/have negative opinion of treatment/did not think treatment would help/did not feel a need for treatment/did not wish to stop substance use), worried about effect on job and/or reputation (did not want others to find out about treatment/concerned that treatment would have a negative effect on job), and other (barrier not listed in survey).
Data Analysis
We computed population-adjusted frequencies and proportions using the population weights assigned to each observation in the NSDUH public-use data file. Among men and women with SUD, we calculated and compared gender-specific proportions with past-year SUD treatment need by substance type (eg, alcohol, illicit drugs) using the Pearson χ2 test. We calculated similar analyses by gender for treatment receipt and barriers to treatment. We considered P ≤ .05 to be significant.
We performed multivariable logistic regression to assess sociodemographic factors associated with receipt of SUD treatment separately by gender among respondents with SUD. We selected sociodemographic variables determined a priori based on previous literature and clinical experience to be associated with receipt of SUD treatment to be included in the multivariable models. 10,12,19 We reported both unadjusted odds ratios (ORs) and ORs adjusted for all other variables in the model. We used the Wald χ2 test of significance, with P ≤ .05 considered significant. We classified men and women reporting ≥1 child aged <18 years living in the household as parenting. We defined comorbid depression by a past-year major depressive episode. We performed analysis using SAS version 9.4 (SAS Institute, Inc). As a secondary data analysis of publicly available, de-identified data, this study was exempt from institutional review board approval.
Results
About two-thirds of the study sample were men (63.4%; 95% CI, 62.1%-64.7%), and approximately one-third were women (36.6%; 95% CI, 35.3%-37.9%; P < .001). Most were non-Latinx White, were employed, were insured, were unmarried, and had ≥high school diploma (Table 1). Most rated their health as good or very good. Women were more likely than men to be younger, unmarried, and parenting, as well as to have government program assistance and comorbid depression, and men were more likely than women to identify as Latinx, have a lower education level, and lack health insurance.
Demographic characteristics of adults with substance use disorder (SUD), by gender, National Survey on Drug Use and Health, 2015-2018 a
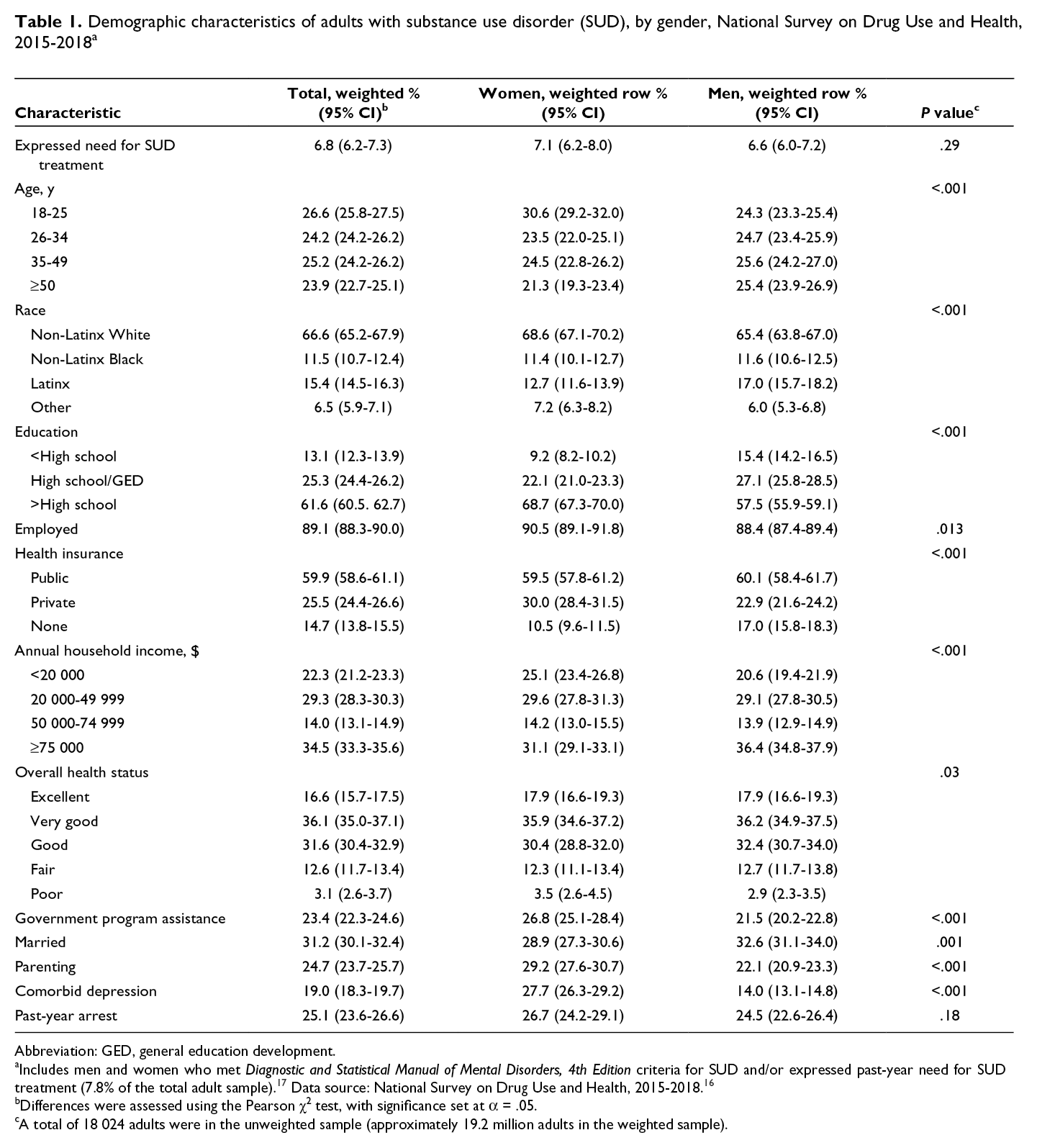
Abbreviation: GED, general education development.
aIncludes men and women who met Diagnostic and Statistical Manual of Mental Disorders, 4th Edition criteria for SUD and/or expressed past-year need for SUD treatment (7.8% of the total adult sample). 17 Data source: National Survey on Drug Use and Health, 2015-2018. 16
bDifferences were assessed using the Pearson χ2 test, with significance set at α = .05.
cA total of 18 024 adults were in the unweighted sample (approximately 19.2 million adults in the weighted sample).
Nearly the entire study population met DSM-IV SUD criteria (98.4%; 95% CI, 98.1%-98.7%). Of the small percentage of respondents who expressed a past-year need for SUD treatment (6.8%; 95% CI, 6.2%-7.3%), most also met DSM-IV SUD criteria (5.3%; 95% CI, 4.8%-5.7%), and a small percentage did not meet DSM-IV SUD criteria (1.6%; 95% CI, 1.3%-1.9%; data not shown).
Most of the study population needed treatment for alcohol use disorder (AUD) (74.5%), and approximately one-third needed treatment for an illicit drug use (eg, opioid, cocaine) disorder (35.4%) (Table 2). By substance type, a greater percentage of women than men with SUD needed treatment for OUD (11.9% vs 9.9%; P = .002). A greater percentage of adults with OUD needed treatment for use of pain relievers (women: 10.1% [95% CI, 9.2%-11.1%]; men: 7.9% [95% CI, 7.3%-8.5%]; P < .001) than use of heroin (women: 2.9% [95% CI, 2.4%-3.5%]; men: 3.3% [95% CI, 2.8%-3.7%]; P = .33).
Gender-stratified prevalence of substance use disorder (SUD) treatment need by substance type among adults with SUD, National Survey on Drug Use and Health, 2015-2018 a
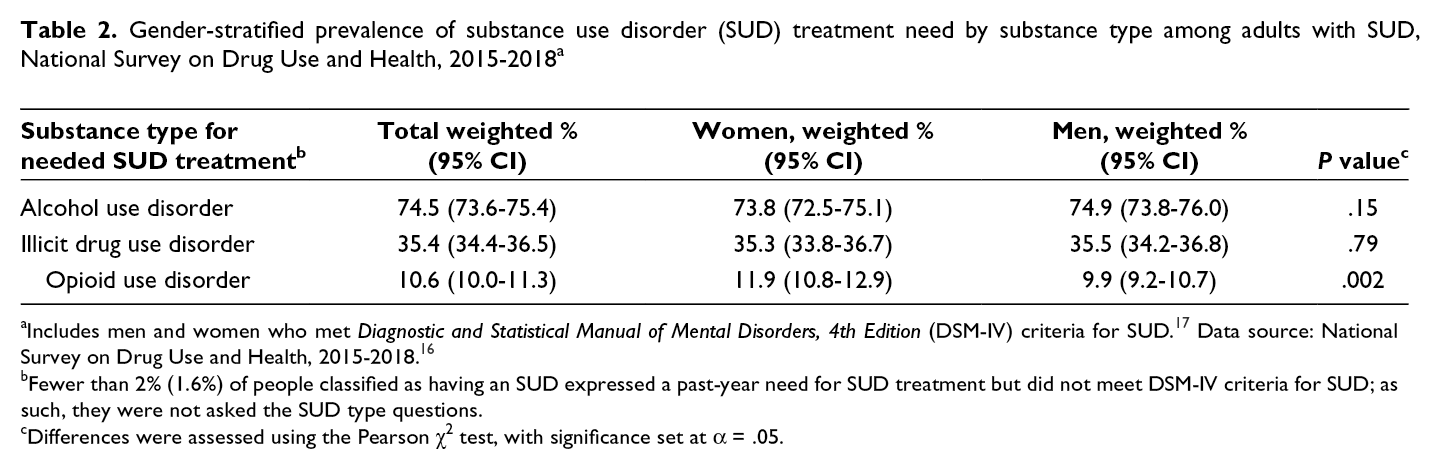
aIncludes men and women who met Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) criteria for SUD. 17 Data source: National Survey on Drug Use and Health, 2015-2018. 16
bFewer than 2% (1.6%) of people classified as having an SUD expressed a past-year need for SUD treatment but did not meet DSM-IV criteria for SUD; as such, they were not asked the SUD type questions.
cDifferences were assessed using the Pearson χ2 test, with significance set at α = .05.
A small percentage of adults received SUD treatment (10.6%), and treatment receipt did not vary by gender (Table 3). SUD treatment receipt did not change significantly during the study period among women (8.8% in 2015, 10.6% in 2016, 11.4% in 2017, 11.1% in 2018) or men (11.1% in 2015 and 2016, 10.8% in 2017, 9.9% in 2018). Fewer than 1 in 10 adults with a need for AUD treatment received services, and a smaller percentage of women with AUD than men with AUD received treatment (7.5% vs 8.9%; P = .052). Approximately one-third of men and women with a need for OUD treatment received it. Among men and women who expressed a need for SUD treatment, about one-fifth received treatment (20.1%; 95% CI, 16.7%-23.4%).
Gender-specific proportions of substance use disorder (SUD) treatment receipt by substance type among adults with SUD, National Survey on Drug Use and Health, 2015-2018 a
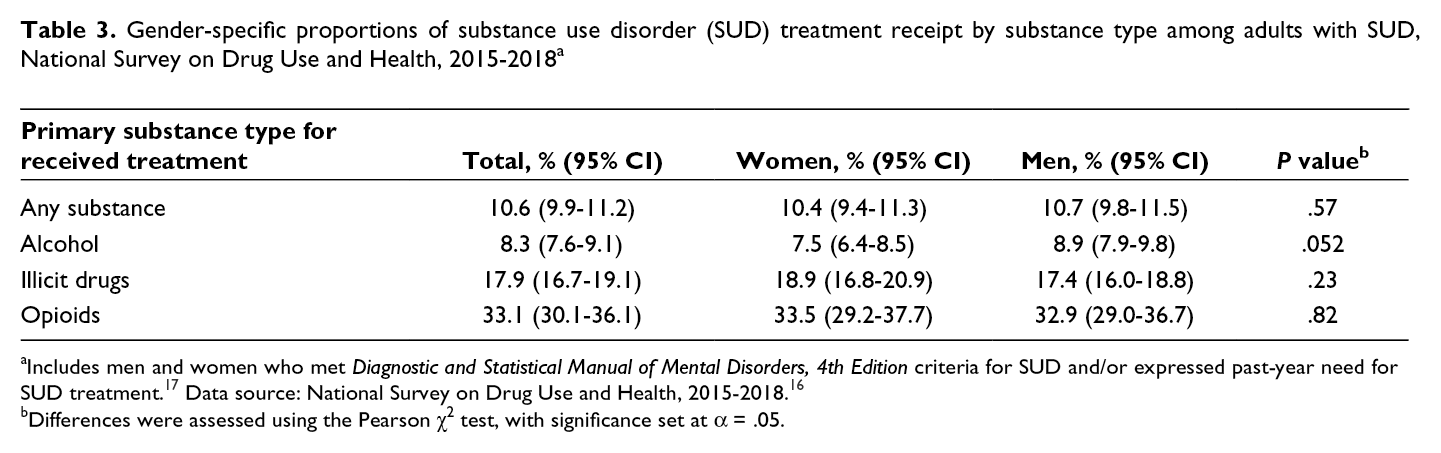
aIncludes men and women who met Diagnostic and Statistical Manual of Mental Disorders, 4th Edition criteria for SUD and/or expressed past-year need for SUD treatment. 17 Data source: National Survey on Drug Use and Health, 2015-2018. 16
bDifferences were assessed using the Pearson χ2 test, with significance set at α = .05.
In the gender-stratified adjusted multivariate analysis, certain sociodemographic factors were significantly associated with the odds of receiving SUD treatment, whereas expressing a need for treatment was not associated with treatment receipt (Table 4). Non-Latinx Black women (adjusted odds ratio [aOR] = 0.51; 95% CI, 0.27-0.94) and non-Latinx Black men (aOR = 0.44; 95% CI, 0.27-0.71) had half the odds of receiving treatment than their non-Latinx White counterparts. Latinx women had the lowest odds of receiving SUD treatment (aOR = 0.37; 95% CI, 0.18-0.73). Having private health insurance increased the odds of receiving SUD treatment compared with having no health insurance among men (aOR = 2.05; 95% CI, 1.31-3.20) but not women (aOR = 1.70; 95% CI, 0.97-2.99). Men with lower incomes had slightly higher odds of receiving SUD treatment than men with higher incomes (aOR = 1.76; 95% CI, 1.12-2.76); we did not find this difference among women. Lastly, parenting women had higher odds of receiving treatment than nonparenting women (aOR = 1.97; 95% CI, 1.26-3.08).
Gender-stratified sociodemographic factors associated with substance use disorder (SUD) treatment receipt among adults with SUD, National Survey on Drug Use and Health, 2015-2018 a
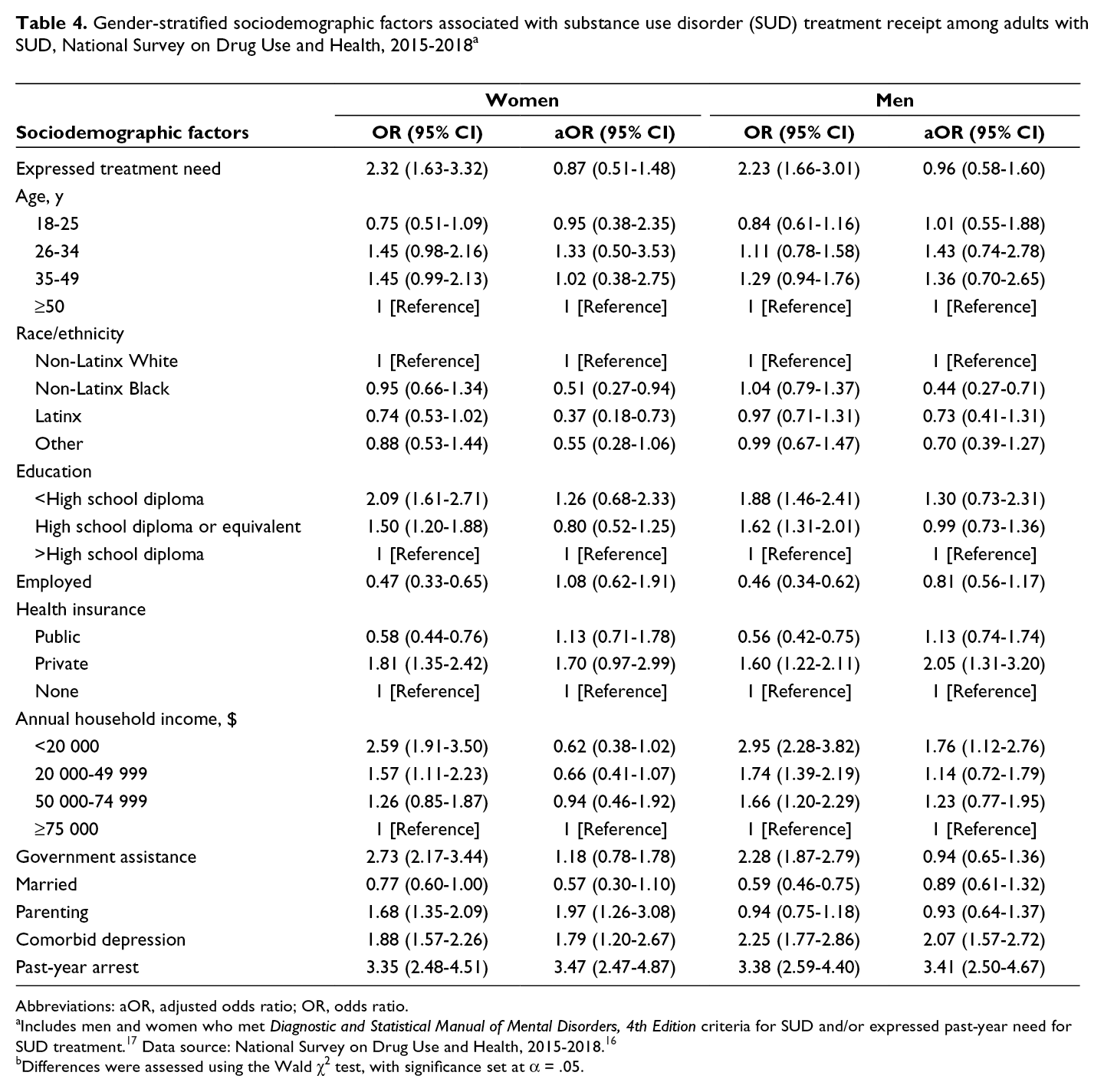
Abbreviations: aOR, adjusted odds ratio; OR, odds ratio.
aIncludes men and women who met Diagnostic and Statistical Manual of Mental Disorders, 4th Edition criteria for SUD and/or expressed past-year need for SUD treatment. 17 Data source: National Survey on Drug Use and Health, 2015-2018. 16
bDifferences were assessed using the Wald χ2 test, with significance set at α = .05.
Most respondents who expressed a need for SUD treatment but did not receive treatment reported ≥1 treatment barrier (91.8%; 95% CI, 88.9%-94.8%); we found no difference by gender (women: 93.9% [95% CI, 89.2%-98.6%]; men: 90.5% [95% CI, 86.6%-94.4%]; P = .33). The most commonly reported barrier among men and women was a negative opinion of treatment (57.9%), followed by financial reasons (37.2%) and the desired treatment being unavailable or at full capacity (26.2%). Women were significantly more likely than men to report transportation and/or time barriers (23.8% vs 9.4%; P < .001) and worry about the effect of treatment on their reputation or job (31.1% vs 17.5%; P = .013). When analyzed by substance type and gender, most of these trends and gender differences persisted. However, among adults with OUD, the most common reason for unmet treatment need was a lack of financial resources (49.5%), followed by a negative opinion of treatment (46.9%).
Discussion
In this nationally representative population, only 1 in 10 men and women with SUD received treatment in the United States. We found important differences between men and women in proportions of SUD treatment need and receipt by substance type. Notably, a larger proportion of women than men with SUD needed treatment for OUD, reflecting evolving patterns in SUD by gender in the current overdose crisis. 4,5 Furthermore, a smaller proportion of women than men received treatment for AUD. Lastly, regardless of gender, the unmet SUD treatment need was significantly higher among non-Latinx Black and Latinx adults than among non-Latinx White adults.
Despite the increasing attention to SUD that has come with the overdose crisis, we found that the unmet SUD treatment need is high among both men and women, a finding that is consistent with previous research. 11,12,20 Reasons for this public health concern are multiple and stem from individual, societal, and systemic factors. 21 Across gender, we found that expressing a need for SUD treatment was not associated with receipt of SUD treatment when we adjusted for sociodemographic variables in our multivariate analysis. These findings highlight low levels of receipt of SUD treatment despite personal desire or motivation for treatment. Improvements in health care provider SUD screening and assessment of readiness to change substance use behavior alone are insufficient to increase SUD treatment use. We need to expand interventions beyond targeting low levels of problem recognition and instead prioritize use of a multidimensional approach, such as one that includes closing the gap in SUD treatment capacity via expansion of reimbursement policies for evidence-based SUD treatment. 22
Our study highlights an important gender difference in the current overdose crisis: among adults with SUD, a larger proportion of women than men need treatment for OUD. Although more men than women in the general population have OUD, 23 our study found that more women than men compose the population of people needing SUD treatment. Overall, these findings mirror epidemiologic data highlighting the changing gender composition of people with OUD. During the past decade, drug-related deaths have increased more rapidly among women than men. 5 Although recent data suggest that the prevalence of OUD and its negative consequences may be increasing among women, a recent study using national data on SUD treatment admissions found that women had slightly higher odds of receiving medication for OUD than men. 24 Historically, services tailored to women (eg, women’s recovery groups, child care) have generally been considered beneficial but not necessary, leading to their underuse in OUD treatment settings. 25 The higher proportion of OUD among women compared with men with a need for SUD treatment further supports previous evidence, 6,13 endorsing the need for universal adoption of gender-informed treatment for people with OUD.
Alcohol is the most common SUD. Although we did not find a difference by gender in the proportion of people with AUD among people with SUD, we did find a difference in receipt of treatment. A smaller percentage of women than men received needed treatment for AUD. This observation supports previous work detailing the narrowing of the gender gap in AUD 5 and highlights a persistent gender disparity in receipt of treatment for AUD. More work is needed to improve access to gender-informed treatment services for AUD, 19 particularly among reproductive-age women considering the teratogenic effects of alcohol. In addition, the postpartum period is associated with a higher risk of opioid overdose, a risk that may be increased in women with AUD after childbirth. 26
Although we did not find a significant difference by gender in overall receipt of SUD treatment, we did identify racial and ethnic inequities in unmet SUD treatment need. Latinx women and non-Latinx Black men and women were significantly less likely than non-Latinx White adults to receive SUD treatment. These findings confirm previous studies highlighting disparities in receipt of SUD treatment among people of color. 11 Non-Latinx Black and Latinx people with SUD have lower odds of initiating SUD treatment despite presenting with greater addiction severity, largely because of structural racism. 27,28 Systemic discriminatory practices affecting income, education, employment, housing, health care, and criminal justice systems limit opportunities for people of color to engage in high-quality treatment services. 29 -31 In addition, the stigma associated with SUD and SUD treatment is prevalent among many communities of color. Similar to previous work, our research found Latinx women to be the least likely to receive needed SUD treatment, likely reflecting the unique stigma this population faces because of cultural norms. 32 In line with the American Society for Addiction Medicine’s statement on racial injustice, future efforts to address health disparities need to prioritize addressing racial and ethnic inequities among people with SUD. 33 Partnering with the affected communities to develop community-driven, multilevel interventions and use harm reduction approaches are possible ways to begin to combat the systemic barriers that disproportionately affect these communities. 34,35
Consistent with previous studies, our study found that among men and women with an expressed need for SUD treatment, the most common barriers to care were attitudinal (ie, having a negative opinion about treatment). 29 Furthermore, women were more likely than men to report concern about the effect of treatment on their reputation or job. A large driver of these findings can be explained by the stigma of SUD and SUD treatment that is pervasive in communities, including in health care and legal settings. 36 Unfortunately, women are particularly susceptible to SUD-associated stigma and discrimination because social norms are less accepting of SUD among women than men. 10 Future efforts to close the national unmet SUD treatment gap and its gender disparities will be minimally effective if these efforts do not include components designed to lessen or eliminate stigma and discrimination. 36 Promisingly, when stratified by substance type, a slightly smaller percentage of adults with an expressed need for OUD treatment, compared with people with other SUDs, reported a negative opinion of treatment as a barrier. This finding may highlight emerging positive effects of recent public health and policy strategies to decrease stigma associated with medications for OUD. 1
Limitations
This study had several limitations. First, although NSDUH is considered the gold standard for reporting data on substance use, SUD, and SUD treatment receipt for the United States, it is not comprehensive because it excludes certain populations, such as people who are incarcerated, institutionalized, or experiencing homelessness. Second, NSDUH data are self-reported, which can lead to misclassification bias. Third, data on SUD treatment need and receipt could be underreported unevenly across groups, leading to differential misclassification in our results. Fourth, NSDUH does not assess sex and gender as separate variables and does not include a comprehensive definition of gender. Thus, we were not able to evaluate their different effects or perform analysis among transgender and gender-nonconforming adults, who are at additional risk for SUD and unmet SUD treatment need because of gender identity–based discrimination. 37 Fifth, our outcome of SUD treatment receipt was calculated from binary items on location of treatment; treatment length of time and type (eg, behavioral, medication) were not assessed, precluding our ability to evaluate SUD treatment outcomes by treatment settings. Therefore, treatment receipt in our study does not reflect receipt of ongoing SUD care, likely leading to an underestimation of receipt of the recommended standard of care for SUD treatment that exists in a chronic disease model. 38 Lastly, because data were cross-sectional, we were not able to assess the potential causality of factors related to unmet treatment need.
Conclusions
Despite the increased attention to SUD treatment that has come with the opioid crisis, large disparities in receipt of SUD treatment exist nationwide. SUD treatment receipt is unacceptably low for men, for women, and, in particular, for people of color. Inequities in SUD treatment receipt may relate to recent data that demonstrate that rates of overdose death are increasing most rapidly among women and people of color. 5 As public health efforts target expanding SUD treatment capacity and addressing disparities in SUD treatment use, interventions informed by gender and culture should be prioritized.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Anna Beth Parlier-Ahmad reports receiving National Institute on Drug Abuse (NIDA) award #T32DA007027 (principal investigator: William Dewey). Caitlin E. Martin is supported by award #K23 DA053507 from NIDA and partially by KL2TR002648 from the National Center for Advancing Translational Sciences.