
Abstract
Objective
Pregnant women are at increased risk of serious complications from influenza and are recommended to receive an influenza vaccination during pregnancy. The objective of this study was to assess trends, timing patterns, and associated factors of influenza vaccination among pregnant women.
Methods
We used 2010-2018 MarketScan data on 1 286 749 pregnant women aged 15-49 who were privately insured to examine trends and timing patterns of influenza vaccination coverage. We examined descriptive statistics and identified factors associated with vaccination uptake by using multivariate log-binomial and Cox proportional hazard models.
Results
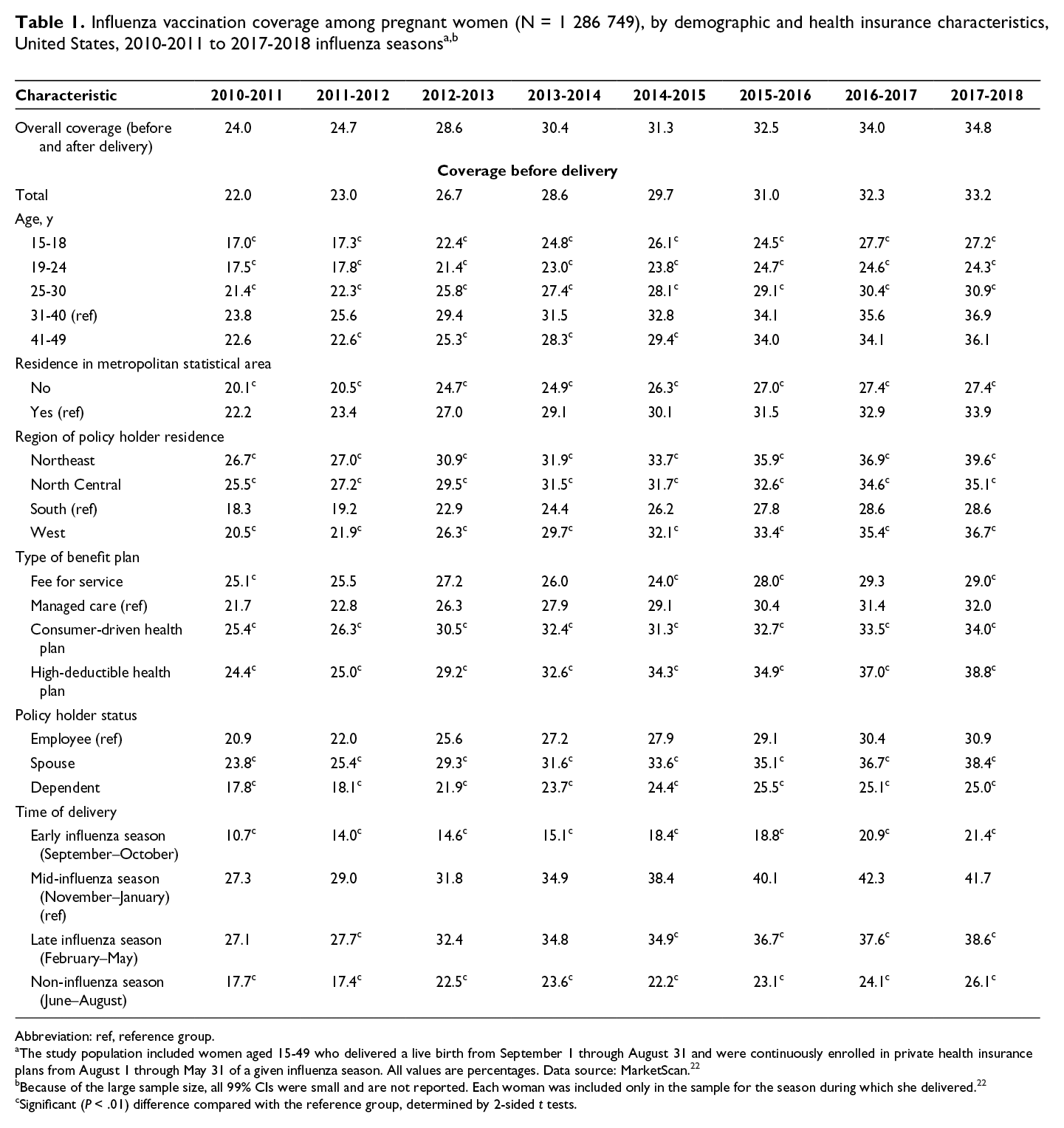
In-plan influenza vaccination coverage before delivery increased from 22.0% during the 2010-2011 influenza season to 33.2% during the 2017-2018 influenza season. About two-thirds of vaccinated women received the vaccine in September or October during each influenza season. For women who delivered in September through May, influenza vaccination coverage increased rapidly at the beginning of influenza season and flattened after October. For women who delivered in June through August, influenza vaccination coverage increased gradually until February and flattened thereafter. Most vaccinated women who delivered before January received the vaccine in the third trimester. Increased likelihood of being vaccinated was associated with age 31-40, living in a metropolitan statistical area, living outside the South, enrollment in a consumer-driven or high-deductible health plan, being spouses or dependents of policy holders, and delivery in November through January.
Conclusions
Despite increases during the past several years, vaccination uptake is still suboptimal, particularly after October. Health care provider education on timing of vaccination and recommendations throughout influenza seasons are needed to improve influenza vaccination coverage among pregnant women.
Influenza infection during pregnancy is an important factor in morbidity and mortality of pregnant women and newborn infants. 1,2 In the United States, pregnant women are at higher risk for hospitalization associated with laboratory-confirmed influenza virus infection than nonpregnant women are. 3,4 Children aged <6 months, who are too young to be vaccinated, have the highest influenza mortality risk among all children. 5
Substantial evidence from randomized controlled trials and large retrospective population-based cohort studies shows that influenza vaccination can protect pregnant women and their infants against influenza-associated disease. 1,6 The Advisory Committee on Immunization Practices (ACIP) recommends that all women who are or will be pregnant during the influenza season receive an influenza vaccination during any trimester of pregnancy. 7 Annual internet panel surveys show that overall influenza vaccination coverage among pregnant women in the United States has been flat at 40%-50% since the 2010-2011 influenza season. 8,9 Previously identified determinants of influenza vaccination coverage include health care provider recommendation for vaccination, perceived severity of influenza infection, concerns about vaccine safety, and demographic characteristics such as age, race/ethnicity, and education. 2,8
For the general population, ACIP recommends that influenza vaccination should be received by the end of October and should continue to be offered as long as influenza viruses are still circulating. 7 ACIP recommendations for the vaccination of pregnant women do not specify an optimal time (calendar or gestational) for vaccination. 1,7,10 The literature, mainly on influenza vaccine immunogenicity during pregnancy, shows mixed evidence on the optimal time for influenza vaccination among pregnant women. 1,11 -20 Timing patterns of prenatal influenza vaccination in practice, especially how prenatal influenza vaccination varies by calendar month and whether pregnant women are complying with the ACIP recommendation for the general population, have not been fully characterized because the quality of existing data is insufficient. 1
On top of yearly trends of coverage and selected factors associated with the likelihood of vaccination that were explored in a recent study, 21 the primary objective of this study was to assess timing (calendar month and trimester) of influenza vaccination for privately insured women vaccinated during pregnancy, by month of delivery (used throughout to indicate childbirth rather than vaccine delivery).
Methods
We used the MarketScan 2010-2018 Commercial Claims and Encounters databases to assess influenza vaccination coverage of pregnant women during the 2010-2011 through 2017-2018 influenza seasons. MarketScan data, one of the largest private health insurance claims data sets in the United States, has included about 255 million enrollees since 1995 and about 40 million enrollees annually in recent years, from more than 160 contributing employers in the private sector and 40 contributing health insurance plans. 22 The Commercial Claims and Encounters database includes data on health insurance; encounter information such as service date, diagnostic codes, and procedure codes; and demographic characteristics, such as age and sex.
We analyzed data on all women aged 15-49 who delivered a live birth from September 1 through August 31 and were continuously enrolled in private health insurance plans from August 1 through May 31 of a given influenza season. We included data from the 2010-2011 through 2017-2018 influenza seasons. We included each woman only in the sample for the season during which she delivered, because we intentionally examined vaccination that was targeted to provide protection for mothers and infants against influenza viruses circulating at the time of delivery.
We grouped women by age (15-18, 19-24, 25-30, 31-40, 41-49), residence in a metropolitan statistical area (yes/no), region (Northeast, North Central, South, West), type of health insurance plan (fee-for-service plan, managed care plan, consumer-driven health plan, high-deductible health plan), health insurance policy holder status (employee, spouse, dependent), time of delivery (early influenza season [September–October], mid-influenza season [November–January], late influenza season [February–May], and non-influenza season [June–August]), and, for vaccinated women, influenza vaccination provider type (obstetrics/gynecology, family practice, medical doctor [not elsewhere classified], multispecialty physician, other).
We identified women with a live birth by using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) 23 and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) 24 codes: 650, V27.0, V27.2, V27.3, V27.5, V27.6, O80, Z370, Z372, Z373, Z375, Z376, and Z379. 25,26 We identified influenza vaccination by using Current Procedural Terminology codes 27 and Healthcare Common Procedure Coding System codes 28 from either inpatient or outpatient service claims files. 29 We examined the timing of influenza vaccination by calendar month of the vaccination claim, before pregnancy, during pregnancy, and after delivery (extending through the end of the influenza season) and by trimester, defined as first trimester (0-13 weeks’ gestation), second trimester (14-26 weeks’ gestation), and third trimester (27-40 weeks’ gestation). Because no information on gestational age was available in the data, following the literature, we approximated the beginning of pregnancy as 40 weeks before the delivery date. 26 We conducted sensitivity analyses, including examining influenza vaccination among a subsample that was restricted to full-term deliveries (identified by ICD-9-CM code 650 or ICD-10-CM code O80) and adopting alternative gestational ages at birth, assuming pregnancy began 37, 38, 39, and 41 weeks before the delivery date.
We used SAS version 9.4 (SAS Institute, Inc) to conduct statistical analyses. We used frequencies and descriptive statistics to describe the study population and calculate influenza vaccination uptake, cumulative coverage, and vaccination timing during each influenza season, for the total sample and for subpopulations by women’s characteristics. We constructed a multivariate log-binomial model and a multivariate Cox proportional hazard model for regression analyses to identify factors independently associated with influenza vaccination uptake and hazard of vaccination (overall and in September or October). We used 2-sided t tests to determine significance, with P < .01 considered significant. As a secondary analysis of de-identified data, this study did not require institutional review board approval.
Results
For each influenza season, 115 272-205 118 pregnant women were included in the study.
Coverage and Timing of Influenza Vaccination Before, During, and After Pregnancy
Overall influenza vaccination coverage, including vaccination before delivery and postpartum, increased from 24.0% (99% CI, 23.8%-24.3%) during the 2010-2011 influenza season to 34.8% (99% CI, 34.5%-35.2%) during the 2017-2018 influenza season (Table 1). During the 2017-2018 influenza season, monthly vaccination coverage for women who delivered in September or October peaked in September, at 10.6% and 21.5%, respectively, and coverage for women who delivered in other months through May peaked in October (range, 13.8%-21.6%) (Figure). For women who delivered from September 2017 through May 2018, the percentage of vaccination (by month of delivery) decreased rapidly after October, from 0.8%-9.7% (mean, 5.3%) in November to 0%-2.5% (monthly means, 0%-1.3%) in January and thereafter. For women who delivered from June through August 2018, the vaccination rate peaked in November (9.8%), December (6.1%), and January (6.3%), respectively. Results for other influenza seasons showed similar patterns. In our sensitivity analysis, during the 2017-2018 influenza season, calendar timing of influenza vaccination among women with full-term deliveries showed a similar pattern.
Abbreviation: ref, reference group.
aThe study population included women aged 15-49 who delivered a live birth from September 1 through August 31 and were continuously enrolled in private health insurance plans from August 1 through May 31 of a given influenza season. All values are percentages. Data source: MarketScan. 22
bBecause of the large sample size, all 99% CIs were small and are not reported. Each woman was included only in the sample for the season during which she delivered. 22
cSignificant (P < .01) difference compared with the reference group, determined by 2-sided t tests.
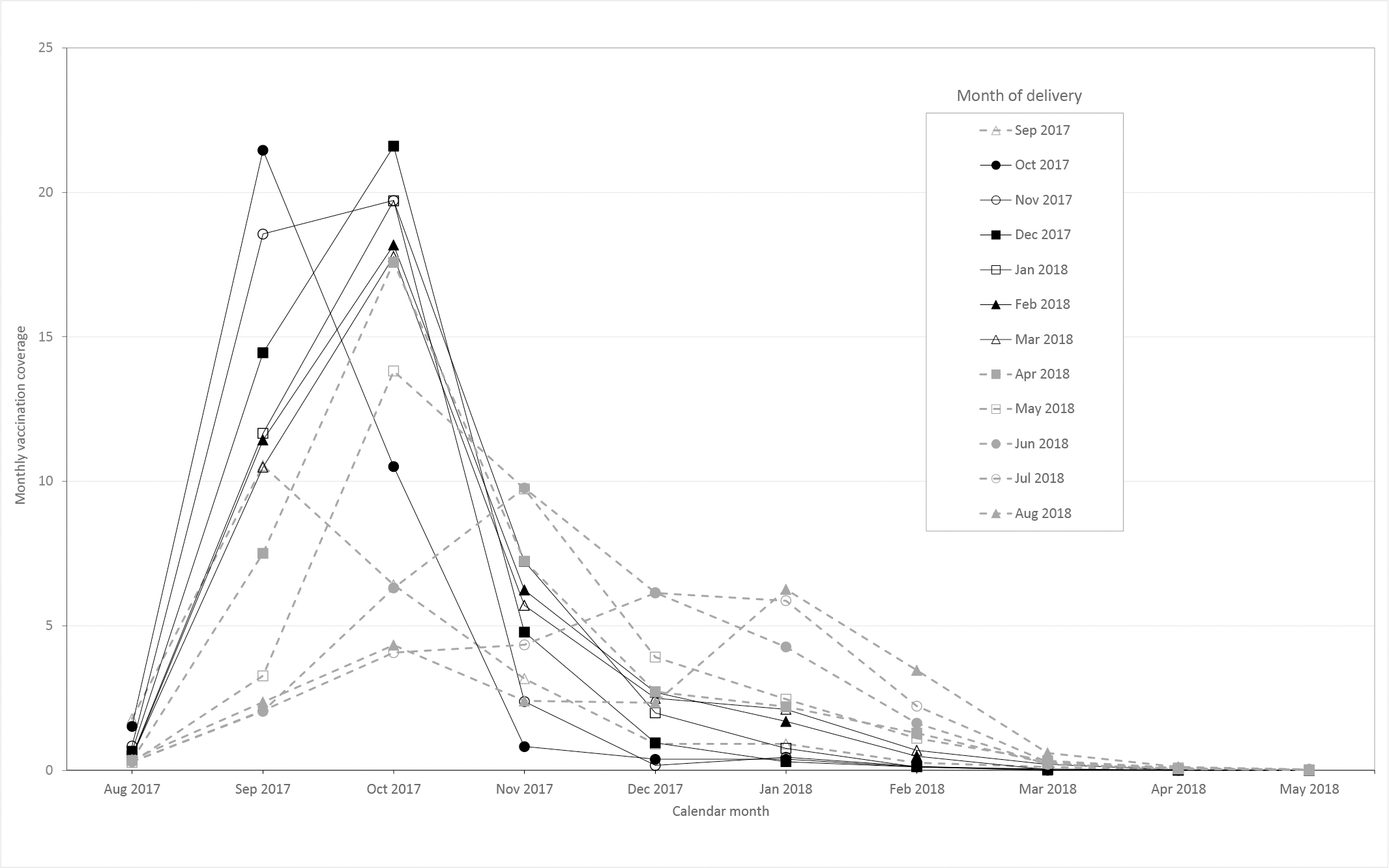
Monthly influenza vaccination coverage among pregnant women, before, during, and after pregnancy, in each month, by month of delivery, United States, 2017-2018 influenza season. The study population included women aged 15-49 who delivered a live birth from September 1 through August 31 and were continuously enrolled in private health insurance plans from August 1 through May 31 of a given influenza season. Data source: MarketScan. 22 Each line represents the percentage of vaccinations by calendar month among pregnant women who delivered in the corresponding month. Percentage of vaccination considers vaccinations received postpartum. Overall postpartum vaccination coverage was 1.6%. Each woman was included only in the sample for the season during which she delivered.
Coverage and Timing of Influenza Vaccination Before and During Pregnancy
Overall influenza vaccination coverage before delivery increased from 22.0% (99% CI, 21.7%-22.2%) during the 2010-2011 influenza season to 33.2% (99% CI, 32.8%-33.5%) during the 2017-2018 influenza season (Table 1), an average annual increase of about 1.6 percentage points (P < .001). During the 2017-2018 influenza season, women who delivered in mid-influenza season had the highest vaccination coverage (41.7%) compared with women who delivered in early influenza season (21.4%), late influenza season (38.6%), and non-influenza season (26.1%). Coverage also varied by other women’s characteristics. All differences in coverage by subpopulations were significant. Despite lower overall coverage, patterns in other earlier influenza seasons were similar for most variables across seasons.
Among women who were vaccinated before delivery during the 2017-2018 influenza season, about two-thirds received the vaccination in September or October, and about 30% received the vaccination in November through January. This pattern of peaking in September or October was stable across all study years and persisted among women who delivered in any month from September through May: the percentage of women receiving the vaccination in September or October ranged from 48.9% (for women who delivered in May) to 95.4% (for women who delivered in October). In contrast, vaccinations among women who delivered from June through August were mainly received in November through January, ranging from 49.4% (for women who delivered in August) to 65.6% (for women who delivered in June). Overall, most (58.0%-65.8%) vaccinated pregnant women received an influenza vaccination from obstetricians/gynecologists in all influenza seasons, followed by family physicians (9.2%-13.4%), medical doctors (not elsewhere specified; 2.1%-8.3%), and multispecialty physicians (2.1%-6.2%). Other types of vaccination providers together accounted for 14.8%-21.3% of vaccinations, with no single type of provider accounting for more than 4% of vaccinations.
During the 2017-2018 influenza season, regardless of delivery month, cumulative influenza vaccination coverage before delivery increased from September to October. For pregnant women who delivered from November through May, vaccination coverage increased at slower rates in November and December and flattened thereafter. For pregnant women who delivered from June through August, coverage increased until February and flattened through the end of the season. The final cumulative coverage of influenza vaccination before delivery ranged from 10.3% (for women who delivered in September) to 42.2% (for women who delivered in December). Results for other influenza seasons showed similar patterns.
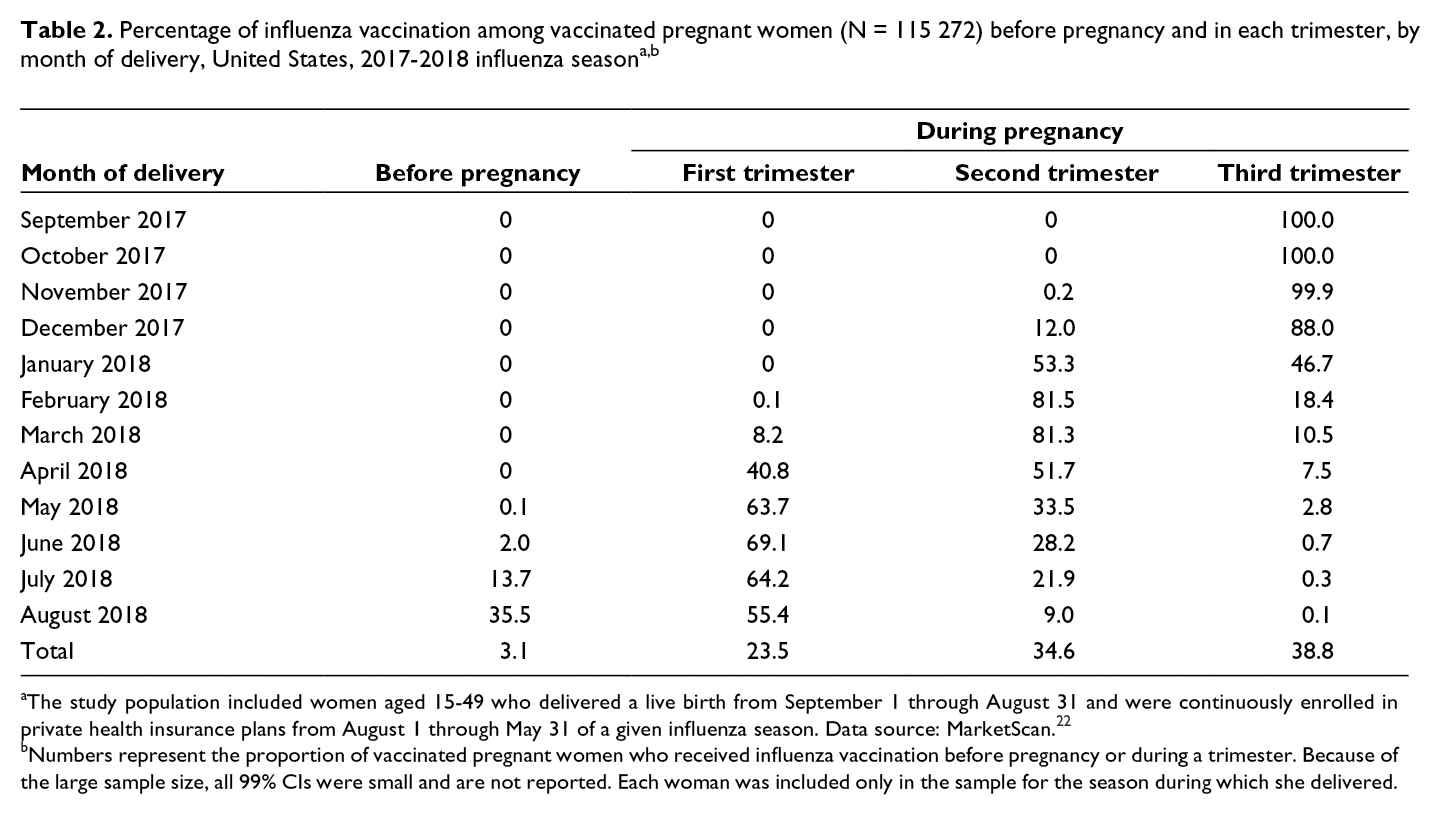
The peak trimester of vaccination uptake differed by month of delivery. During the 2017-2018 influenza season, among vaccinated women who delivered in September through December, ≥88.0% received vaccination in the third trimester, and the remainder received vaccination in the second trimester. More than half of vaccinated women who delivered from January through April received vaccination in the second trimester. Vaccinated women who delivered from May through August primarily received vaccination in the first trimester, with about 3% of vaccinations received before pregnancy (Table 2). Patterns for other influenza seasons were similar.
aThe study population included women aged 15-49 who delivered a live birth from September 1 through August 31 and were continuously enrolled in private health insurance plans from August 1 through May 31 of a given influenza season. Data source: MarketScan. 22
bNumbers represent the proportion of vaccinated pregnant women who received influenza vaccination before pregnancy or during a trimester. Because of the large sample size, all 99% CIs were small and are not reported. Each woman was included only in the sample for the season during which she delivered.
In sensitivity analyses estimating alternative gestational ages at birth, during the 2017-2018 influenza season, the overall proportions of women who were vaccinated before pregnancy and during each trimester were unchanged, for both the main sample and the subsample of full-term deliveries. Compared with our main duration of 40 weeks’ gestation, a longer duration of pregnancy resulted in similar or lower vaccination rates before pregnancy and during the first trimester, shifting the observed vaccinations to the second and third trimesters.
Factors Associated With Coverage and Likelihood of Influenza Vaccination Before and During Pregnancy
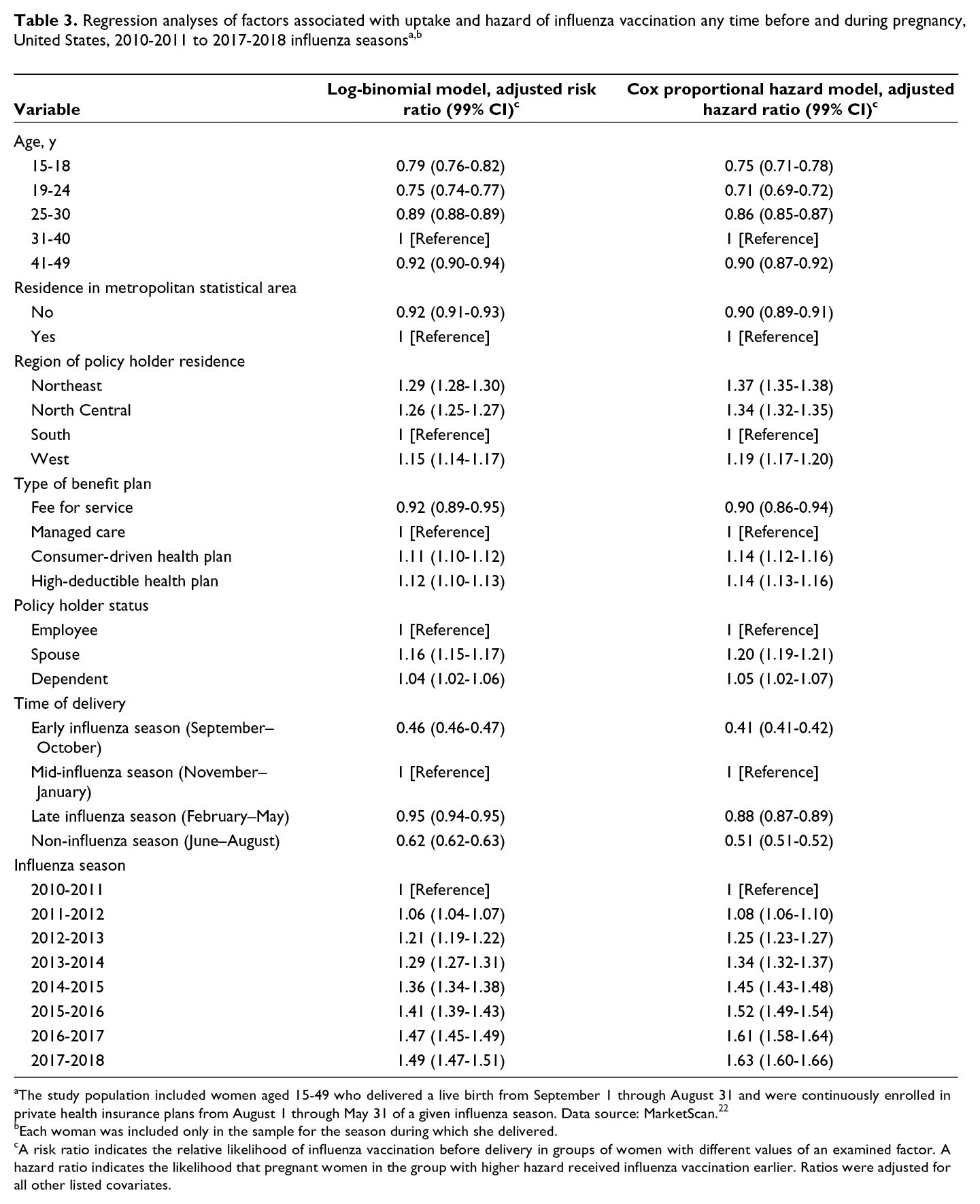
Pooling all the study influenza seasons, increased coverage and likelihood (hazard) of vaccination before and during pregnancy at any time during the influenza season were associated with age 31-40, enrollment in a consumer-driven health plan or a high-deductible health plan, and being spouses or dependents of the primary policy holders, after adjusting for other factors in multivariable analysis (Table 3). Conversely, decreased coverage and likelihood (hazard) of vaccination before and during pregnancy were associated with age 19-24, not living in a metropolitan statistical area, living in the South, enrollment in a fee-for-service plan, or delivery in months other than November through January. Findings were similar for vaccination in September or October.
aThe study population included women aged 15-49 who delivered a live birth from September 1 through August 31 and were continuously enrolled in private health insurance plans from August 1 through May 31 of a given influenza season. Data source: MarketScan. 22
bEach woman was included only in the sample for the season during which she delivered.
cA risk ratio indicates the relative likelihood of influenza vaccination before delivery in groups of women with different values of an examined factor. A hazard ratio indicates the likelihood that pregnant women in the group with higher hazard received influenza vaccination earlier. Ratios were adjusted for all other listed covariates.
Discussion
Influenza vaccination coverage during pregnancy increased from the 2010-2011 influenza season to the 2017-2018 influenza season among privately insured women. However, despite ACIP’s influenza vaccination recommendation, vaccination coverage among pregnant women in our sample was inadequate.
Our findings on trends in overall coverage among privately insured women were similar to the findings of a recent study using similar data, 21 with the period of observation extended through the 2017-2018 influenza season. Part of the reason for the increasing trends in vaccination coverage during our study period, overall and in almost all sociodemographic subgroups examined, could be the Affordable Care Act. Enacted in 2010, the Affordable Care Act reduced financial barriers to routine adult vaccination and is associated with improved receipt of influenza vaccination among women. 30 Vaccination coverage in our study was consistently lower than vaccination coverage in a previous study that reported a flat trend in coverage from the 2010-2011 to 2016-2017 influenza season using survey data. 8 The discrepancy is likely the result of differences in methodologies: our estimates did not include vaccinations received outside health insurance plans, whereas survey data may overestimate true coverage because of issues such as social desirability bias and recall bias. 8,9,31 In addition to corroborating previous literature focused on yearly trends of vaccination coverage and factors associated with the likelihood of vaccination, 8,21 our study examined timing (calendar month and trimester) of influenza vaccination for privately insured women to highlight the disparity in vaccine uptake by calendar month among pregnant women who deliver at different times during or outside an influenza season.
Although our findings seem intuitive, this study is the first to our knowledge to quantify timing patterns of influenza vaccination among pregnant women using claims data, which may help inform strategies to increase influenza vaccination coverage among pregnant women in clinical practice. The roughly similar patterns of vaccination timing for women who delivered from September through May indicate that, in practice, influenza vaccination for pregnant women was administered as soon as the vaccine became available, mainly early during the influenza season. These findings are consistent with ACIP’s recommendation to administer influenza vaccination anytime during pregnancy, optimally by the end of October (for the general population). Obstetricians/gynecologists report consistent support for influenza vaccination during any trimester: a recent survey of obstetricians/gynecologists found that few physicians reported altering their recommendations for influenza vaccination of pregnant patients 32 in response to publication of a study suggesting safety concerns related to first-trimester vaccination in some circumstances 33 (a later definitive study found no association). 34 Overall, researchers have established that influenza vaccination is safe at any point during pregnancy. 1
The overall timing patterns of influenza vaccination among pregnant women in our study are similar to timing patterns of influenza vaccination among nonpregnant women of the same age in our sample and the general US population. 35 Given the ACIP recommendation that people should get vaccinated by October and, if not, should continue to be vaccinated as long as influenza viruses are circulating, 7 our findings indicate that influenza uptake after October is suboptimal, particularly given that 75% of US influenza seasons from the 1982-1983 season to the 2017-2018 season had peak influenza activity in January or later. 7,36 Having private health insurance (and presumably access to vaccination services) may not be the only factor influencing receipt of vaccination. Because, overall, about 60% of vaccinated women in our study received influenza vaccination from obstetricians/gynecologists, but that percentage was smaller for vaccinations received after October, our data suggest substantial missed opportunities for influenza vaccinations during routine obstetric/gynecologic visits for women who delivered after October. Compared with nonpregnant women of reproductive age, pregnant women are at increased risk of influenza hospitalization. 37 -39 Thus, health care providers should make efforts to ensure that this population receives the influenza vaccination throughout the entirety of the season.
The timing patterns for women who delivered from June through August indicate that in practice, those women may not consider getting vaccinated until they become aware of their pregnancy, leading to low vaccination uptake in September and October and during the entire season as compared with women who delivered from September through May. ACIP recommendations emphasize that women who might be pregnant during influenza season should also receive the influenza vaccine. 7 When being consulted about a birth plan, obstetricians/gynecologists and other health care providers should emphasize the importance of influenza vaccination to protect the health of potential mothers and neonates and that influenza vaccination can be safely administered anytime during pregnancy.
Time of delivery was associated with influenza vaccination uptake, anytime or by the end of October, during the study period. Women who delivered in September or October, or after January, were less likely to receive influenza vaccination than women who delivered in November through January. Women who delivered in early influenza season might not have sufficient access to the vaccine before delivery, because the influenza vaccine generally begins reaching health care provider offices in mid-September. Women who delivered during the late influenza season and non-influenza season were still at early gestational age or were not yet pregnant in September or October, when influenza vaccination uptake rates peaked. Consequently, during that time, they likely had fewer routine health care provider visits than women who were close to delivery and, thus, fewer opportunities for vaccination. However, these women would have had many subsequent health care provider visits during the influenza season, highlighting missed opportunities for vaccine administration. During the current COVID-19 pandemic, it is particularly important for health care providers to administer recommended vaccines, likely including COVID-19 vaccines, during routine health care provider visits for pregnant women, who might be at increased risk for severe COVID-19 illness. 40
Limitations
Our study had several limitations. First, our study data were from private health insurance claims on a segment of the population reported for reimbursement purposes and, thus, might not be representative of the US general population. Pregnant women with public health insurance might have different vaccination coverage or behaviors than pregnant women with private health insurance; however, research suggests our data are acceptably representative of the privately insured population of pregnant women in the United States. 26 Second, we excluded pregnant women who did not deliver a live birth or were not continuously enrolled in private health insurance plans from August through May during each influenza season. The excluded population of pregnant women might differ from our study sample. Third, influenza vaccination coverage might be underestimated if not all claims were successfully reported and reimbursed or if some pregnant women received vaccination outside their health insurance plans. However, survey data indicate that most vaccinated pregnant women (>80%) received influenza vaccination in obstetrician/gynecologist offices or other medical-related places, 31 which should be captured in these data. Finally, our main study sample included preterm and full-term deliveries, and the beginning of pregnancy was approximated as 40 weeks before the delivery date. Because 90% of births occurred between 37 and 41 weeks’ gestational age from 2010 to 2017, 41,42 previous research and our sensitivity analyses suggest that our results were unlikely to be driven by using 40 weeks from recorded delivery date to approximate the beginning of pregnancy. 26
Conclusion
Despite increases in influenza vaccination uptake among pregnant women during the past several years, coverage remains suboptimal, particularly after October. To improve influenza vaccination coverage among pregnant women, intervention strategies such as health care provider education on timing of influenza vaccination and recommendations throughout influenza seasons are needed, 43 before and during pregnancy, particularly for women who are aged ≤24, live outside a metropolitan statistical area, live in the South, are enrolled in a fee-for-service plan, are primary policy holders, or deliver early in the influenza season, during the late influenza season, or outside the influenza season. Given the substantial share of vaccinations administered by prenatal care providers, it is important to have obstetricians/gynecologists and other health care providers—including but not limited to family physicians, internists, nurses, and nurse–midwives—improve rates of influenza vaccination (and other recommended vaccinations) among pregnant women by strongly recommending and administering influenza vaccination or referring pregnant women to other vaccination providers when vaccination cannot be provided on site. 44
Footnotes
Supplementary Material
Supplementary material that includes all results with additional tables and figures is available from the authors upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.