
Abstract
Racial/ethnic minority groups are disproportionately affected by the COVID-19 pandemic. We examined ethnic differences in SARS-CoV-2 testing patterns and positivity rates in a large health care system in Northern California. The study population included patients tested for SARS-CoV-2 from March 4, 2020, through January 12, 2021, at Stanford Health Care. We used adjusted hierarchical logistic regression models to identify factors associated with receiving a positive test result. During the study period, 282 916 SARS-CoV-2 tests were administered to 179 032 unique patients, 32 766 (18.3%) of whom were Hispanic. Hispanic patients were 3 times more likely to receive a positive test result than patients in other racial/ethnic groups (odds ratio = 3.16; 95% CI, 3.00-3.32). The rate of receiving a positive test result for SARS-CoV-2 among Hispanic patients increased from 5.4% in mid-March to 15.7% in mid-July, decreased to 3.9% in mid-October, and increased to 21.2% toward the end of December. Hispanic patients were more likely than non-Hispanic patients to receive a positive test result for SARS-CoV-2, with increasing trends during regional surges. The disproportionate and growing overrepresentation of Hispanic people receiving a positive test result for SARS-CoV-2 demonstrates the need to focus public health prevention efforts on these communities.
The COVID-19 pandemic has magnified longstanding racial/ethnic inequities in the United States. Hispanic and Black people have a disproportionately higher prevalence of COVID-19 risk factors (eg, multiple comorbidities) and are more susceptible to serious complications than non-Hispanic White people. 1 -4 These populations also face social and economic circumstances, such as shared living spaces and reliance on public transportation, that can increase their likelihood of contracting SARS-CoV-2, the virus that causes COVID-19, and that make it difficult to obtain timely access to tests and to self-isolate if they receive a positive test result. 5
In Northern California, Hispanic people compose more than one-third of the population and are overrepresented in the essential workforce. 6,7 Stanford Health Care (SHC) services the Northern California area through primary and specialty care; an estimated 13% of the population it serves are Hispanic. However, it is unknown if this population also has a disproportionately high prevalence of COVID-19 and how these trends are changing over time. We investigated trends in COVID-19 testing practices and positivity rates, as well as differences in testing characteristics, among Hispanic and non-Hispanic patients at SHC.
Methods
Data Source
We collected data for this study from a tertiary-care academic medical center with an Epic electronic health record (EHR) system (Epic Systems Corporation) and managed in an EHR-based relational database. The Stanford University Institutional Review Board approved this study.
Study Cohort
We identified patients who had reverse transcription–polymerase chain reaction (RT-PCR) tests for SARS-CoV-2 at SHC in the EHR from March 4, 2020, through January 12, 2021. We extracted self-reported data on race/ethnicity (Hispanic, non-Hispanic Black, non-Hispanic Asian, non-Hispanic White, and “other” [American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander] or missing). We excluded patients whose data on ethnicity were missing or not provided.
Statistical Analyses
We compared test differences between Hispanic and non-Hispanic patients in demographic characteristics (age, sex [male or female], and primary health insurance payer [private, Medicare, Medicaid, or other]) and testing characteristics (percentage of patients with a positive test result, number of tests per patient, whether an antibody test was received, and test site [outpatient, emergency department, or inpatient setting]). We evaluated bivariate analyses using the Pearson χ2 and t tests. We calculated test positivity by using a 7-day rolling average to better identify trends. We developed a multivariate logistic regression, specifying patient as a random effect, to examine the likelihood of receiving a positive test result for SARS-CoV-2 in relation to patient factors—including ethnicity, age, sex, and primary health insurance—and testing week. All statistical tests were 2-sided, with significance set at P ≤ .05.
Results
During the study period, 282 916 SARS-CoV-2 RT-PCR tests were administered to 169 998 unique patients (mean, 1.7 tests per patient) for whom ethnicity was reported (Table). Of these, 31 655 (18.6%) patients self-identified as Hispanic. Compared with non-Hispanic patients, Hispanic patients were significantly younger at the time of SARS-CoV-2 testing (mean age [SD], 38.5 [20.4] vs 48.4 [21.2]; P < .001), and a higher proportion were female (56.8% vs 55.2%) and had Medicaid insurance (33.1% vs 7.1%) (P < .001 for both). Compared with non-Hispanic patients, Hispanic patients were more likely to be tested for SARS-CoV-2 in the emergency department (23.6% vs 11.5%) and the inpatient setting (3.9% vs 2.1%) and less likely to receive an antibody test (3.5% vs 5.7%).
Characteristics of patients tested for COVID-19 (N = 169 998) and testing characteristics (N = 282 916), stratified by Hispanic ethnicity, March 4, 2020, through January 12, 2021, Stanford Health Care, Stanford, California a
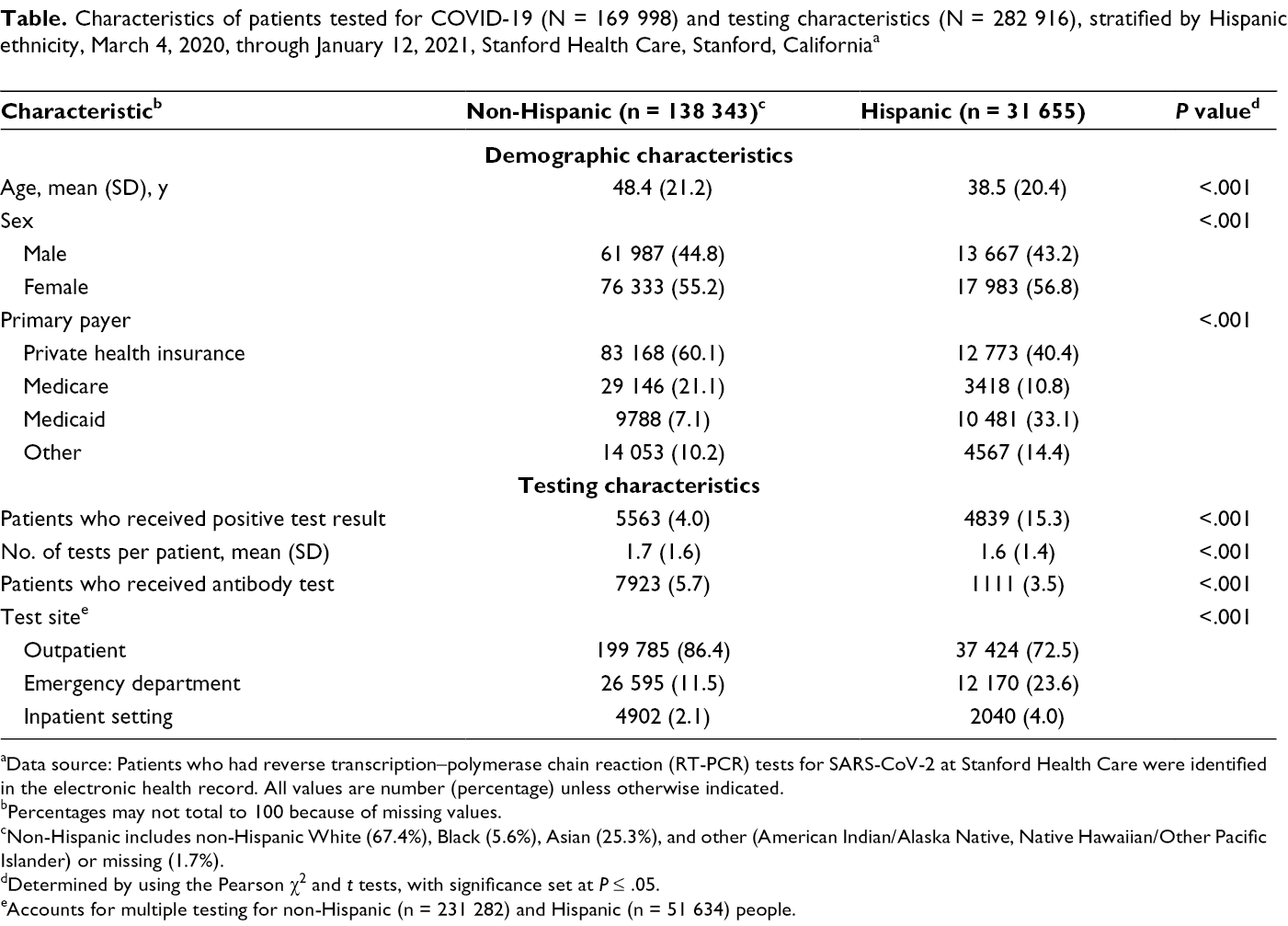
aData source: Patients who had reverse transcription–polymerase chain reaction (RT-PCR) tests for SARS-CoV-2 at Stanford Health Care were identified in the electronic health record. All values are number (percentage) unless otherwise indicated.
bPercentages may not total to 100 because of missing values.
cNon-Hispanic includes non-Hispanic White (67.4%), Black (5.6%), Asian (25.3%), and other (American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander) or missing (1.7%).
dDetermined by using the Pearson χ2 and t tests, with significance set at P ≤ .05.
eAccounts for multiple testing for non-Hispanic (n = 231 282) and Hispanic (n = 51 634) people.
Hispanic patients had higher rates of SARS-CoV-2 test positivity than non-Hispanic patients (15.3% vs 4.2%; P < .001) (Table). Test positivity for SARS-CoV-2 increased from 5.4% in mid-March to 15.7% in mid-July among Hispanic patients but declined among non-Hispanic patients (6.4% vs 2.9%) (Figure). Toward the end of December, the test positivity rate was 21.2% among Hispanic patients and 7.8% among non-Hispanic patients.
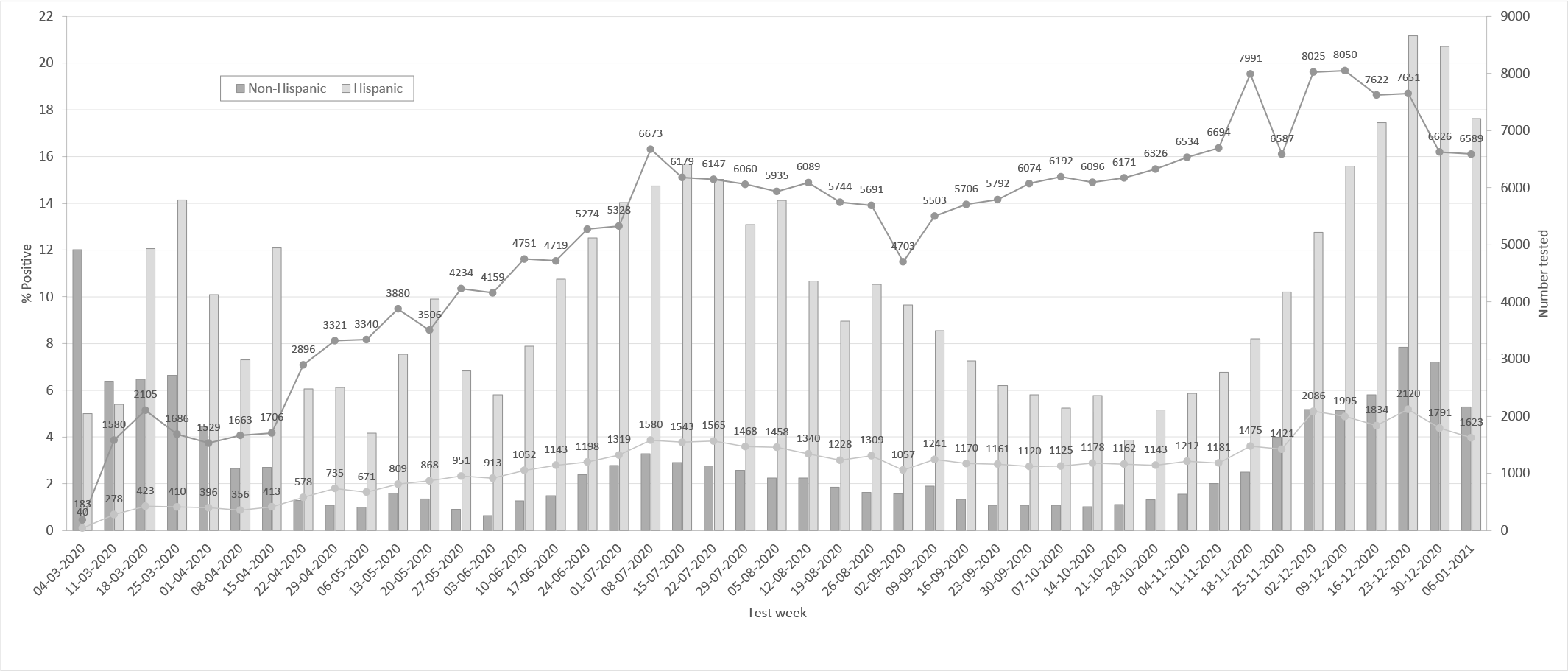
Number of SARS-CoV-2 tests (N = 282 916) and percentage of people who received a positive test result for SARS-CoV-2, by Hispanic ethnicity, March 4, 2020, through January 12, 2021, Stanford Health Care, Stanford, California.
After adjusting for patient demographic characteristics, primary health insurance payer, and testing characteristics, Hispanic patients were almost 3 times more likely than non-Hispanic patients to have a positive test result for SARS-CoV-2 (odds ratio = 3.23; 95% CI, 3.07-3.39).
Discussion
Hispanic people were overrepresented among patients receiving a positive test result for SARS-CoV-2 in a large health care system in Northern California, and their test positivity rates increased during the study period. We found that Hispanic people were almost 3 times more likely than non-Hispanic people to have a positive test result for SARS-CoV-2 during the study period. In addition, Hispanic people were on average 10 years younger, were more likely to be tested in the emergency department, and had higher rates of Medicaid coverage than their non-Hispanic counterparts. The disparities in SARS-CoV-2 testing positivity by Hispanic ethnicity increased during regional surges in the summer and late winter months.
Our findings are consistent with and extend the findings of other studies that highlight the higher positivity rate of SARS-CoV-2 among Hispanic people compared with non-Hispanic people. 3,8 Our study adds to the literature by showing temporal changes, with Hispanic patients having higher test positivity rates than patients in other racial/ethnic groups as the COVID-19 pandemic continues.
One possible explanation for our findings is that racial/ethnic minority groups are overrepresented in the essential workforce, which increases their chances of viral exposure and transmission. Another possible explanation is that Hispanic people and others who have been socially and economically marginalized are more likely than non-Hispanic White people to live in multigenerational households, particularly in densely populated urban settings. 9 A study that examined community determinants of COVID-19 infection in Massachusetts found that factors such as the proportion of non–US-born people, mean household size, and overrepresentation in the food service sector were associated with a higher community prevalence of COVID-19 among Hispanic people than among non-Hispanic people. 10 The living situations highlighted make it difficult for people to socially distance or self-isolate in a private room if they receive a positive test result for SARS-CoV-2, as recommended by the Centers for Disease Control and Prevention. 11 It is also likely that underlying comorbidities such as obesity and diabetes among Hispanic people increase not only their risk for receiving a positive test result for SARS-CoV-2 but also the severity of disease.
Finally, limited English proficiency may further contribute to disparities in COVID-19 infections, because public health messaging may not be readily accessible for linguistic minority groups such as Spanish-speaking people. 12 Hispanic patients in our study were more likely than non-Hispanic patients to be hospitalized for COVID-19 and tested in the emergency department. It is noteworthy that Hispanic people were approximately 10 years younger at the time of test positivity than non-Hispanic people. The interaction among age, ethnicity, risk factors, and disease severity warrants further study.
The increasing rates of test positivity among Hispanic people during our study period reflect the changing demographic characteristics of the COVID-19 pandemic. The ability to identify these trends and incorporate this information into model forecasting is essential to ensure accurate predictions that appropriately represent populations disproportionately at risk for SARS-CoV-2 infection. Early models predicting COVID-19 outcomes were mainly developed from non-Hispanic White and Asian patients, reflecting the incidence of disease at the onset of the pandemic. 13 -15 However, newer data highlight the overrepresentation of Hispanic people among patients who receive a positive test result for SARS-CoV-2. Our work underscores this disproportionate incidence of disease and highlights the trend in test positivity among Hispanic patients. As shelter-in-place ordinances relaxed in Northern California, Hispanic people were likely the first people to return to the essential workforce and, thus, had a higher level of exposure to SARS-CoV-2 than non-Hispanic people. 16 The disparity in test positivity rates by Hispanic ethnicity in our study widened during regional surges in the summer and late winter months. Robust public health infrastructure is needed to prevent these trends in transmission, and more epidemiologic studies are necessary to identify effective mitigation strategies.
Strengths and Limitations
Our study had 2 strengths. First, Hispanic people were overrepresented in a large Northern California health system. Second, SHC was an early testing site; therefore, our dataset contains test results from the beginning of the pandemic across the Bay Area community. However, our study also had several limitations. First, our results may not be generalizable to patients who were not tested at SHC sites, particularly because SHC was an early test site in the area. Second, we were not able to account for temporal changes in test availability and practices, such as differentiating between asymptomatic screening and symptomatic testing. However, these trends likely do not differ by race/ethnicity. Third, we did not capture data on clinical characteristics and outcomes of the tested patients because most of them did not receive other care at SHC and were not hospitalized. However, other studies have documented the overrepresentation of Hispanic people in hospitalizations and deaths for COVID-19 across US hospitals. 4 Fourth, approximately 14% of patients with SARS-CoV-2 testing in our study had missing data on race/ethnicity. Still, in a relatively well-insured Hispanic population (41% with private health insurance), disparities by ethnicity were notable and persistent. Our findings likely underrepresent the disparities in test positivity among Hispanic people who are uninsured or who are unable to easily obtain a test for SARS-CoV-2.
Conclusions
The COVID-19 pandemic has amplified disparities in testing and outcomes among racial/ethnic minority groups. Our work highlights trends in test positivity for Hispanic people as the COVID-19 pandemic continues. More work is needed to identify targeted interventions to address the social determinants of health among Hispanic people to reduce the number of COVID-19 infections and ensure emerging predictive modeling represents the population disproportionately at risk of SARS-CoV-2 infection.
Footnotes
Acknowledgments
The authors acknowledge Ms Tina Seto, MS, Stanford Hospital, for her help in extracting data from the electronic health record system at Stanford Health Care.
Ethics approval
The Stanford University Institutional Review Board approved this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: F.R. is funded by a career development award from the National Heart, Lung, and Blood Institute (K01 HL 14460) and the American Heart Association/Robert Wood Johnson Harold Amos Medical Faculty Development Program. This work was funded by Office of Faculty Development and Diversity’s 2020 COVID-19 and Health Disparities Pilot Grants, Stanford University.