
Abstract
Objectives
Among young people, dual use of marijuana and e-cigarette, or vaping, products (EVPs) is linked with using more inhalant substances and other substances, and poorer mental health. To understand antecedents and potential risks of dual use in adults, we analyzed a representative adult population in Utah.
Methods
We used data from the 2018 Utah Behavioral Risk Factor Surveillance System (n = 10 380) and multivariable logistic regression to evaluate differences in sociodemographic characteristics, comorbidities, and risk factors among adults aged ≥18 who reported currently using both EVPs (any substance) and marijuana (any intake mode), compared with a referent group of adults who used either or neither.
Results
Compared with the referent group, adults using EVPs and marijuana had greater odds of being aged 18-29 (adjusted odds ratio [aOR] = 12.44; 95% CI, 6.15-25.14) or 30-39 (aOR = 3.75; 95% CI, 1.73-8.12) versus ≥40, being male (aOR = 3.29; 95% CI, 1.82-5.96) versus female, reporting ≥14 days of poor mental health in previous 30 days (aOR = 2.30; 95% CI, 1.23-4.32) versus <14 days, and reporting asthma (aOR = 2.09; 95% CI, 1.02-4.31), chronic obstructive pulmonary disorder (aOR = 2.94; 95% CI, 1.19-7.93), currently smoking cigarettes (aOR = 4.56; 95% CI, 2.63-7.93), or past-year use of prescribed chronic pain medications (aOR = 2.13; 95% CI, 1.06-4.30), all versus not.
Conclusions
Clinicians and health promotion specialists working with adults using both EVPs and marijuana should assess risk factors and comorbidities that could contribute to dual use or associated outcomes and tailor prevention messaging accordingly.
E-cigarette, or vaping, products (EVPs) were introduced into the US market in 2007. In 2018, the prevalence of EVP use in the previous 30 days was estimated at 3.2% among all US adults, 1 7.6% among young adults (aged 18-24), and nearly 27.5% among high school students. 2 In Utah, the rate of EVP use among students in grades 8, 10, and 12 in 2019 was estimated to be 12.4%, and the rate among adults 5.6%. 3 Although the high rate of EVP use among young adults and adolescents has led to considerable research on underlying drivers, including social influences, advertising, and product characteristics, 4 research on facilitators of adult use is limited. Many adults who use EVPs also use various forms of tetrahydrocannabinol (THC), the primary mind-altering substance contained in marijuana. 5 Dual use of marijuana and EVPs is associated with using inhalant substances and other types of substances among young adults 6 and with adverse mental health outcomes among adolescents. 7 Many adolescents who engage in dual use of marijuana and EVPs regularly use both tobacco and THC-containing products, posing the potential for addiction to 2 substances. 8
From March 2019 through February 2020 in the United States, 2807 hospitalizations and 68 deaths were attributed to EVP-associated lung injury (EVALI). 9 The outbreak was subsequently linked to vitamin E acetate, an additive used in some THC-containing EVPs. 8 In Utah, which recorded the highest EVALI rate nationally during the outbreak, more than 80% of cases were among adults reporting use of THC-containing EVPs, which are illegal for nonmedical use in Utah and, thus, frequently obtained from sources such as family, friends, and online or in-person dealers. 10 People who use THC-containing EVPs may do so because EVP cartridges reduce odor, deliver high concentrations of THC, and are discreet; these users could represent a subset of people using both marijuana and EVPs. 11 -15 Among adults who use any marijuana, an estimated 37% currently use THC-containing EVPs and 61% have ever used them; among adults who use marijuana in an aerosolized form, more than 60% prefer using THC-containing liquids in a cartridge-based EVP to using dry marijuana in a large vaporizer device. 11
Given high rates of adult EVP use in Utah and the harmful health effects associated with dual use of marijuana and EVPs, population-level analysis is needed to understand the correlates and risks of dual use among adults in Utah. We analyzed the sociodemographic characteristics, behavioral risk factors, and comorbidities among adults in Utah who use both EVPs and marijuana to better understand their potential health risks.
Methods
We used data from the 2018 Utah Public Health Indicator Based Information System. 16 This system is based on the Behavioral Risk Factor Surveillance System (BRFSS), which includes correlates of EVP and marijuana use collected during the year before the 2019 EVALI outbreak. BRFSS is an annual health-related landline and mobile telephone survey that collects data from residents of all 50 states, the District of Columbia, and 3 US territories on population characteristics, health-related risk behaviors, chronic health conditions, and use of preventive services. 17 For our analysis, we defined a dual-use group as adults aged ≥18 who reported current use of both EVPs and marijuana based on their responses to 2 questions. The first question was, “Do you now use electronic cigarettes or e-cigarettes every day, some days, or not at all?” Response options were every day, some days, not at all, don’t know/not sure, and refused. We considered an answer of “every day” or “some days” to be current use of e-cigarettes. The second question was, “During the past 30 days, on how many days did you use marijuana?” Response options were number of days (0-30), none, don’t know/not sure, and refused. We categorized any answer of ≥1 day as current use of marijuana.
These questions did not specify the substance used in the e-cigarettes or the mode for intake of THC. We selected a priori sociodemographic characteristics (age and sex), comorbid conditions, and other potential risk factors for use of inhalant substances and the 2019 EVALI outbreak. We did not include race/ethnicity as a covariate because a maximum of 12 degrees of freedom was available for variable selection, 18 and descriptive statistics suggested that dual use was not distributed differently across racial/ethnic groups. Comorbid conditions were current asthma, current chronic obstructive pulmonary disease (COPD), and ≥14 days of poor mental health in the past 30 days (ie, self-assessed stress, depression, or emotional distress). Other potential risk factors were being a current smoker (≥100 cigarettes in lifetime and use on some days or every day) and use of prescribed chronic pain medications in the past year. 16 Given the limited research on predictors of adult EVP use and associations between cigarette smoking and low income among adults in previous research, 19 we also included a 4-category variable for annual household income (≥$75 000, $50 000-$74 999, $25 000-$49 999, <$25 000).
Statistical Analyses
Our analytic sample consisted of 10 380 adults aged ≥18 in Utah in 2018. We compared adults who currently used EVPs some days or every day and used marijuana at least once in the previous 30 days (ie, dual-use group) and adults who used one or neither (referent group). We used a multivariable regression model to estimate the association between dual use and individual characteristics. We calculated adjusted odds ratios (aORs) and 95% CIs. We retained annual household income in the multivariable model, which improved the stability of the model, as indicated by a decrease of more than 60 000 points in the Akaike information criterion score. 18 A sensitivity analysis compared our multivariable results with the results from an alternate model with a referent group of adults who used neither EVPs nor marijuana. We used SAS version 9.4 (SAS Institute, Inc) to perform the regression analysis and SAS-callable SUDAAN version 11.1 (RTI International) to account for the complex survey design and the use of appropriate survey weights. The Centers for Disease Control and Prevention reviewed this activity for human subjects protection and determined it nonresearch for the primary benefit of enhancing public health practice.
Results
Overall, 6.3% (95% CI, 5.7%-7.0%) of adult BRFSS respondents in 2018 reported using marijuana (any intake mode) during the previous 30 days; a similar proportion (6.1%; 95% CI, 5.4%-6.7%) reported currently using EVP products (any substance) on some days or every day, and 89.5% (95% CI, 88.7%-90.3%) reported using neither. A total of 122 adults (1.7%; 95% CI, 1.4%-2.1%) reported dual use of marijuana and EVPs. Adults in the dual-use group reported using marijuana more days per month (median, 15 days; range, 1-30 days) than adults who reported marijuana use only (median, 10 days; range, 1-30 days).
Univariate Analysis
We found several differences between the dual-use group and adults using either marijuana or EVPs or neither of the two (ie, the referent group) in the univariate analysis (Table 1). A greater percentage of adults in the dual-use group than in the referent group were male rather than female (67.8% vs 49.5%; OR = 2.14; 95% CI, 1.37-3.35) and aged 18-29 (66.7% vs 24.2%; OR = 9.73; 95% CI, 5.18-18.23) or 30-39 (17.8% vs 20.7%; OR = 3.02; 95% CI, 1.45-6.30) versus aged ≥40. Compared with the referent group, adults in the dual-use group had higher odds of self-reported annual household incomes of $25 000-$49 999 (33.6% vs 21.8%; OR = 2.11; 95% CI, 1.17-3.80). Comorbid conditions were more common among the dual-use group as compared with the referent group, including asthma (18.1% vs 9.4%; OR = 2.14; 95% CI, 1.16-3.92), COPD (9.8% vs 4.2%; OR = 2.48; 95% CI, 1.08-5.74), and ≥14 days of poor mental health per month (33.2% vs 11.4%; OR = 3.74; 95% CI, 2.36-5.92). Compared with the referent group, the dual-use group included a greater percentage of adults who currently smoked cigarettes (65.6% vs 8.3%; OR = 5.77; 95% CI, 3.66-9.10) and a greater percentage who had used prescribed pain medication in the past year (32.0% vs 15.1%; OR = 2.63; 95% CI, 1.66-4.19).
Characteristics of adults who reported using both marijuana (any intake mode) and EVPs (with or without tetrahydrocannabinol), compared with adults using either or neither marijuana or EVPs, in the previous 30 days, Utah, 2018 a
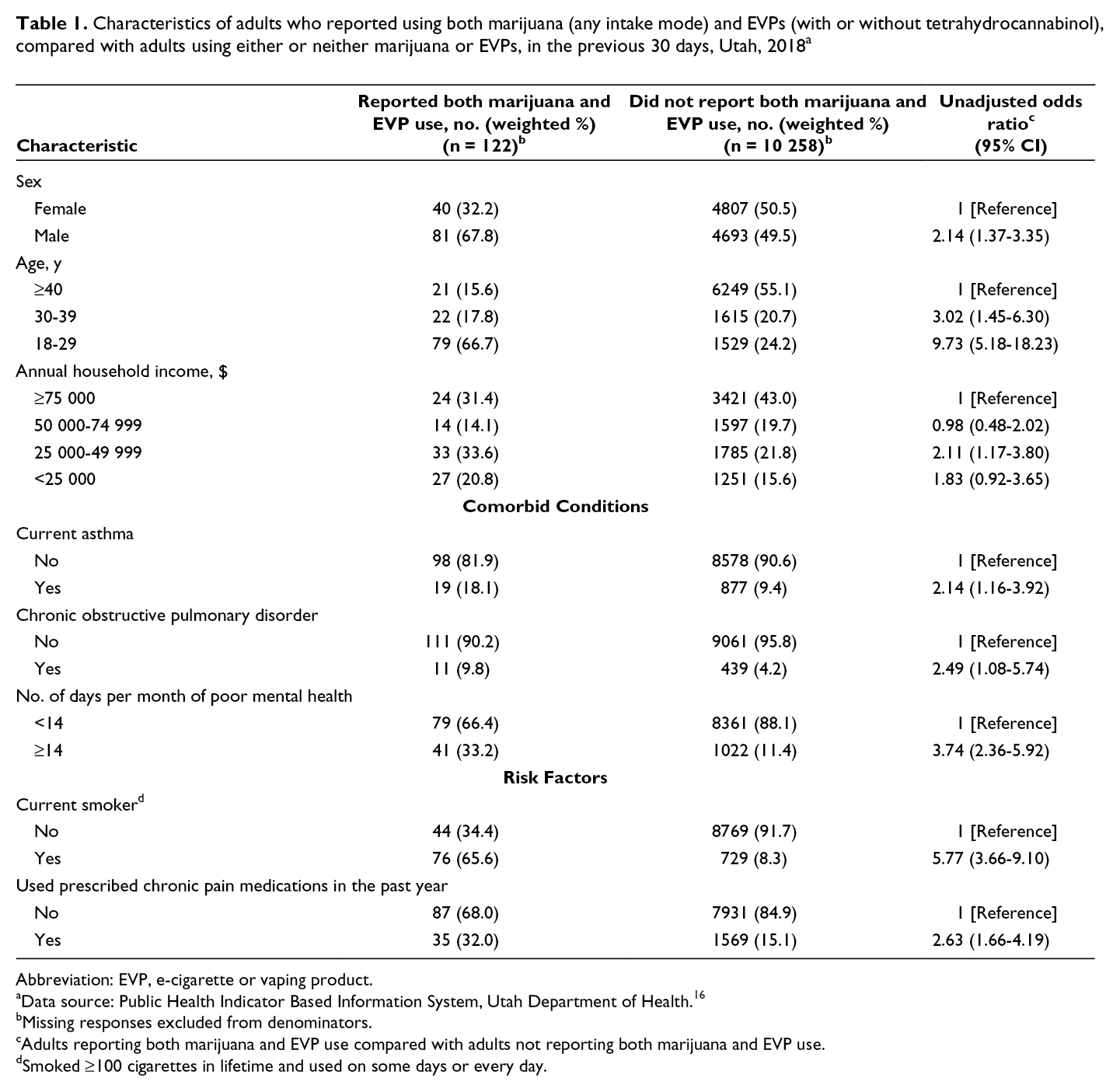
Abbreviation: EVP, e-cigarette or vaping product.
aData source: Public Health Indicator Based Information System, Utah Department of Health. 16
bMissing responses excluded from denominators.
cAdults reporting both marijuana and EVP use compared with adults not reporting both marijuana and EVP use.
dSmoked ≥100 cigarettes in lifetime and used on some days or every day.
Multivariable Analysis
In the multivariable analysis, adults in the dual-use group, after adjusting for age, sex, and income, had greater adjusted odds of being male (aOR = 3.29; 95% CI, 1.82-5.96) and of being aged 18-29 (aOR = 12.44; 95% CI, 6.15-25.14) or aged 30-39 (aOR = 3.75; CI, 1.73-8.12), compared with being aged ≥40 (Table 2). Compared with the referent group, adults in the dual-use group had greater odds of having asthma (aOR = 2.09; 95% CI, 1.02-4.31), COPD (aOR = 2.94; 95% CI, 1.19-7.93), or ≥14 days of poor mental health per month (aOR = 2.30; 95% CI, 1.23-4.32). Lastly, compared with the referent group, adults in the dual-use group had greater odds of currently smoking cigarettes (aOR = 4.56; 95% CI, 2.63-7.93) or having used prescribed chronic pain medication in the past year (aOR = 2.13; 95% CI, 1.06-4.30). Risk factors were consistent between this model (ie, with the referent group of adults who used either marijuana or EVPs, or neither of the two) and the alternative model with the referent group limited to adults who used neither of the two.
Multivariable regression model of risk factors for using both marijuana (any intake mode) and e-cigarette, or vaping, products (with or without tetrahydrocannabinol) in the previous 30 days, Utah, 2018 a
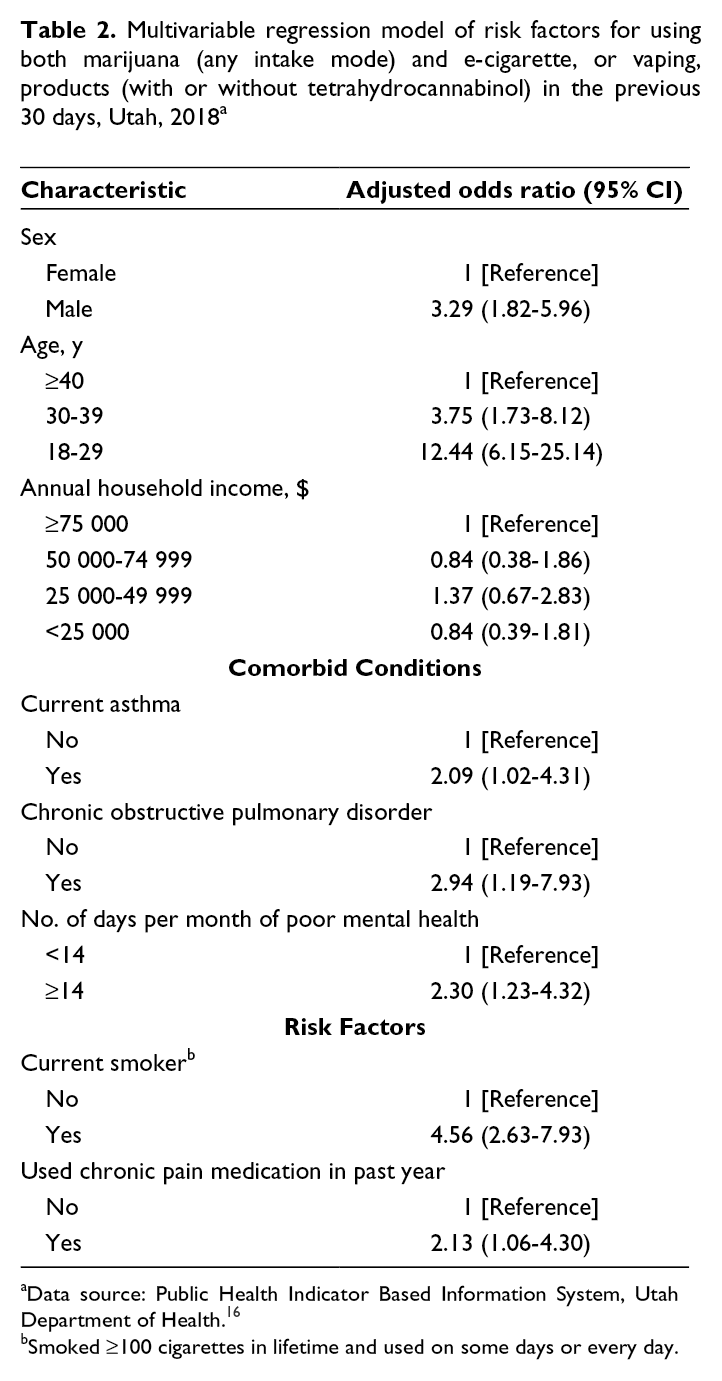
aData source: Public Health Indicator Based Information System, Utah Department of Health. 16
bSmoked ≥100 cigarettes in lifetime and used on some days or every day.
Discussion
Adults in Utah who reported using both marijuana and EVPs, as compared with a referent group of adults who used one or neither of the two, had greater odds of having respiratory problems, taking chronic pain medication, and poor mental health, in addition to being younger and male; they also reported using marijuana more frequently than those who reported using marijuana only. Our findings, coupled with the evidence that the use of multiple inhalant substances and THC-containing EVPs were implicated in the 2019 EVALI outbreak, suggest that this group of adults may have a constellation of risk factors for potential addiction and other harmful effects.
Multivariable analysis showed that adults in the dual-use group tended to be young and male, which aligns with previously reported high rates of both marijuana and EVP use among men 8,12,20 and young adults. 11,12,20 Both male sex and young age are associated with underlying psychological characteristics (eg, impulsivity or sensation seeking) that predict both marijuana use and EVP use. 1,12 Young people might also face pressure to experiment, 4 or they might prefer THC-containing, cartridge-based EVPs to smoking combustible marijuana because they want to conceal use. 11,20 In addition to substantially higher odds of being aged 18-29 (compared with aged ≥40) in the dual-use group, the higher odds of being aged 30-39 suggests that adults in Utah approaching midlife are also at risk for multiple inhalant substance use and related harmful effects. Approximately one-quarter of EVALI cases in Utah were among patients aged 30-39. 10
Respiratory comorbid conditions were common among adults using both EVPs and marijuana. The higher odds of having asthma or COPD among people using EVPs and marijuana compared with those using one or neither could be attributable to past smoking, especially given that studies of adolescents 8,20 -22 and young adults 6,23 associated cigarette smoking with dual use. In addition, people with preexisting respiratory problems could perceive reduced risk in using EVPs relative to smoking. 5,11 -13,21 EVALI patient samples in Utah, 10 Illinois and Wisconsin, 24 and Indiana 25 had high rates of asthma (20%-30%). Our finding of an additional association of COPD and dual use was potentially enabled by our focus on adults. Further research should assess the degree to which preexisting respiratory comorbidities among people using marijuana and EVPs could contribute to additional or more severe respiratory illnesses and injuries.
Adults in the dual-use group had more than twice the odds of having ≥14 days of poor mental health in the past month. Studies indicate that dual use of marijuana and EVPs is associated with both depression and suicidal ideation 7 and that poor mental health is associated with multiple substance use. 4 However, the directionality in these relationships is unclear. Some adults might be using EVPs or marijuana impulsively to cope with anxiety or depression, 4 and adults who use marijuana to cope might seek out THC-containing, cartridge-based EVPs because they have a higher THC content than combustible marijuana. 10,11 Poor mental health could also prompt more frequent use of THC-containing EVPs and the development of addictive behavior. 7 EVALI patient samples in Utah, 10 Illinois and Wisconsin, 24 and Indiana 25 also had high reported rates of anxiety (26%-34%) and depression (22%-25%), further suggesting that poor mental health could be linked with multiple substance use.
Smoking combustible cigarettes was also common among adults in the dual-use group, with more than 4 times greater odds compared with the referent group. Although the rate of tobacco cigarette use among adults is lower in Utah (9%) than in the United States (14%), 26 the high rate of current cigarette smoking (66%) observed in the dual-use group in our study suggests that nicotine use could be part of a broader array of substance use concerns in this population. One study reported that 90% of people who had ever used THC-containing EVPs had also used nicotine-containing EVPs, 27 and about 15% of EVALI patients were found to use only nicotine-containing EVPs, even after biomarker validation. 9 Using both marijuana and EVPs has also been associated with alcohol use 6,22 and higher-frequency marijuana use, 22 the latter of which was mirrored in our study results.
Finally, using both marijuana and EVPs was associated with the use of prescribed chronic pain medications. For people with chronic pain, using marijuana with or without a prescription might be perceived as an additional therapeutic option to manage pain and daily activities. Using THC-containing EVPs might be preferable to smoking combustible marijuana to allow for a higher dosage of THC 14 or for more discreet use when it is not being used socially. 11,12,20,22 In Utah, about 50% of adults who use marijuana who also have chronic pain reported using marijuana medicinally, compared with only 33% of all adults who use marijuana. 28
Annual household income was significant only in the univariate analysis, mirroring previous studies that reported limited evidence for associations between EVP use and socioeconomic status 20,21 or parental education level. 29 However, evidence supports a link between low school performance and dual use of marijuana and EVPs among adolescents. 4,7 For the dual-use group of adults in our study, lower income could be related to a generally higher likelihood of inhalant substance use, as reported for cigarette smoking, 14 or underlying health problems (eg, chronic pain) that could affect income.
Strengths and Limitations
This study had several strengths, including that it provided a representative, population-level analysis of the characteristics of people who use both marijuana and EVPs. Second, this study focused on adults, which adds information to previous studies that focused largely on adolescents and young adults. Third, this study identified sociodemographic, behavioral, and health-related factors associated with the dual use of marijuana and EVPs.
The study also had several limitations. First, the time intervals used to assess current EVP use (some days or every day) and current marijuana use (≥1 day during the previous 30 days) differed. The measure used to assess marijuana use may have captured more data than the measure used to assess EVP use because it accounted for nonroutine and intermittent use. Second, the sample size of 122, while representative, was small, especially when considering subgroups. Third, previous studies pointed to both macrolevel factors (eg, substance and product availability) and microlevel factors (eg, impulsivity or self-esteem) as important determinants of marijuana and EVP use 11,12 ; these variables were not available in our analysis. Fourth, because our data did not examine specific intake modes, we could not comment on risk profiles associated with various subgroups of adults engaged in dual use of EVPs and marijuana, such as people who use both nicotine-containing and THC-containing EVPs. 30 Fifth, we did not include race and ethnicity as predictors because of data constraints and limited descriptive evidence for racial or ethnic differences in dual use in our sample or in Utah’s EVALI outbreak. One previous convenience-sample study found no racial or ethnic differences in use of THC-containing EVPs, 11 whereas another study found less likelihood of use among African American people compared with White people 10 ; these potential differences merit further consideration. Sixth, interaction effects might have helped to identify potential interrelations of factors (eg, the effect of age on smoking, or on poor mental health) for which ORs differed between the univariate and multivariable analyses, but we could not accommodate these factors within the available degrees of freedom.
Finally, we could not capture data on Utah-specific disparities in substance use based on religion; such disparities would affect the generalizability of the findings to other states. Most people in Utah are affiliated with the Church of Jesus Christ of Latter-day Saints (LDS), which encourages abstinence from cigarettes and marijuana and clarified in 2019 that church members should also abstain from EVPs. 31 High rates of EVP use and EVALI in Utah, then, could be attributable to previously less explicit guidelines on vaping for members or to higher rates among non-LDS populations that offset the lower rates among LDS populations, as suggested in studies of chronic disease. 32
Conclusions
Our findings suggest that clinicians and public health practitioners should consider factors associated with adults’ dual use of marijuana and EVPs or use of THC-containing EVPs specifically, including respiratory conditions, poor mental health, and chronic pain management, which could increase adults’ risk for additional or exacerbated adverse outcomes. Although EVPs generally contain fewer harmful chemicals than smoke from combustible tobacco products, they should not be used by adolescents, young adults, pregnant women, or adults who do not currently use tobacco products. 33 The high rate of cigarette smoking observed in our study among adults using EVPs and marijuana suggests that clinicians should ask patients who smoke cigarettes about e-cigarette use, and cessation messages should reference the rapidly expanding landscape of tobacco products. THC use is associated with a range of adverse health effects, particularly with prolonged or frequent use. People engaging in ongoing use that leads to impairment or distress should seek evidence-based treatment from a health care professional.
Not using marijuana and EVPs, including THC-containing EVPs, is the best way to avoid adverse effects such as addiction, mental distress, and new or exacerbated pulmonary illnesses and injuries. Clinicians and health promotion specialists can better design and deliver prevention messaging if they understand the characteristics of populations at risk of dual use of marijuana and EVPs. Given the ongoing health risks associated with dual use and the potential for future outbreaks associated with unknown substances in the EVP market, clinicians and public health practitioners should remain attuned to ways in which preexisting conditions, mental health, pain management needs, and history of use of inhalant substances might cause people to use marijuana concurrently with EVPs or THC-containing EVPs. In addition, state surveillance instruments should consider identifying all modes of marijuana intake, 34 including the most frequently used mode, to better differentiate the risks associated with various forms of inhalant substance use.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.