
Abstract
The Centers for Disease Control and Prevention (CDC) and state, territorial, and local health departments have expanded efforts to detect and respond to HIV clusters and outbreaks in the United States. In July 2017, CDC created the HIV Outbreak Coordination Unit (OCU) to ensure consistent and collaborative assessment of requests from health departments for consultation or support on possible HIV clusters and outbreaks of elevated concern. The HIV OCU is a multidisciplinary, cross-organization functional unit within CDC’s Division of HIV/AIDS Prevention. HIV OCU members have expertise in areas such as outbreak detection and investigation, prevention, laboratory services, surveillance and epidemiology, policy, communication, and operations. HIV OCU discussions facilitate problem solving, coordination, and situational awareness. Between HIV OCU meetings, designated CDC staff members communicate regularly with health departments to provide support and assessment. During July 2017–December 2019, the HIV OCU reviewed 31 possible HIV clusters and outbreaks (ie, events) in 22 states that were detected by CDC, health departments, or local partners; 17 events involved HIV transmission associated with injection drug use, and other events typically involved sexual transmission or overall increases in HIV diagnoses. CDC supported health departments remotely or on site with planning and prioritization; data collection, management, and analysis; communications; laboratory support; multistate coordination; and expansion of HIV prevention services. The HIV OCU has augmented CDC’s support of HIV cluster and outbreak assessment and response at health departments and had important internal organizational benefits. Health departments may benefit from developing or strengthening similar units to coordinate detection and response efforts within and across public health agencies and advance the national Ending the HIV Epidemic initiative.
Keywords
Early detection of HIV clusters and outbreaks offers opportunities to rapidly respond to interrupt transmission. HIV cluster detection and response efforts have expanded considerably in recent years, and responding to HIV clusters and outbreaks is 1 of 4 pillars of the federal Ending the HIV Epidemic initiative (the other 3 pillars are diagnosis, treatment, and prevention). 1,2 Localized increases in the number of HIV diagnoses associated with injection drug use (IDU) in the setting of the opioid crisis have also led to increased attention to opioid-related HIV transmission and outbreaks. 3
HIV Cluster and Outbreak Detection
The Centers for Disease Control and Prevention (CDC) and state, territorial, and local health departments systematically identify clusters through analysis of HIV diagnosis data and nucleotide sequence data that are routinely reported to state and local HIV surveillance programs and then to the National HIV Surveillance System. These data can be used at local and federal levels to identify (1) increases in diagnoses above an expected baseline, also known as time–space clusters, 4 -10 and (2) molecular clusters of similar HIV nucleotide sequences, indicative of ongoing, rapid transmission. 11 -13 In addition, clusters may be identified or reported by health care providers and community members 14 -16 or through contact tracing performed as part of HIV partner services. 17 -19
HIV Cluster and Outbreak Investigation and Response
As clusters are identified, health departments review existing data to determine the level of concern and need for enhanced investigation and response. For clusters of concern, it is important to understand the extent of the network, which might include not only people with diagnosed HIV infection but also people with undiagnosed HIV infection and people at risk for HIV infection. People found to be part of the network are linked to appropriate services, such as testing and care for HIV infection and other infectious diseases, prevention services (eg, preexposure prophylaxis, syringe services programs), and other essential support services (eg, housing, social services). In addition to linking people to needed services, cluster and outbreak response involves identifying and addressing gaps in care and prevention services by implementing new services, expanding existing services, or modifying services to improve accessibility and acceptability.
HIV cluster and outbreak response is an inherently multidisciplinary activity, requiring collaboration and coordination across multiple subject matter areas, organizational units, and agencies. Health departments have implemented prevention activities such as HIV testing, contact tracing, and linkage to treatment for years. However, in contrast to public health efforts to detect and respond to other pathogens, such as tuberculosis or foodborne infections, detecting and responding to HIV clusters and outbreaks is a relatively new area of focus, with substantial expansion of these activities in recent years. 20 -22 Therefore, CDC and health departments are still developing systems and structures to promote collaboration and coordination for HIV cluster and outbreak response.
CDC supports routine HIV cluster detection and response efforts in state, territorial, and local health departments in all 50 states, the District of Columbia, Puerto Rico, and the US Virgin Islands through its flagship HIV surveillance and prevention program for health departments. 20 The federal Ending the HIV Epidemic initiative, through the “respond” pillar, supports health departments in 26 states, the District of Columbia, and Puerto Rico to develop enhanced HIV cluster detection and response activities, including establishing new partnerships, workforce, processes, data systems, and policies to facilitate robust, real-time cluster detection and response and escalate efforts to appropriately respond to large HIV outbreaks when needed. 21 This program includes a requirement to develop a standing committee that meets regularly to guide the response to HIV clusters; through this group, health departments can collaborate to build strong cluster response programs, coordinate investigation and response efforts, and identify and address gaps in programs and services that are revealed by cluster detection and response.
We describe the CDC HIV Outbreak Coordination Unit (OCU), its first 2½ years of experience during July 2017–December 2019, and lessons learned. This information can inform efforts of health departments and other public health organizations that are developing systems and structures to coordinate response efforts across subject matter areas or large and diverse organizations.
Methods
Rationale for Creating the HIV OCU
Before the HIV OCU was established, staff members at the CDC Division of HIV/AIDS Prevention (DHAP) who learned of possible HIV clusters or outbreaks from health departments, media coverage, health care providers, or others (eg, staff members at academic institutions) handled consultation in a nonstandardized manner, depending on the program they oversaw and their own areas of subject matter expertise. As a result, the level of support varied, and internal communication about these situations was sometimes challenging or lacking.
To address these challenges, DHAP staff members with expertise in various program areas collaborated to create the HIV OCU in July 2017. DHAP staff members adapted the HIV OCU model from a similar unit within CDC’s Division of Tuberculosis Elimination and modified it to consider context specific to HIV and the structure of DHAP.
Structure and Operations of the HIV OCU
The HIV OCU is a functional unit that includes a multidisciplinary group of DHAP staff members with expertise in cluster and outbreak detection, surveillance and epidemiology, cluster and outbreak investigation, cluster and outbreak response, HIV testing, HIV treatment, HIV prevention, laboratory services, HIV program implementation, policy, communication, operations, and budget.
The HIV OCU reviews and discusses events of elevated concern that meet the following criteria: (1) any explicit health department request to DHAP for consultation or assistance to investigate or respond to a possible HIV cluster or outbreak; (2) possible HIV clusters or outbreaks with media coverage; (3) HIV clusters detected through analysis of national surveillance data that are of special concern (eg, rapid growth, vulnerable population, high levels of drug resistance); or (4) events that span multiple states. One or 2 key HIV OCU points of contact are assigned for each event to communicate directly with the health department, monitor investigation and response activities, coordinate CDC response to requests for support, and provide routine updates to the OCU. These staff members are often project officers with an established relationship with that health department.
Key information presented at HIV OCU meetings includes a description of how the event was identified, key epidemiologic findings, investigation and prevention efforts to date, local capacity, and requests by and needs of the health department. HIV OCU meetings facilitate situational awareness, cross-branch problem solving, and coordination of follow-up with the health department about new activities and intersections with work currently supported by DHAP. Each time an event is discussed, consideration is given as to whether the event should remain open (ie, the HIV OCU needs to continue monitoring and discussing the event) or can be closed (ie, ongoing monitoring can be conducted through routine project officer relationships). Some events with intensified support remain open for months, whereas less concerning events are often closed quickly. For events that remain open, support needs often evolve (Figure 1).
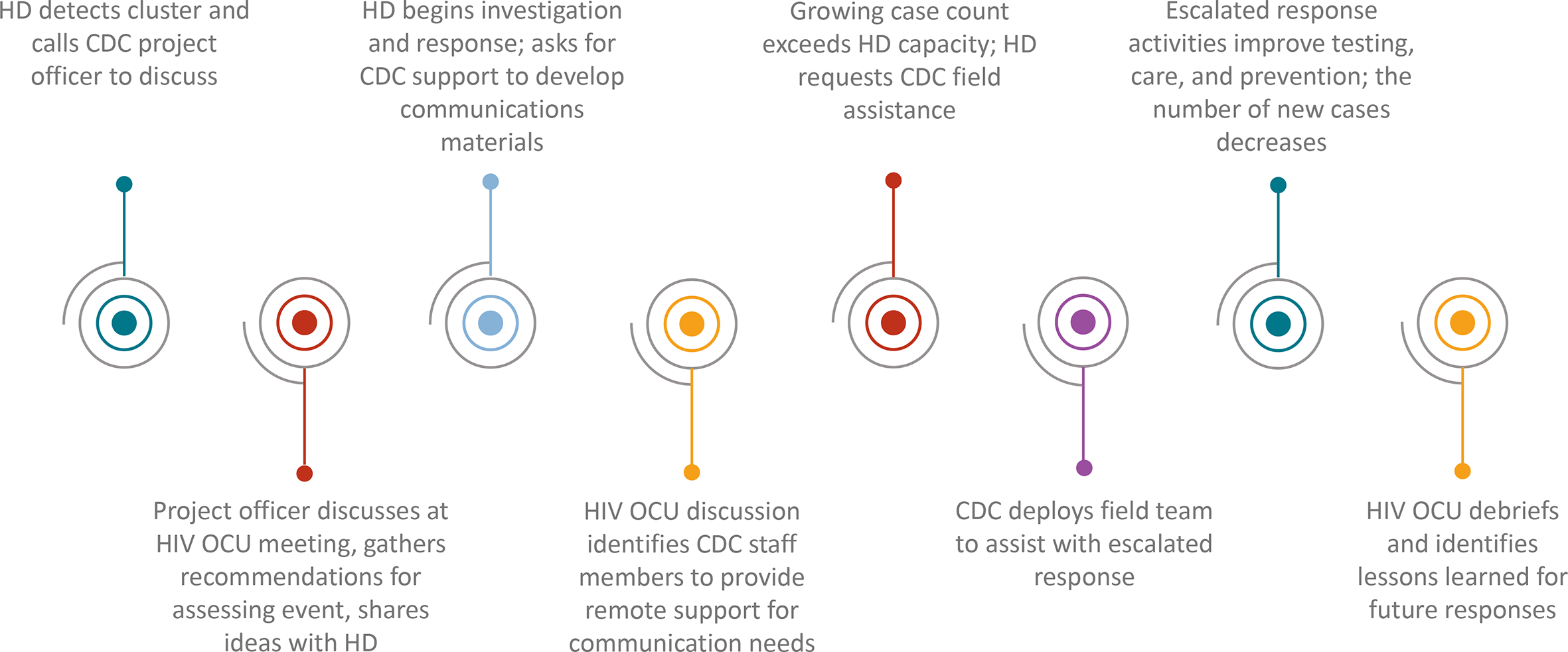
Example timeline of outbreak investigation and response support by the CDC HIV Outbreak Coordination Unit (OCU). This timeline is meant to be illustrative, as each event differs in the timeline and needs. Abbreviations: CDC, Centers for Disease Control and Prevention; HD, health department.
Epidemiologic, laboratory, or other data discussed at HIV OCU meetings are de-identified before transmission to CDC in keeping with DHAP policy. HIV OCU discussions focus on important aggregate findings and are treated as sensitive. All HIV OCU members receive security and confidentiality training and sign confidentiality agreements.
Outcomes
During July 2017–December 2019, the HIV OCU reviewed 31 events involving 22 states in all 4 US Census regions. CDC was notified of these events through various mechanisms, including health department notification to CDC of HIV clusters or outbreaks identified locally (n = 18), public communication or media coverage (n = 7), CDC national cluster analysis (n = 4), or notification by a non–health department partner (n = 2). Seventeen of the 31 events involved HIV transmission known to be primarily associated with IDU, whereas the other 14 events related to sexual transmission or a combination of transmission categories.
Of the 31 events, 18 were discussed at 1 or 2 HIV OCU meetings. Often, a small increase in HIV diagnoses was detected and, upon review, it was determined that the health department did not need HIV OCU support and the event could be closed. The project officers monitored the event and informed the HIV OCU if future discussion was needed. Nine events were discussed at 3-6 meetings; these events typically involved an HIV outbreak response led by the health department with ongoing remote CDC consultation. Four events, in which the health department requested on-site investigation and response support, were discussed at 8-14 HIV OCU meetings; 3 of these events involved large increases in HIV diagnoses associated with IDU, and the fourth event involved increases in a geographic area that CDC deemed vulnerable to IDU-associated outbreaks. 23 For 1 such event, CDC implemented an incident management system to coordinate support for the state and local health departments. Of the 31 events, 6 events remained open for discussion as of December 2019; 3 had been open for fewer than 6 months, and 3 had been open for more than 6 months.
Domains in which DHAP supported health departments included data management, analytical support, planning and prioritization, surveillance, qualitative and ethnographic interviews and other enhanced data collection, informatics, data security and confidentiality, community engagement, communications, multistate coordination, partner services surge capacity, and expansion of HIV prevention services, including HIV testing, preexposure prophylaxis, linkage-to-care services, substance abuse treatment, and syringe services programs. CDC delivered this support through remote assistance, on-site assistance, capacity-building assistance provided by DHAP-funded organizations, and by facilitating peer-to-peer consultation. For 10 events, the DHAP laboratory tested blood specimens, including HIV sequencing, and conducted phylogenetic and transmission network analyses.
Lessons Learned
In its first 2½ years, the HIV OCU augmented CDC’s support of HIV cluster and outbreak assessment and response at health departments, an activity critical to the success of the Ending the HIV Epidemic initiative. HIV cluster and outbreak response activities, whether at CDC or at health departments, require a full range of HIV expertise in surveillance, prevention, and care and often require new or improved collaborations to address unique challenges experienced by communities affected by rapid transmission. The HIV OCU contributed to improvements in supporting cluster detection and response activities at health departments by enabling rapid identification and mobilization of CDC expertise to rapidly interrupt transmission.
Improvements to Support Provided to Health Departments
The HIV OCU has strengthened DHAP support for HIV cluster and outbreak response activities at health departments in multiple ways. It has strengthened and streamlined CDC communication with health departments about possible outbreaks and increased access to CDC expertise. For example, before the HIV OCU was established, several DHAP staff members might have contacted a health department with an HIV outbreak to offer support and request information. Now, 1 or 2 points of contact in DHAP gather information, assess needs, and coordinate CDC support, maximizing the efficiency of communication between health departments and CDC.
The HIV OCU has also helped DHAP to build local capacity through CDC assistance and through facilitating communication among health departments to share experiences and lessons learned from similar responses. For example, because of the breadth of experience and knowledge among HIV OCU participants, DHAP was able to quickly share examples of investigation instruments (eg, questionnaires, qualitative interview guides, medical record abstraction forms) with health departments, reducing the effort required to implement these tools amid an outbreak. Discussions during HIV OCU meetings also led DHAP to recognize important similarities with previous HIV outbreaks and facilitate direct communication among health departments with similar outbreaks. In one instance, these connections led to an ongoing, health department–led peer-to-peer working group among health departments responding to HIV outbreaks among people who inject drugs.
HIV OCU activities have also allowed DHAP to identify common needs for health department support and prioritize developing tools to support them. The work of the HIV OCU helped to identify needs for communications materials, such as examples of health alerts, letters to health care providers, and press releases, which were developed and made available to all health departments. 24
Internal Organizational Benefits
The HIV OCU has also had important organizational benefits for DHAP; these benefits might also be present for health departments establishing a similar entity. The HIV OCU has enhanced communication among key contacts in various organizational units within DHAP. This enhanced communication has led to additional collaboration to develop programmatic resources to support HIV cluster detection and response.
Participation in the HIV OCU by DHAP staff members and fellows from a range of organizational units has provided valuable training on and exposure to cluster detection methods and outbreak investigation and response approaches. This experience has expanded the cadre of staff members readily available for future cluster and outbreak responses, and many OCU members have deployed as part of CDC field teams to support health department outbreak responses.
The HIV OCU has also accelerated development of a scaled approach to providing technical assistance to health departments (Figure 2). This scaled approach includes building the capacity of project officers and other DHAP staff members to support the initial phases of these activities as part of their routine work while also providing a range of more intensive remote or in-person support options. The scaled approach can also include use of an incident management system, which uses a standardized approach to emergency response to improve internal coordination of CDC support and collaboration among agencies during a response. 25 Another benefit of the HIV OCU is streamlined decision making, as evidenced when the HIV OCU facilitated rapid implementation of an incident management system and deployment of numerous staff members to support a health department with an escalated response to an HIV outbreak among people who inject drugs. 7
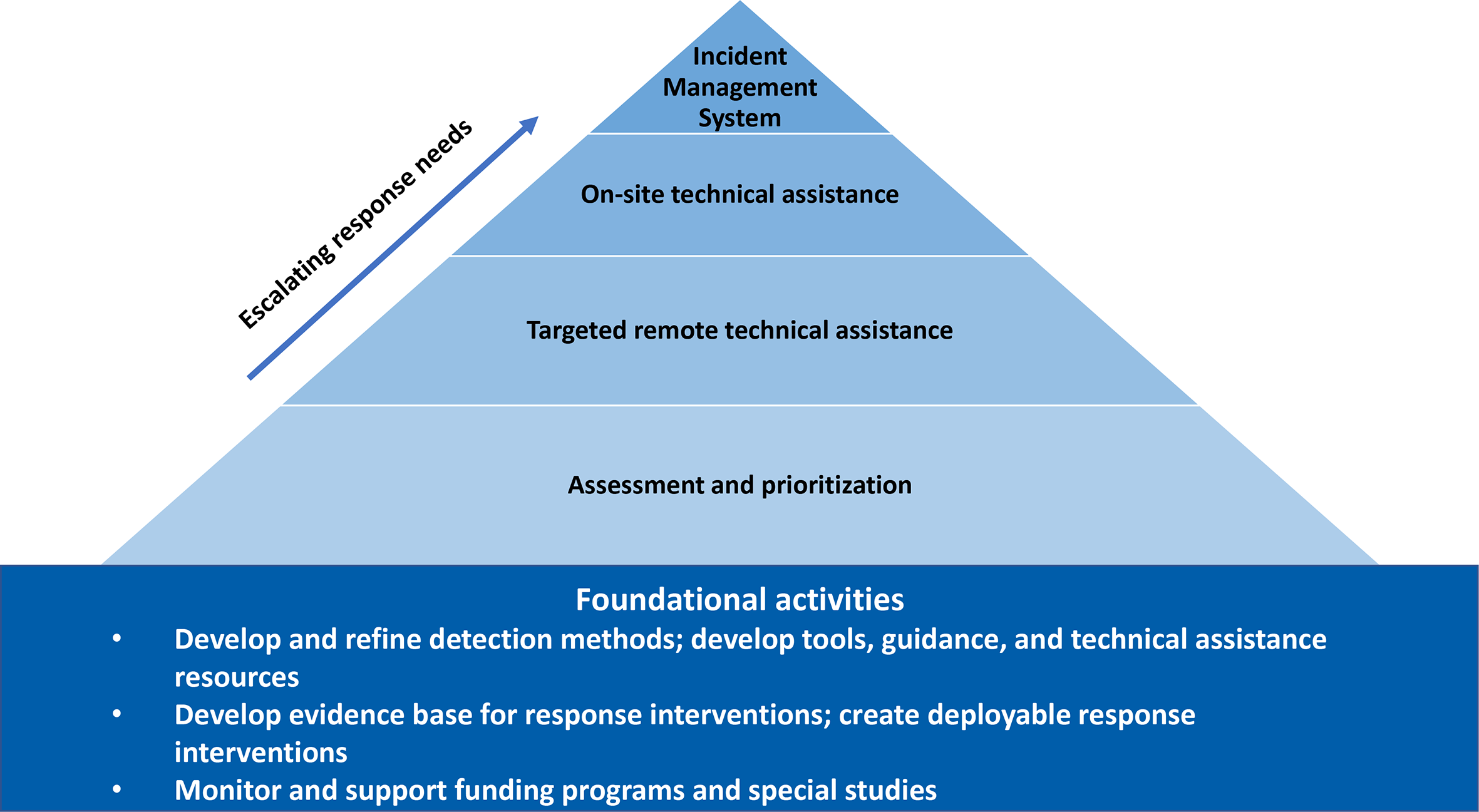
A scaled approach by the Centers for Disease Control and Prevention to provide technical assistance to health departments on HIV cluster and outbreak detection and response.
Future Directions
CDC has identified several areas for future development of the HIV OCU. These areas include expanding efforts to recruit and formally train DHAP staff members for field involvement in responses in which CDC surge support is requested; developing criteria for when an event should be considered closed; and continuing to strengthen collaborations with other divisions and federal agencies, including with staff members involved in cluster and outbreak responses related to other pathogens (eg, sexually transmitted diseases, tuberculosis, viral hepatitis) and other related conditions (eg, opioid use). In addition, a need exists to develop new standardized tools and deployable response interventions based on needs identified in individual health department responses.
Conclusion
As health departments develop or strengthen a unit or standing committee to coordinate HIV cluster and outbreak response activities, the experience of DHAP’s HIV OCU can provide valuable insight. Effective cluster detection and response programs require diverse experience and skills, representation from multiple relevant organizational units, and buy-in and participation from leaders with the authority to implement change. Establishing a regular, efficient meeting schedule along with ongoing review of data, open communication, and opportunities to build staff capacity can contribute to the success of these programs. The partnership, collaboration, and integration of surveillance, prevention, and care activities exemplified in the HIV OCU are essential to efforts to end the HIV epidemic in the United States.
Footnotes
Acknowledgments
The authors acknowledge all current and past HIV Outbreak Coordination Unit members.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.