
Abstract
Roughly 1.8 million individuals were detained or incarcerated in U.S. correctional facilities in 2022. Prior research has found that incarcerated persons are at increased risk for foodborne outbreaks. We aim to summarize recent national outbreak surveillance data and describe the nexus between disease burden and the law to inform prevention efforts. First, we describe epidemiological data for single-state correctional and all noncorrectional foodborne outbreaks during 1998–2022 that were reported to the Centers for Disease Control and Prevention’s Foodborne Disease Outbreak Surveillance System. Second, we summarize state statutes and regulations for seven key food safety provisions in the 10 states with the largest incarcerated populations. Incarcerated and detained individuals experience nearly seven times as many outbreak-associated illnesses per 100,000 individuals than the public. Further, the median number of illnesses per outbreak in correctional settings is nearly six times greater than noncorrectional settings. All 10 states codified all or most of the seven food safety provisions for food service establishments, whereas express legal requirements instituting these provisions within correctional facilities were largely absent. Legal interventions, rigorous food safety practices, and collaborations with health departments are critical tools needed to reduce foodborne outbreaks in correctional facilities.
Background
In 2022, roughly 1.8 million adults were incarcerated or detained in correctional facilities in the United States (Buehler & Kluckow, 2024). It is well established that incarcerated and detained individuals experience higher rates of chronic, mental health, and infectious diseases than the public (Binswanger et al., 2009; Maruschak et al., 2021; Wilper et al., 2009; Yi et al., 2017). Disease disparities may be accentuated by barriers from medical copays, limited sanitation and hygiene supplies, overcrowding, limited health resources, and lower health literacy (Bick, 2007; Lupez et al., 2024; Rampey et al., 2016). A prior analysis of outbreak surveillance data from 1998 to 2014 found more than fivefold higher illnesses per 100,000 population for correctional settings compared with noncorrectional settings, indicating that incarcerated populations are at increased risk for foodborne disease outbreaks (Marlow et al., 2017). Correctional facilities typically work on limited menus where all, or nearly all, individuals eat the same meal (which is potentially the only available source of food). Food may be prepared in large batches and held for long periods of time, potentially leading to larger foodborne outbreaks. Importantly, foodborne illness and outbreaks are largely preventable using evidence-based food safety operational controls, such as those outlined in the U.S. Food and Drug Administration (FDA) Food Code (Food Code, 2022). The Food Code specifies key operations (such as food safety training, food worker health, and time and temperature control of food products) to ensure safe food handling within retail and food service establishments; application of these practices has significantly reduced the risk of foodborne illness within retail settings (Food Code, 2022).
Outbreaks in correctional settings lead to preventable illness and are disruptive to correctional facilities, leading to costly medical and public health responses and security implications. To build on this prior work and inform the development of prevention efforts, we: (1) provide an updated analysis of outbreaks from 1998 to 2022 to determine if previous findings are consistent with more recent data, and (2) examine core food safety provisions in the ten states with the largest incarcerated populations to identify differences between codified requirements in correctional settings and noncorrectional settings using legal epidemiology. Legal epidemiology studies use standardized search strings and scoping criteria to collect and analyze laws related to a particular health outcome (Burris et al., 2016). Legal epidemiology allows researchers to understand what the law says and its relationship to a particular public health issue with the same rigor, replicability, and reliability as other epidemiological investigations. Coupling updated outbreak data with a legal landscape assessment serves to quantify current burden and describe initial avenues for potential action.
Methods
Outbreak Data and Epidemiology Methods
To better understand recent disease burden and underlying causes, we describe the epidemiological data for foodborne outbreaks in correctional facilities reported to the Foodborne Disease Outbreak Surveillance System (FDOSS) with a date of first illness onset from January 1, 1998, through December 31, 2022 (as of May 1, 2024) and compare these data with those in noncorrectional settings. This analysis includes more recent data (2015–2022) and reanalyzes data originally covered in the Marlow publication (1998–2014) as the FDOSS system is dynamic and older records may have been updated or corrected since they were first analyzed (Marlow et al., 2017). FDOSS collects voluntary reports of foodborne disease outbreaks from state, local, and territorial health departments in the United States. This system is the primary source of national data for illnesses, hospitalizations, and deaths; etiologic agents; implicated foods; contributing factors; and food preparation and consumption settings associated with reported foodborne outbreaks. Foodborne outbreaks are nationally notifiable and defined as two or more cases of a similar illness resulting from ingestion of a common food (Centers for Disease Control & Prevention, 2011). Multistate outbreaks were excluded from the correctional data as they involved multiple exposure settings including but not limited to correctional facilities. Using data from 1998 to 2022, authors summarized all reported single-state outbreaks where food was eaten or prepared in a correctional facility (including adult and youth federal, state, local, and tribal prisons, jails, and other detention facilities) and compared them to all outbreaks that were reported to have occurred in noncorrectional settings (e.g., restaurants, schools, and health care facilities). We used the Federal Bureau of Justice Statistics and the Office of Juvenile Justice and Delinquency Prevention correctional population estimates (available at https://bjs.ojp.gov and https://ojjdp.ojp.gov) to calculate outbreak-associated illnesses per 100,000 population. We also used the U.S. Census Bureau population estimates (available at https://www.census.gov), subtracting incarcerated population estimates, to calculate outbreak-associated illnesses per 100,000 among populations in noncorrectional settings (estimates shown in the Supplementary Appendix, Table A1). SAS software version 9.4 was used for all analyses (SAS Institute Inc., Cary, NC).
Legal Epidemiology Methods
The legal scan summarizes state statutes and regulations (as of April 1, 2023) specific to seven key food safety provisions: (1) excluding ill food service staff from working, (2) prohibiting or minimizing bare hand contact with ready-to-eat food, (3) requiring food service workers to wash their hands, (4) requiring at least one food worker to be a certified food protection manager, (5) requiring training for all food service workers specific to food preparation, (6) specifying requirements for hot and cold holding practices, and (7) mandating inspections of food service operations. These seven provisions are included in the current FDA Food Code (Food Code, 2022) and present minimal infrastructural requirements to ensure food safety. The legal analysis covered the 10 states with the largest incarcerated populations (California (CA), Florida (FL), Georgia (GA), Illinois (IL), Michigan (MI), New York (NY), Ohio (OH), Pennsylvania (PA), Texas (TX), and Virginia (VA)), collectively representing 50% of the U.S. incarcerated population in 2016 and 54% of the total average U.S. population 2010–2020 (Kaeble & Cowing, 2018; U.S. Census Bureau, Population Division, 2021). This sampling is not representative of all 50 states but provides a range of legal landscapes for this initial review of public health law.
Authors used a standard search string combining terms for each food safety provision in Westlaw (Thomson Reuters, Toronto, Canada) to identify related laws for the selected states:
food & (exclu!/25 illness ill sick!/5 worker employee) (glove bare! p.p.e. “personal protective equipment”/5 hand!/15 ready-to-eat) (wash!/5 hand/25 food) (certif!/10 “food protection manager”) (train!/25 inmate prisoner/5 worker employee) (hot/3 cold/5 regulat! hold!) (inspect!/20 food).
All laws identified through this process were reviewed and coded by attorneys for the presence or absence of the seven provisions using the Public Health Law Information Portal, hosted by the Centers for Disease Control and Prevention (CDC)’s Office of Public Health Law Services (https://phlip.cdc.gov/login) (Supplementary Appendix A2 and A3). Following data collection and coding, authors conducted a blind cross-check to identify and adjudicate any discrepancies. Courts are reluctant to interpret statutory and regulatory language to imply a burden of duty to the state, historically finding that the state’s police power should be strictly construed; therefore, we excluded laws that did not expressly apply to adult correctional facilities (E. Amos, as Comptroller, Plaintiff in Error, v. C. M. Conkling, and…, 1930; State v. F.C. Mitchell, 1940; Weber et al., 2021). Definitions for “retail food” and “food service establishment” vary from jurisdiction to jurisdiction. The authors broadly apply these terms to establishments that serve ready-to-eat food to the public and refer to them as “noncorrectional settings.”
Results
From 1998 to 2022, there were 284 reported single-state foodborne outbreaks in correctional settings, resulting in 26,136 illnesses, 224 hospitalizations, and 4 deaths (Table 1). The median number of illnesses per outbreak was nearly six times greater for correctional settings (median 40, range 2–1,644) than noncorrectional settings (median 7, range 2–1,939). Further, the median number of illnesses per 100,000 was nearly seven times greater for correctional settings (median 34, range 10–144) than in noncorrectional settings (median 5, range 2–10). Salmonella species were the most common etiology of single-state correctional outbreaks, followed closely by Clostridium perfringens (Table 2). Food was prepared on site at the correctional facility in over 90% of single-state outbreaks. Nineteen single-state correctional outbreaks (7%) reported the involvement of illicitly prepared products; 52% of which were caused by Salmonella species and 21% caused by Clostridium botulinum. A food vehicle was implicated in 48% of single-state correctional outbreaks and 41% of noncorrectional outbreaks during this time period.
Comparison of Reported Correctional and Noncorrectional Foodborne Outbreaks—Foodborne Disease Outbreak Surveillance System, 1998–2022
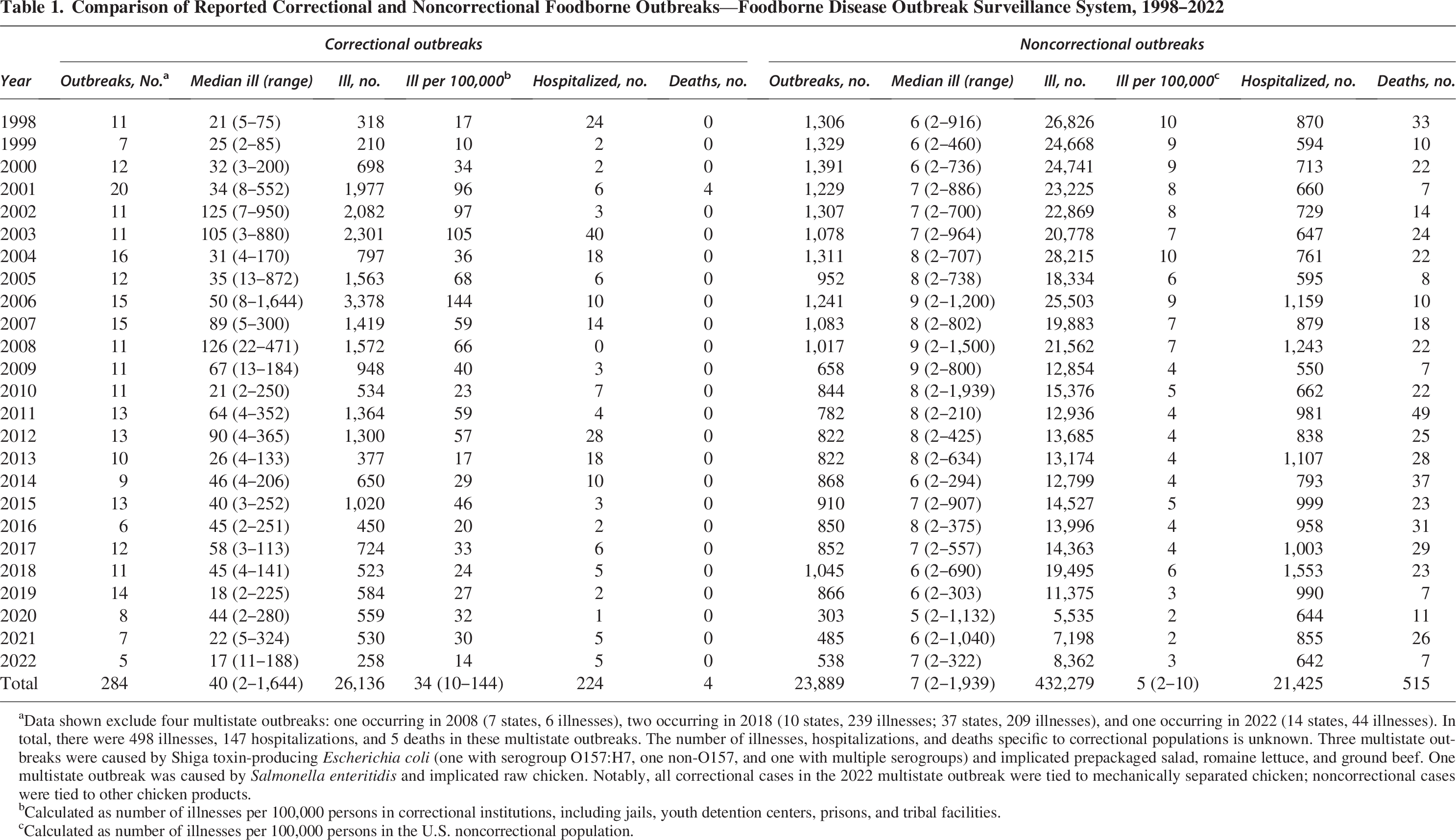
Data shown exclude four multistate outbreaks: one occurring in 2008 (7 states, 6 illnesses), two occurring in 2018 (10 states, 239 illnesses; 37 states, 209 illnesses), and one occurring in 2022 (14 states, 44 illnesses). In total, there were 498 illnesses, 147 hospitalizations, and 5 deaths in these multistate outbreaks. The number of illnesses, hospitalizations, and deaths specific to correctional populations is unknown. Three multistate outbreaks were caused by Shiga toxin-producing Escherichia coli (one with serogroup O157:H7, one non-O157, and one with multiple serogroups) and implicated prepackaged salad, romaine lettuce, and ground beef. One multistate outbreak was caused by Salmonella enteritidis and implicated raw chicken. Notably, all correctional cases in the 2022 multistate outbreak were tied to mechanically separated chicken; noncorrectional cases were tied to other chicken products.
Calculated as number of illnesses per 100,000 persons in correctional institutions, including jails, youth detention centers, prisons, and tribal facilities.
Calculated as number of illnesses per 100,000 persons in the U.S. noncorrectional population.
Comparison of Etiologic Agent in Correctional and Noncorrectional Foodborne Outbreaks—Foodborne Disease Outbreak Surveillance System, 1998–2022
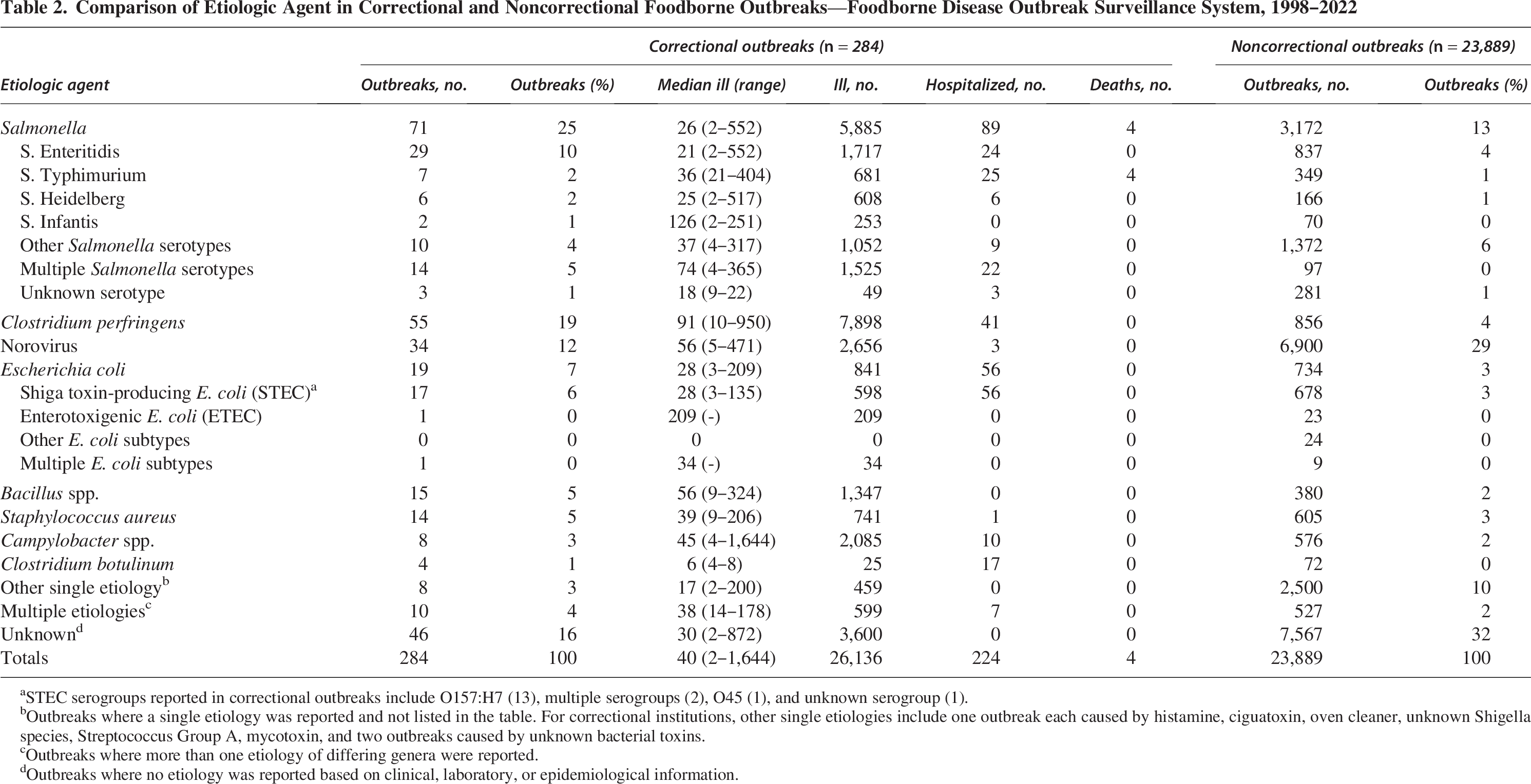
STEC serogroups reported in correctional outbreaks include O157:H7 (13), multiple serogroups (2), O45 (1), and unknown serogroup (1).
Outbreaks where a single etiology was reported and not listed in the table. For correctional institutions, other single etiologies include one outbreak each caused by histamine, ciguatoxin, oven cleaner, unknown Shigella species, Streptococcus Group A, mycotoxin, and two outbreaks caused by unknown bacterial toxins.
Outbreaks where more than one etiology of differing genera were reported.
Outbreaks where no etiology was reported based on clinical, laboratory, or epidemiological information.
Contributing factors are practices that most likely contributed to foodborne outbreaks, typically assigned by investigators to identify root causes for outbreaks. At least one contributing factor was reported in 54% of single-state correctional outbreaks and 45% of noncorrectional outbreaks. Time and temperature control issues (including, but not limited to, improper hot or cold holding, insufficient thawing, and insufficient cooking) were listed in 72% of single-state correctional outbreaks and 45% of noncorrectional outbreaks, and ill food workers were reported in 21% of single-state correctional outbreaks and 35% of noncorrectional outbreaks, indicating different causes of correctional outbreaks.
The Westlaw search identified 1,839 statutes and 1,848 regulations. All 10 states reviewed by the authors codified all or most of the seven food safety provisions for noncorrectional settings; however, express legal requirements instituting these provisions within correctional facilities were nearly absent (Table 3). California was the only state to have codified all food safety provisions for correctional facilities and food service establishments. Three states (CA, NY, and VA) required food safety inspections for correctional facilities. Two states (CA and FL) required handwashing among food workers, two states (CA and FL) specified hot and cold holding practices, and two states (CA and TX) required food safety training of food workers specifically for adult correctional facilities.
Comparison of Food Safety Laws for Food Service Establishments and State Adult Correctional Institutions, 2023 a
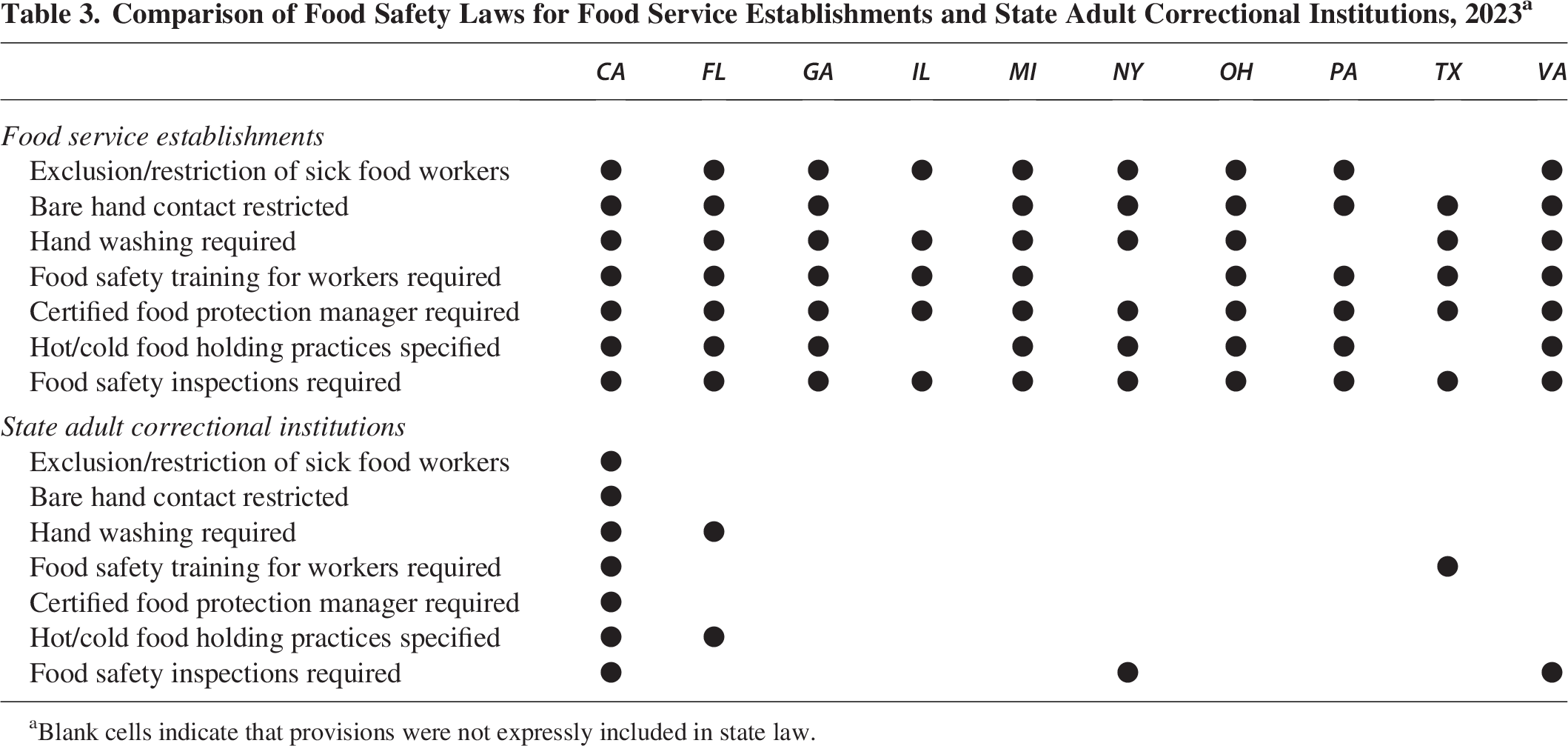
Blank cells indicate that provisions were not expressly included in state law.
Discussion
Building on the evidence of previous publications, these data demonstrate that incarcerated and detained individuals continue to be disproportionately impacted by foodborne outbreaks compared with the public, experiencing not only more outbreaks per population but also larger outbreaks. Outbreaks in correctional facilities result in preventable morbidity and mortality, placing acute strain on health services and potentially leading to logistical and security concerns for facility operations as they manage investigations, recalls, and health transportations. Using updated economic estimations of the per-case cost of foodborne illness by pathogen (Hoffmann et al., 2025), the costs of single-state correctional foodborne outbreaks from 1998 to 2022 would equate to roughly $193 million (in 2023 dollars). While this assumes that costs are comparable between correctional and public settings, this figure highlights the magnitude of economic impacts, much of which is incurred by the public through taxes allocated to correctional facilities. High economic burden per case is assigned to illnesses caused by Salmonella, C. botulinum, and Campylobacter due to the high occurrence of morbidity (including long-term morbidity) and mortality associated with these infections. Among single-state correctional outbreaks, these three etiologies accounted for 30% of illnesses, but 92% of estimated costs. As the incarcerated population ages, facilities should consider the increased likelihood of severe and fatal foodborne illness among older adults (Scallan et al., 2015).
Previous reports indicated a median of five (range: 1–11) foodborne outbreaks occurring annually in correctional facilities during 1974–1991 (Cieslak, 1996). Our analysis shows a median of 11 (range 5–20) single-state foodborne outbreaks annually across 1998–2022. Such a change may not reflect a true increase in correctional foodborne outbreaks as outbreak investigations and reporting practices have also changed over time. Of note, we observed fewer outbreaks reported in FDOSS from 2020 to 2022. The decrease may have been impacted by the SARS COV-2 pandemic. Overall, notifiable diseases, including foodborne illness, were less frequently reported during the SARS-COV-2 pandemic, potentially relating to changes in exposures, investigations, and reporting (Crane et al., 2022; Ray et al., 2021).
Mechanically separated chicken has been a growing concern for correctional outbreaks in the reported literature (Hutchinson et al., 2018; Oppegard et al., 2022; Taylor et al., 2015). Since 2014, three outbreaks in correctional settings were caused by mechanically separated chicken products, including a multistate outbreak in 2022, which was excluded from this analysis because it involved multiple settings. Raw mechanically separated poultry products are known to contain higher prevalence of Salmonella and Campylobacter than other chicken or turkey products in routine performance testing (Progress Report on Salmonella and Campylobacter Testing of Raw Meat and Poultry Products, 1998–2014, n.d.). Knowing that these products more frequently contain pathogens than other raw meat and poultry products, facilities should strongly consider the risks of using these products. If used, facilities should take additional precautions to make sure products are fully thawed before use and cooked to at least 165 °F.
The locations of food preparation and low reports of links to illicitly prepared products indicate food safety challenges are centered in correctional food service operations. Food preparation in correctional settings is complex, requiring the processing, cooking, and holding of large batches of food in centralized and disseminated settings. Nearly 20% of single-state correctional outbreaks were caused by C. perfringens but only represented 4% of outbreaks in noncorrectional settings. Outbreaks caused by C. perfringens commonly relate to improper cooking, cooling, and reheating of animal products (called time and temperature control issues) (Wittry et al., 2022). Time and temperature control issues were frequently cited contributing factors in correctional outbreaks, speaking to a lack of food safety operational control. Such issues can be addressed through low-cost and practical practices such as temperature logs during cooking and holding. Notably, hot and cold holding practices were only specified into law for adult correctional facilities in two of the ten states covered by our legal analysis.
Nine of 10 states reviewed had fewer food safety provisions expressly applied to state adult correctional facilities than for food service establishments, indicating that there could be different requirements, training, and enforcement of foundational food safety practices in correctional settings. Several states used generalized setting language within their legal statues to refer to places where food may be prepared (ostensibly including correctional facilities); however, since a specific notation of setting may facilitate enforcement, only provisions that explicitly addressed correctional facilities were included. Of note, where food safety provisions were recorded for both correctional and food service establishments, there were often discrepancies in the level of detail in the laws. For example: Section 113949.1 of the California Health and Safety Code provides detailed instructions on the types of illnesses that would warrant sick workers to be excluded from food service, clearly defining the pertinent illnesses, requirements for laboratory testing before returning to work, and provisions in case of food worker refusals. However, Title 15, Section 3052 of the California Code of Regulations (the portion of California Code citing health and safety requirements for correctional facilities) more generally lists, “an inmate food handler with any condition which may contaminate food shall be referred to the medical department for examination and shall not return to work in the food service area until medically cleared.” In other instances, legal codes for retail food establishments (such as those for inspection requirements in Title 12, Section 5–585 and Title 2, Section 5–585 of the Virginia Administrative Code) use verbatim language from the FDA Food Code, whereas provisions for correctional facilities (Title 6, Section 15–20 of the Virginia Administrative Code) more generally summarize purview, documentation, and review of jail kitchen facilities for food regulation compliance, but do not explicitly list inspection frequency or situations requiring additional inspections. Though both pairs of provisions indicate the exclusion of sick workers and the requirement for inspections of food facilities, the vagueness of the wording may be a barrier to equal implementation and enforcement of the code in correctional settings and generally indicate a difference in priority or food safety culture.
These data highlight opportunities to improve food safety in correctional facilities through policy and practice. First, jurisdictions can consider codifying food safety provisions like those required for retail food establishments. Specifically, greater food safety oversight within correctional facilities through inspections is of particular importance (U.S. Food & Drug Administration, 2024) and may require changes to permitting and department authorities. Inspections provide opportunities to review and reinforce food safety practices and build collaboration between correctional and public health partners. Only three of the 10 states reviewed explicitly required food safety inspections for correctional settings, whereas these are required for retail food establishments in all ten states. It is critical that inspection codifications specifically note that they are for the purpose of food safety and are not combined with overall facility inspections, which may cover topics like water, sanitation, and occupational health. Second, correctional facilities and accrediting agencies can consider adopting rigorous food safety practices like those found in the FDA Food Code to reduce illnesses, medical and outbreak investigation costs, and potential liability. Previous studies have directly linked application of various Food Code elements and decreased foodborne disease incidence or outbreak size in retail settings (Hedberg et al., 2006; Hoover et al., 2020; Hsuan et al., 2017; Kambhampati et al., 2016; Moritz et al., 2023). As a first step, CDC, in partnership with public health and correctional agencies, developed Model Food Safety Practices for Correctional Facilities (https://www.cdc.gov/correctional-health/publications/food-safety.html). This resource maintains the same rigor as the FDA Food Code but is tailored for food safety operations within correctional settings and directly addresses the common contributing factors identified in this analysis. Implementation of these Model Practices can be accomplished through training, development of standard operating procedures, record-keeping, and collaboration. Finally, improved collaboration between correctional and public health authorities could also enhance identification of outbreaks, food vehicles, contributing factors, and inform prevention efforts. Increased collaboration can have broad public health impacts, increasing the accuracy of disease surveillance and more rapid and appropriate response to health threats.
There are several limitations to these analyses. First, the epidemiology analysis is limited to outbreaks voluntarily reported to FDOSS, representing a subset of foodborne illnesses. Outbreaks in some settings (e.g., restaurants and schools) may be more likely to be investigated and reported. While record review and food histories may be easier to obtain in correctional facilities, medical copays, lack of autonomy, and sociocultural factors may limit health-care-seeking behavior (Canada et al., 2022; Lupez et al., 2024). Overall, the sensitivity of disease reporting for correctional facilities compared with noncorrectional facilities is unknown. Second, both FDOSS and Westlaw represent dynamic systems; they summarize data available at a single point in time and may differ from other reports, including the Marlow and colleagues’ publication (Marlow et al., 2017). Next, the scope of the legal analysis was limited. While states included in the legal review collectively accounted for a large proportion of the incarcerated population, they are not representative of state food safety laws nationwide. Importantly, food safety is regulated at the federal, state, and local levels; however, our legal analysis reviewed only statutes and regulations applicable to state, adult correctional facilities; laws promulgated at the local level were not included. Further, the legal review focused only on adult state correctional facilities and excluded locally operated facilities, jails, federally operated facilities, facilities for youth, and facilities operated by third parties on behalf of a state or locality, which may have their own distinct jurisdictional food safety laws. Last, this analysis did not examine facility policies or day-to-day practices, which might include more robust requirements than are found in the law. It is worth noting that even if correctional facilities did not expressly require food safety provisions in their legal code, they may be practiced or encouraged by government agencies, accreditation officials, and facilities.
Conclusion
Foodborne outbreaks present not only significant health risks to incarcerated and detained persons and correctional staff but also place logistical, medical, security, and financial strains on correctional systems. While foodborne outbreaks may not represent as common a health burden as other chronic and infectious diseases in correctional settings, they are preventable through the application of low-cost, evidence-based practices. Providing nutritious and safe food to large populations with diverse medical and religious needs is a challenging endeavor, and one that warrants resources and attention to achieve safer and more equitable food systems. States can consider codifying food safety expectations for correctional facilities into law. Importantly, while the law provides baseline requirements, the adoption of more food safety laws alone will not lead to demonstrable or sustained improved food safety practice. Rather, legal standards are a foundational tool that, when coupled with training, education, and enforcement, has the potential to improve the quality and safety of food served in correctional settings. Facilities and accrediting organizations can further supplement baseline legal provisions with rigorous food safety practices, such as those found in CDC’s Model Food Safety Practices for Correctional Facilities (Centers for Disease Control & Prevention, 2024). Future research is needed including quantitative studies to describe the impact of food safety regulations on disease burden as well as assessments of the application of food safety laws within correctional facilities. Future work may also seek to better describe the underlying factors of the incarcerated population which may contribute to differences in rates of foodborne illness (including differences in psychosocial motivations, knowledge, or behavior).
Authors’ Contributions
N.D.: Writing—original draft and formal epidemiology analysis (supporting); F.A.F.: Conceptualization (co-lead), writing—original draft, and formal legal analysis; D.F.: Formal legal analysis (co-lead) and writing—review and editing; K.L.: Formal legal analysis (co-lead) and writing—review and editing; S.H.: Formal epidemiology analysis (lead), visualization, and writing—review and editing; A.P.: Formal legal analysis; S.C.: Conceptualization, methodology, and supervision; M.H.: Conceptualization and writing—review and editing; V.R.: Conceptualization and writing—review and editing; H.K.: Conceptualization, formal epidemiology analysis, and writing—review and editing; M.P.: Formal legal analysis, supervision, and writing—review and editing; and H.W.: Conceptualization (co-lead), methodology, writing—original draft, and supervision.
Footnotes
Acknowledgment
The authors thank their state, local, and territorial health department colleagues who investigate and report foodborne outbreaks to FDOSS. They also thank Akshara Menon, Amanda Moreland, Joya Banerjee, Natalie Vawter, Hannah Bunting, Regen Weber, Ariana Perez, Sophia Gracias, Mason Ramsay, and Rachel Hulkower for their contributions to this analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and the CDC. Funding for the FDOSS is provided by the CDC.
Article Summary
A review of foodborne disease outbreaks and food safety laws in state adult correctional facilities.
Disclaimer
The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the CDC.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.