
Abstract
Objectives
Experiences of vicarious racism—hearing about racism directed toward one’s racial group or racist acts committed against other racial group members—and vigilance about racial discrimination have been salient during the COVID-19 pandemic. This study examined vicarious racism and vigilance in relation to symptoms of depression and anxiety among Asian and Black Americans.
Methods
We used data from a cross-sectional study of 604 Asian American and 844 Black American adults aged ≥18 in the United States recruited from 5 US cities from May 21 through July 15, 2020. Multivariable linear regression models examined levels of depression and anxiety by self-reported vicarious racism and vigilance.
Results
Controlling for sociodemographic characteristics, among both Asian and Black Americans, greater self-reported vicarious racism was associated with more symptoms of depression (Asian: β = 1.92 [95% CI, 0.97-2.87]; Black: β = 1.72 [95% CI, 0.95-2.49]) and anxiety (Asian: β = 2.40 [95% CI, 1.48-3.32]; Black: β = 1.98 [95% CI, 1.17-2.78]). Vigilance was also positively related to symptoms of depression (Asian: β = 1.54 [95% CI, 0.58-2.50]; Black: β = 0.90 [95% CI, 0.12-1.67]) and anxiety (Asian: β = 1.98 [95% CI, 1.05-2.91]; Black: β = 1.64 [95% CI, 0.82-2.45]).
Conclusions
Mental health problems are a pressing concern during the COVID-19 pandemic. Results from our study suggest that heightened racist sentiment, harassment, and violence against Asian and Black Americans contribute to increased risk of depression and anxiety via vicarious racism and vigilance. Public health efforts during this period should address endemic racism as well as COVID-19.
The COVID-19 pandemic has revealed and widened racial health and social inequities, traceable to structural inequities stemming from a legacy of legally sanctioned racism and contemporary forms of racial discrimination. 1 -8 Racism has caused excess deaths in communities of color during the pandemic, from COVID-19 and other sources. 1,2,9 Clear instances include the racially motivated murders of Black people and police brutality. Notable examples include the killings of Ahmaud Arbery, Breonna Taylor, George Floyd, and Rayshard Brooks in 2020. Other health hazards include rising instances of racial insults, harassment, and attacks on Asian American people, driven largely from stigmatizing language by elected officials. 10 -13 This volatile period is a historically important point of global reckoning with systemic racism and the multiple ways it surfaces. 9,14
Acts of racism against Asian and Black Americans have been salient during the COVID-19 pandemic and have become increasingly visible via social media and news coverage. 15 -17 Videos of George Floyd’s killing were widely shared and sparked widespread protest. 18 A video of a White woman who called the police after a Black man asked her to leash her dog went viral. 19 Racial harassment and xenophobic taunts against Asian Americans have also been publicized through news outlets. 20 -22 Acts of anti-Asian violence have risen, such as attacks on elderly Asian Americans and, most recently, the killing of 6 Asian American women in Atlanta, Georgia. 23,24
Social media also serves as a forum for expressing racist sentiment. 25 For example, analysis of race-related tweets demonstrated a 68.4% rise in negative tweets about Asians (from 9.8% in November 2019 to 16.5% in March 2020). 26 Other studies of trends in Twitter and Google data indicate an increased use of racist slurs during the COVID-19 pandemic. 22,27 -31 Research suggests that increased anti-Asian sentiment during this period is associated with politicians and conservative news outlets blaming China for the pandemic and racializing the disease as the “China virus.” 22,32,33
Vicarious Racism
Racially motivated attacks and other racial injustices have broad adverse population-level health implications. 34 -36 In contrast to direct interpersonal discrimination, vicarious racism is experienced indirectly, by hearing about or seeing racist acts committed against other members of one’s racial group, such as those of friends or family members, and witnessing acts of racism, either personally or on the news. 37 -40 Vicarious racism also includes hearing about or seeing racism that is not necessarily directed toward an individual but, rather, the entire racial group, such as racist rhetoric from public figures or racist posts on social media.
Such experiences may constitute a source of personal threat even for people not being directly targeted. Social identity theory posits that individuals derive self-image from values attached to their social groups. 41,42 Collective self-esteem includes not only how individuals personally evaluate their groups but also their beliefs about perceptions that people outside their group have of them (public regard). 43 According to this framework, actions that devalue or stigmatize entire groups may negatively affect self-concept and result in low self-esteem and poor mental health. 44,45
Other frameworks, such as “linked lives” and “common fate,” suggest that injustices committed against other members of the same social group are collectively shared and can be personally stressful. 40,46 -48 Neuroscience-based models suggest that experiences of racism directed at other individuals of the same racial group mirror the effects of social threats to the self and activate regions of the brain associated with direct experiences of ostracism, exclusion, and rejection. 49 -51 Accordingly, experiences of what some researchers have termed “secondhand racism” (analogous to “secondhand smoke”) can have potential spillover effects, precipitating physical, behavioral, and mental health responses beyond the immediate victim. 37 Racist events can trigger population-level changes in health, particularly among members of targeted groups. 52 -56 For example, surges in symptoms of depression and anxiety were found among Black Americans after the killing of George Floyd. 57,58 These findings are consistent with research suggesting broader mental health consequences of police killings of unarmed Black people. 59 Chinese and Vietnamese Americans who witnessed friends experience racial discrimination were at greater risk of past-year psychiatric disorder compared with people who did not experience this form of vicarious racism. 60 As a source of psychosocial stress, vicarious racism may also elicit maladaptive coping behaviors, such as alcohol and substance use. 35,61 Other research has found dysregulated physiologic responses to stress during periods of racism-related unrest. 62
Racial Discrimination Vigilance
Repeated exposure to racism may lead to efforts to brace for personal victimization, preemptive efforts to avoid being discriminated against, and learned hypervigilance. 63 -66 Vigilance to racial discrimination involves physical, behavioral, cognitive, and emotional attentiveness to the environment in anticipation of experiencing racism. 64,66,67 Vigilant coping responses include being tense or feeling worried about being the target of racial discrimination, persistent monitoring, and avoiding places where racial discrimination may occur. Qualitative reports suggest that vigilance has increased during the COVID-19 pandemic among Asian and Black Americans. For example, Asian Americans have reported leaving the house only when necessary and exercising particular caution when going outside. 20,21 Black Americans have also described “having to constantly be on high alert” during the COVID-19 pandemic; such vigilance “adds extra anxiety, and it’s always hard, but right now, it’s an exhausting task to even leave the house.” 68 This anecdotal evidence is supported by data indicating that more than one-quarter of Asian Americans and one-fifth of Black Americans feared being threatened or physically attacked during the COVID-19 pandemic. 17 Perseverative thoughts and emotions about being the target of racial discrimination may drain coping resources, resulting in increased levels of depression and anxiety. 69,70
Current Study
Most research on racism and mental health has focused on the effects of directly experienced racial discrimination and prejudice. 35,71 -73 Research on the mental health consequences of vicarious experiences and discrimination vigilance, which have become more salient during the COVID-19 pandemic among Asian and Black Americans, is limited. 31
Qualitatively distinct expressions of racism during the COVID-19 pandemic result in mental health tolls. 29,64,70 Additional studies are needed on the health implications of vicarious racism and racial discrimination vigilance during the COVID-19 pandemic among Asian and Black Americans. More broadly, a need exists for research on health outcomes other than COVID-19 that also represent important public health concerns in these populations.
The objective of our investigation was to examine two understudied facets of racism—vicarious racism and racial discrimination vigilance—in relation to depression and anxiety among Asian and Black adults in the United States during the COVID-19 pandemic. We hypothesized that greater experiences of vicarious racism and racial discrimination vigilance would be associated with worse mental health among Asian and Black Americans during this unprecedented period.
Methods
The Uncovering COVID-19 Experiences and Realities (UnCOVER) Study recruited adults aged ≥18 residing in Atlanta, Georgia; Chicago, Illinois; Los Angeles, California; New Orleans, Louisiana; and New York, New York, using Qualtrics Research Services, which randomly selected people who matched target criteria through their partnerships with market panel companies. We used quota sampling to achieve more even distribution of race groups. To help ensure data quality and integrity, we embedded attention checks throughout the survey, in the form of basic demographic questions that were asked early in the questionnaire and repeated later. We further evaluated entries with straight-line responding to multi-item measures (ie, providing the same response or non-differentiating responses to a series of questions), contradictory or highly improbable answers, outlying completion times, and other evidence of careless responding. The Institutional Review Board at Auburn University determined that study procedures and protocols were exempt from review. We collected data from May 21 through July 15, 2020. We restricted the current analysis to Asian (n = 604) and Black (n = 844) participants.
Measures
Vicarious Racism
Seven items were used to measure the frequency of hearing about or seeing other people of the same racial group experiencing racism (1) in public or (2) in the news; hearing about experiences of racism of (3) current or past romantic partners or (4) friends and family members; hearing racist things said by (5) politicians and (6) other public figures; and (7) seeing racist posts on social media during the COVID-19 pandemic. 38 We measured items on a 6-point Likert scale (0 = never, 1 = about once a month, 2 = a few times a month, 3 = once a week, 4 = a few times a week, and 5 = every day; Asian: α = 0.92; Black: α = 0.87).
We weighted the mean frequency score by using 3 items that assessed a participant’s response to experiencing vicarious racism: (1) the degree to which participants “thought about” these experiences (range, 0 = never to 4 = always) and (2) how “distressed” and (3) “concerned” they were about these experiences (range, 0 = not at all to 4 = extremely; Asian American: α = 0.89; Black American: α = 0.86). We calculated the mean score by dividing by 4 to create an impact weight variable (range, 0-1), which we then multiplied by the frequency score to obtain an overall score, an approach used in other self-reported racism measures. 74,75
For descriptive purposes, a single item assessed whether experiences of vicarious racism during the COVID-19 pandemic were “more than usual,” “less than usual,” or “about the same.” An additional parallel item assessed changes in respondents’ own experiences of “discrimination or being treated unfairly because of your race.”
Racial Discrimination–Related Vigilance
We measured racial discrimination–related vigilance as the mean of 4 items that assessed: (1) avoiding going to places, (2) feeling on guard, (3) being vigilant, and (4) being fearful “during the COVID-19 or coronavirus pandemic” because of the possibility of being discriminated against because of race. We adapted response options from previous measures of racism-related vigilance and measured on a 6-point Likert scale (0 = never, 1 = about once a month, 2 = a few times a month, 3 = once a week, 4 = a few times a week, and 5 = every day; Asian American: α = 0.95; Black American: α = 0.89). 76,77
Depression and Anxiety
We used the Patient-Reported Outcomes Measurement Information System (PROMIS) 4-item Short Forms to assess the frequency of symptoms of depression and anxiety “during the COVID-19 or coronavirus pandemic.” Responses for each ranged from 1 = never to 5 = always (range, 4-20; α = 0.89-0.94). 78,79 We converted scores to T scores standardized to the general US population (mean [SD], 50 [10]) to aid in the interpretation of results.
Covariates
Sociodemographic controls were age (in years), gender (man, woman), nativity (US-born, non–US-born), city (Atlanta, Chicago, Los Angeles, New Orleans, New York), relationship status (married/partnered, romantic relationship, single, separated/widowed/divorced), education (≤high school, some college/associate’s degree, bachelor’s degree, graduate degree), work status (employed full-time, employed part-time, unemployed, out of labor force), ratio of annual household income to poverty threshold ($5000 increments ranging from <$10 000 to ≥$100 000), and health insurance (private, public, other, none). We used the 5-item Social Desirability Response Scale to adjust for potential personality bias in responding to sensitive questions. 80 Example items included “I am always courteous even to people who are disagreeable” and “There have been occasions when I took advantage of someone” (range, 1 = definitely false to 5 = definitely true). We multiplied the total number of items endorsed with an extreme response in the direction of greater social desirability by 20 (range, 0-100). 80
Analyses
We excluded participants with missing data on any variable (Asian American: n = 3; Black American: n = 2), resulting in an analytic sample size of 604 Asian participants and 844 Black participants. We stratified analyses by race given the qualitatively unique sources and experiences of racism experienced by Asian and Black Americans during the COVID-19 pandemic. We used multivariable linear regression to examine depression and anxiety in relation to vicarious racism and vigilance, first separately and then together, controlling for covariates. We evaluated multiplicative effects of vicarious racism and vigilance by adding the corresponding interaction term. We standardized vicarious racism and racism vigilance within each race group and estimated standardized β coefficients for the main study variables. We conducted analyses using SAS version 9.4 (SAS Institute, Inc).
Results
Mean (SD) levels of depression and anxiety were 55.0 (10.2) and 58.5 (10.2), respectively, among Asian participants and 54.1 (10.6) and 57.0 (10.9), respectively, among Black participants (Table 1). Most (91.9%) Asian and (98.1%) Black participants reported experiencing any vicarious racism. About half (51.0%) of Asian participants and 61.6% of Black participants reported that experiences of vicarious racism during the COVID-19 pandemic were “more than usual.” Most participants reported that their personal experiences of racial discrimination were “the same” (62.3% and 63.7% among Asian and Black participants, respectively) or “less than usual” (11.9% and 15.9% among Asian and Black participants, respectively) during the COVID-19 pandemic.
Characteristics of Asian and Black participants in the Uncovering COVID-19 Experiences and Realities (UnCOVER) Study, May 21–July 15, 2020 a
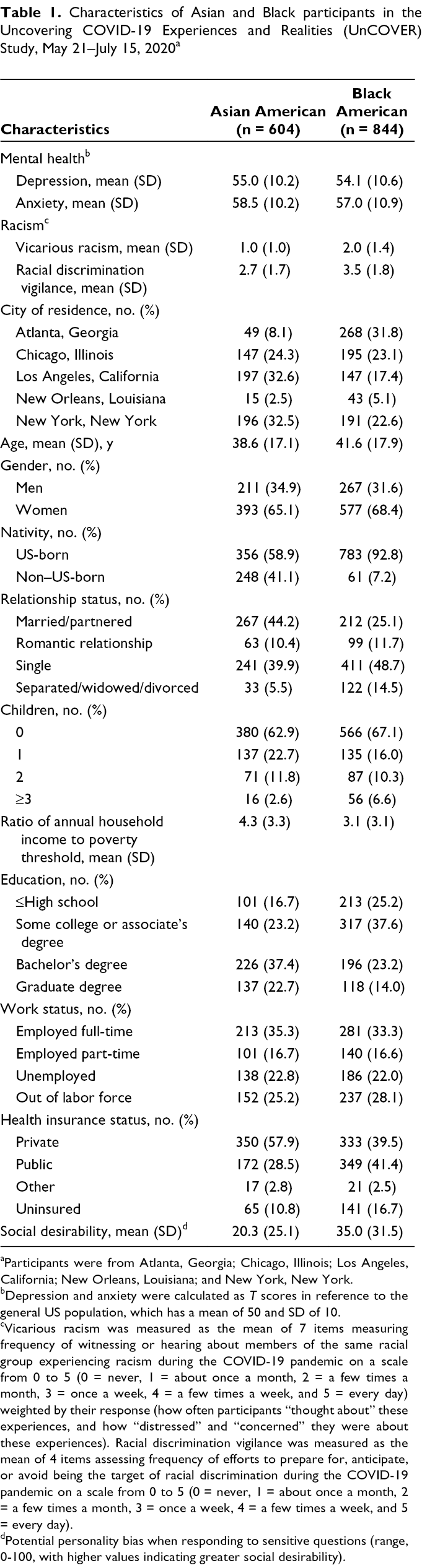
aParticipants were from Atlanta, Georgia; Chicago, Illinois; Los Angeles, California; New Orleans, Louisiana; and New York, New York.
bDepression and anxiety were calculated as T scores in reference to the general US population, which has a mean of 50 and SD of 10.
cVicarious racism was measured as the mean of 7 items measuring frequency of witnessing or hearing about members of the same racial group experiencing racism during the COVID-19 pandemic on a scale from 0 to 5 (0 = never, 1 = about once a month, 2 = a few times a month, 3 = once a week, 4 = a few times a week, and 5 = every day) weighted by their response (how often participants “thought about” these experiences, and how “distressed” and “concerned” they were about these experiences). Racial discrimination vigilance was measured as the mean of 4 items assessing frequency of efforts to prepare for, anticipate, or avoid being the target of racial discrimination during the COVID-19 pandemic on a scale from 0 to 5 (0 = never, 1 = about once a month, 2 = a few times a month, 3 = once a week, 4 = a few times a week, and 5 = every day).
dPotential personality bias when responding to sensitive questions (range, 0-100, with higher values indicating greater social desirability).
The mean (SD) frequency of vicarious racism experiences was 1.7 (1.3) among Asian participants, or experiencing each item between “once a month” and “a few times a month” on average. Among Black participants, the mean (SD) frequency of vicarious racism was 2.8 (1.3), or experiencing each item on average between “a few times a month” and “once a week.”
Among Asian participants reporting any vicarious racism, 72.8% reported thinking about these experiences at least “sometimes” (mean [SD] = 2.0 [1.0]), 89.6% said they were at least “somewhat” distressed (mean [SD] = 2.0 [1.1]), and 68.7% said they were concerned about these experiences “somewhat” or more (mean [SD] = 2.2 [1.2]). Corresponding numbers for Black participants were 87.2% (2.7 [1.1]), 91.2% (2.4 [1.3]), and 85.1% (2.8 [1.2]) for the same levels of thinking about experiences, feeling distressed, and being concerned, respectively. The overall effect of vicarious racism, calculated as the mean (SD) frequency multiplied by the response weight, was 1.0 (1.0) for Asian participants and 2.0 (1.4) for Black participants (Table 1).
Asian and Black participants were also vigilant about being the target of racial discrimination during the COVID-19 pandemic. Forty percent of Asian participants and 67.1% of Black participants reported experiencing at least one form of vigilance “about once a week” or more. The vigilance item with the highest mean frequency was “I fear that I will be discriminated against because I am [race]” among both Asian (mean [SD] = 2.8 [1.8]) and Black (3.8 [2.0]) participants. The overall mean (SD) vigilance score was 2.7 (1.7) among Asian participants, or experiencing each vigilance item between “a few times a month” and “once a week.” Among Black participants, the mean (SD) was 3.5 (1.8), or between “once a week” and “a few times a week” (Table 1).
In linear regression analyses, when examined separately, vicarious racism (Model 1) and vigilance (Model 2) showed positive bivariate relationships with symptoms of depression and anxiety among Asian participants (β = 3.75 [95% CI, 2.97-4.52] and β = 3.67 [95% CI, 2.90-4.44], respectively) and Black participants (β = 2.92 [95% CI, 2.23-3.62] and β = 2.78 [95% CI, 2.09-3.48], respectively) (Table 2). Examining vicarious racism and vigilance together attenuated effect estimates (Model 3), but both remained significantly associated with symptoms of depression and anxiety. Controlling for sociodemographic covariates did not result in substantively different conclusions (Model 4). In this model, each SD increase in vicarious racism was associated with a 1.92-point increase in depressive symptoms and a 2.40-point increase in symptoms of anxiety among Asian participants; each SD increase in vigilance was associated with a 1.54-point increase in depressive symptoms and a 1.98-point increase in symptoms of anxiety in this group. Among Black participants, corresponding values for symptoms of depression and anxiety associated with vicarious racism were 1.72 and 1.98 and for vigilance were 0.90 and 1.64, respectively. We did not find evidence of significant interactions between vicarious racism and vigilance for Asian or Black participants in any of the models.
Association among vicarious racism, racial discrimination vigilance, and mental health among Asian and Black participants aged ≥18 in the Uncovering COVID-19 Experiences and Realities (UnCOVER) Study, May 21–July 15, 2020 a
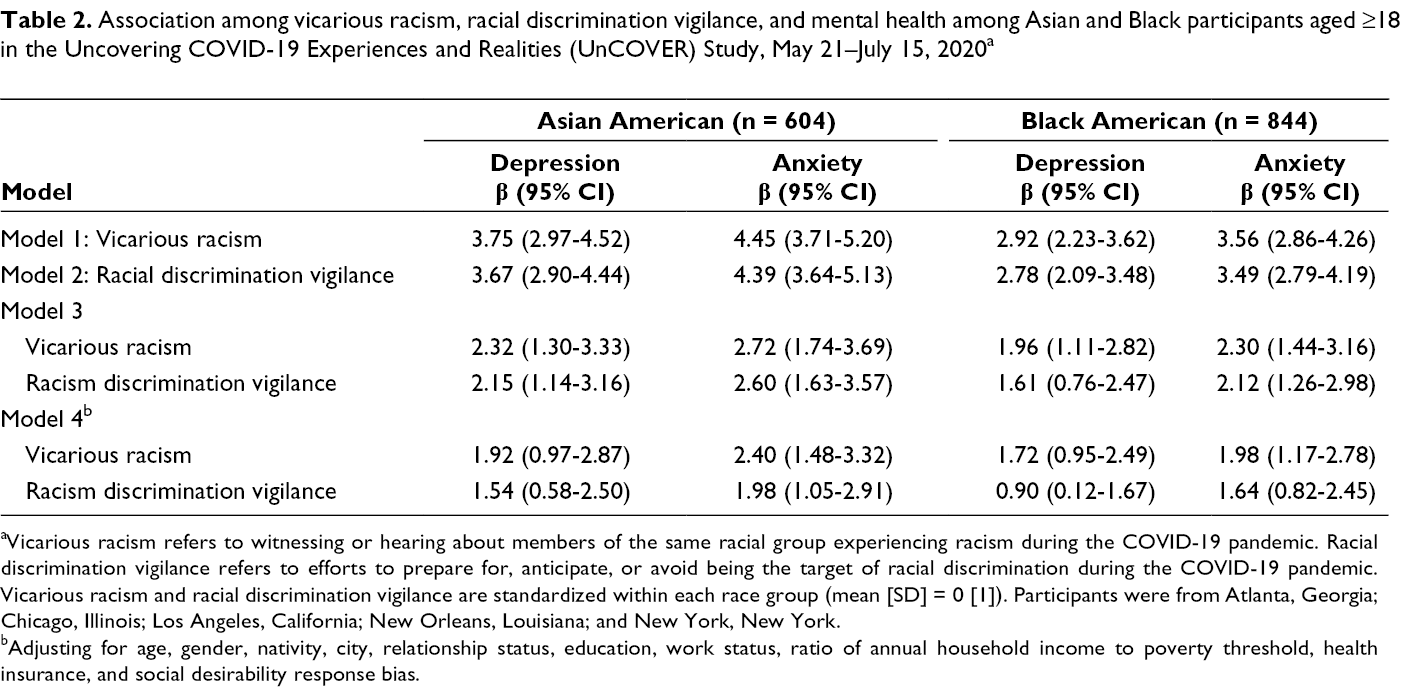
aVicarious racism refers to witnessing or hearing about members of the same racial group experiencing racism during the COVID-19 pandemic. Racial discrimination vigilance refers to efforts to prepare for, anticipate, or avoid being the target of racial discrimination during the COVID-19 pandemic. Vicarious racism and racial discrimination vigilance are standardized within each race group (mean [SD] = 0 [1]). Participants were from Atlanta, Georgia; Chicago, Illinois; Los Angeles, California; New Orleans, Louisiana; and New York, New York.
bAdjusting for age, gender, nativity, city, relationship status, education, work status, ratio of annual household income to poverty threshold, health insurance, and social desirability response bias.
Discussion
Numerous examples in US history demonstrate how acts of racism traumatize entire communities. Lynchings were part of a campaign of terror intended to spread fear, segregate, and suppress the advancement of Black Americans. 81 The Chinese Exclusion Act (1882)—the only major federal legislation focused on a nationality group—effectively prohibited all immigration from China. 82 Large-scale massacres of Chinese Americans ensued in subsequent years. 83 Modern instances of racism and xenophobia, including during the COVID-19 pandemic, also have collective injurious consequences.
Results from our study suggest that vicarious racism has been salient, being more frequent during (vs before) the COVID-19 pandemic among Asian and Black Americans. Such experiences were commonly thought about and considered to be sources of distress and concern. Large segments of Asian and Black Americans were also vigilant about being the target of racial discrimination during the COVID-19 pandemic.
Mental health problems constitute an important public health concern during the COVID-19 pandemic. One study estimated a 3-fold increase in the prevalence of depressive symptoms in the United States during (vs before) the COVID-19 pandemic. 84 Depressive symptoms among Asian American people increased more than 5-fold, from 4.4% to 23.1%. The US Census Household Pulse Survey consistently indicates that Black Americans have had the highest prevalence of depression and anxiety symptoms during the COVID-19 pandemic. 57,58 Our study indicates that experiences of vicarious racism and racism-related vigilance may contribute to increased mental health problems among both Asian and Black Americans. Increases in symptoms of depression and anxiety among Black Americans after the killing of George Floyd may be the result of vicarious racism and heightened vigilance. 57 Ruminative distress in response to witnessing racism and heightened attentiveness to avoid or prepare for personal victimization are psychologically demanding coping responses that increase the risk of depression and anxiety. 65,70,85
Limitations
This study had several limitations. First, the cross-sectional study design limited our ability to draw causal conclusions or infer directionality. For example, poorer mental health may have resulted in greater attentiveness to racism. Unmeasured confounders, such as economic trends, increased unemployment, and rises in racially charged violence, could have driven observed associations. Second, the data collection period was also characterized by increasing numbers of COVID-19 cases, hospitalizations, and deaths and widening racial health inequities, which co-occurred with increases in vicarious racism and racial discrimination vigilance; these unmeasured confounders could have driven the associations we found with mental health. Third, the generalizability of our findings is limited by a focus on only 5 US cities and the self-selected nature of participants and sampling. However, this limitation was counterbalanced by the large sample size and the relatively short recruitment period, which enabled us to obtain a snapshot of how people’s experiences during the COVID-19 pandemic were shaped by race and how racism-related experiences during this moment were related to mental health. Fourth, we did not assess clinically significant depression or anxiety but, rather, symptom levels, thereby limiting inferences about diagnostic risk. Regardless, the PROMIS short-form measures of depression and anxiety are valid and reliable across diverse populations and perform similarly to diagnostic interviews. 79 Fifth, we did not assess parameters of vigilance other than frequency, such as chronicity, duration, severity, or appraisal, which may be conceptually important moderators. Finally, our measures of vicarious racism and vigilance, although based on previously developed scales, have not been widely tested, and their validity and reliability have not been established. 86,87
Conclusions
Our findings are largely concordant with previous research and consistent with experimental studies that have manipulated exposure related to viewing racist events. 37,49,59,88 Taken together, these studies point to the negative health consequences of vicarious racism. Our findings are also aligned with studies that found that racism-related vigilance is psychologically taxing and may result in depression and anxiety. 64,70 Future studies may expand this research to a wider range of mental health outcomes, such as posttraumatic stress disorder, and examine associations in other groups susceptible to racism during the COVID-19 pandemic. Our study contributes to evidence that racism during the COVID-19 pandemic led to increased levels of depression and anxiety in Asian and Black communities. 31,57,89,90 This research highlights racism as a social toxin that has widespread adverse health effects. Leadership at various levels, institutions, and settings should address traumatic racist events, including their implications for mental health. Antiracism policies and practices should be implemented across institutional settings, as a social and moral imperative, and as part of a public health strategy. 91,92
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.