
Abstract
A wealth of coping skills for psychological resilience in the face of everyday stressors becomes pivotal during a global pandemic with physical, social, and societal impacts. The present analyses examined the relationship between coping strategies, pandemic-related distress during early phase COVID-19, and clinical symptoms of depression and anxiety. Data were collected via online survey from a sample of adults diverse in age, ethnicity, sexual orientation, gender, population density, education, disability status, and economic status, all living within the United States (N = 594). Cognitive distortions, mindful nonjudgment, perceived availability of social support, and locus of control significantly mediated the relationship between pandemic distress and clinical symptoms of both anxiety and depression. Multiple regressions explained substantial variance in symptoms of depression (47%) and anxiety (52%) among participants, predominately via mindfulness skills, followed by locus of control. Overall, mindful awareness and mindful nonjudgment emerge as most associated with resilience to pandemic-related distress.
Introduction
Since first reports of the Severe Acute Respiratory Syndrome coronavirus two (SARS-CoV-2) in December 2019, both the virus itself and sociopolitical responses to it have had lasting effects on health. The stress of the pandemic caused increased rates of anxiety, depression, and various mental health symptoms internationally (e.g. Robinson et al., 2022). The majority of the population carried a risk factor for poorer mental health outcomes during the pandemic: female gender, lower socioeconomic status, working as a frontline healthcare worker, high medical risk of contracting the virus, or notably, social isolation (Luo et al., 2020). Indeed, longitudinal data showed that mental health and well-being worsened significantly when lockdowns first began in March 2020 (Robinson et al., 2022). The present study sought to explore early factors in resilience; how to best cope with the stress of an unprecedented, restrictive pandemic.
Ways of coping
Coping is commonly defined in the literature as an individual’s efforts to minimize experienced stress - the burden of accommodations to either positive or negative disruptions (Carver, 2013). It has been conceptualized via several overlapping frameworks. Cognitive and behavioral coping models separate out purely cognitive emotion regulation strategies that can occur in one’s mind (e.g. rumination or putting things into perspective; Garnefski and Kraaij, 2006) from effortful behavioral strategies (e.g. incorporating new routines or seeking social support; Lazarus and Folkman, 1984). Emotion-focused and problem-focused coping models differentiate coping skills meant to manage the emotional response (e.g. venting, denying, seeking social support) from those that solve or reduce the stressor or problem itself (Baker and Berenbaum, 2007). The approach-avoidant coping model contrasts avoidant coping strategies like distraction, escape, and substance use – noted as quite effective when the stressor is out of one’s control – with strategies that approach and solve root problems (Roth and Cohen, 1986). Rarely are any of these overarching categories of coping found to be holistically good or bad.
Mindfulness
Mindfulness skills can be engaged in cognitively (i.e. via shifting focus or thought patterns), as well as behaviorally (e.g. a sitting or walking meditation practice). Mindfulness skills are typically a daily or weekly practice, neither emotion or problem-focused, nor avoidant. They do not fit neatly into the popular models for coping. As mindfulness expert Jon Kabat-Zinn writes, “mindfulness means paying attention. . . on purpose, in the present moment, and nonjudgmentally” (Kabat-Zinn, 2001, p. 24). Research has revealed mindfulness to be a jack-of-all-trades for cognitive, behavioral, emotional, social, and even epigenetic benefits, with proven efficacy treating anxiety, depressive, and eating disorders, addiction, and beyond (Keng et al., 2011, for review).
COVID-19 and coping
Narrative synthesis on infectious disease outbreaks such as Ebola, H1N1, and SARS helps to situate COVID-19 within a broader history of universal outbreak-related coping trends like problem-solving, avoidance, and seeking social support (Chew et al., 2020). Even the earliest research on coping during COVID-19 is aligned: social support is most universally connected to benefits (e.g. Chew et al., 2020; Ogueji et al., 2022; Tuason et al., 2021), and the positive appraisal skill of meaning-making predicted physical and mental health across 30 countries (Eisenbeck et al., 2022).
Longitudinal research also supports the role of coping during COVID-19, for example, with mindfulness skills (e.g. Götmann and Bechtoldt, 2021) and family resilience (e.g. Li et al., 2025) related to greater well-being and self-efficacy, and socially-supportive coping skills related to improvements in depression and anxiety over time (Fluharty and Fancourt, 2021). It may be that mindfulness, family resilience, and social coping skills are serving to mediate the impact of COVID-19 stressors on psychological health. Of note, Fluharty and Fancourt’s (2021) longitudinal sample from the United Kingdom found avoidant coping more associated with low socioeconomic status, while emotion-focused coping was associated with both greater education achievement and mental health, highlighting the role of privilege or access to resources.
Much of the newly robust literature on coping during the pandemic focuses on the same major frameworks of coping that predate the COVID-19 pandemic. While some reviews highlight international coverage (e.g. Cheng et al., 2024), many deeper investigations are tightly limited by populations of convenience during the pandemic. For example, meta-analyses of mindfulness-based interventions show clear improvement in anxiety and resilience in college students – whether learned and practiced digitally or otherwise (Deep et al., 2025) – as well as significant improvement in anxiety and depression in healthcare professionals when including some face-to-face component (Benavides-Gil et al., 2024).
The present study
The present study contributes to existing literature by combining mediation and regression analyses with a broader multi-factor assessment of coping skills than previous research, as well by assessing pandemic-related distress independently from clinical symptoms of anxiety and depression. Furthermore, to identify more universal trends in coping and distress, the sample collected was diverse in age, ethnicity, sexual orientation, gender, population density, education, disability status, and economic status. Understanding how diverse and intersectional populations are affected by pandemic disruption is crucial, because socioeconomic crises exacerbate preexisting disparities in American minority groups (Brooks et al., 2022; Ruprecht et al., 2021; Snowden and Snowden, 2021).
Methods
Participants
Data cleaning reduced the initial 643 online survey submissions to the final sample of 594 participants between the ages of 18 and 78 (M = 35.00; SD = 15.42) who lived in the United States at the time of sampling during the summer of 2020 (Table 1).
Frequency distributions for demographics (N = 594).
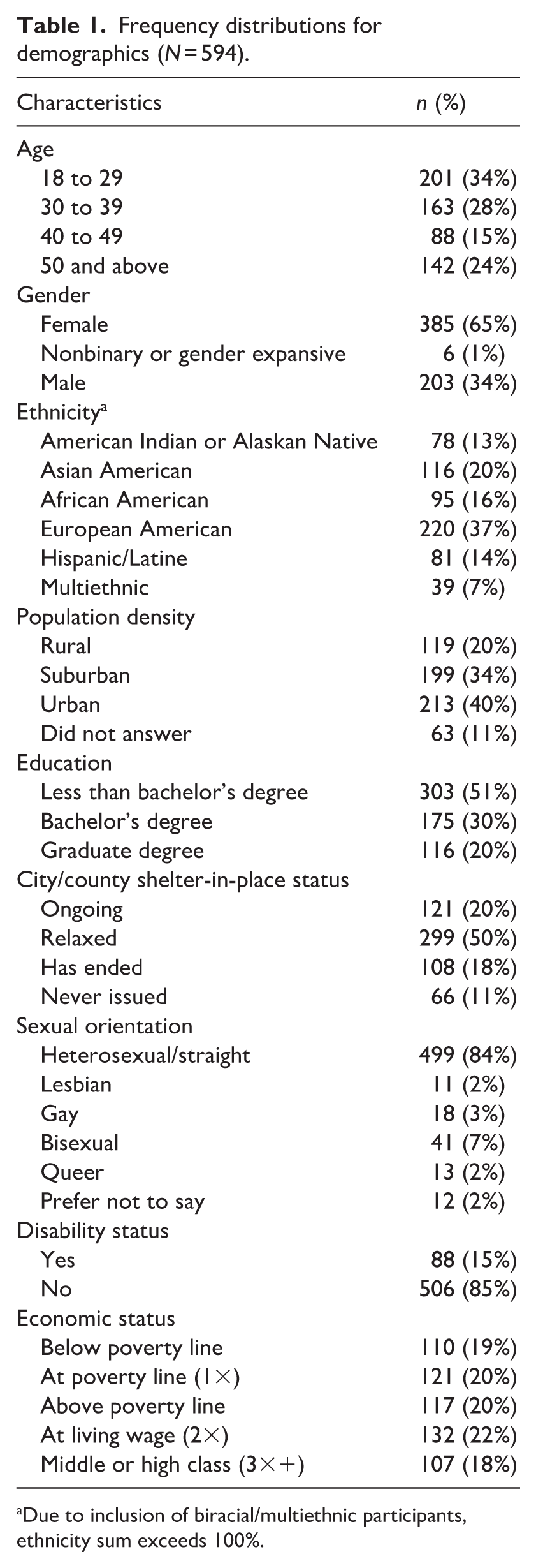
Due to inclusion of biracial/multiethnic participants, ethnicity sum exceeds 100%.
Procedure
Participants were recruited via online and paper channels, including Qualtrics’ participant pool, which compensated respondents with two to three dollars. Recruitment terminated once the demographics minimum quota of 70 was met for all key analyses. After providing informed consent, participants completed the survey online in English, in approximately 20–27 minutes.
Measures
Assessing use of coping skills
Brief coping orientation to problems experienced inventory-18 (Brief COPE-18)
The Brief COPE-18 (Carver, 1997) is an 18-item abbreviation of the 28-item original, and measures the frequency of coping styles and strategies in adults. Participants rate their frequency of engagement in each coping strategy described on a four-point Likert scale, with higher scores indicating more engagement (1 = I haven’t been doing this at all; 4 = I’ve been doing this a lot). The present study utilized a nine-subscale version of the Brief COPE based on Carver’s (1997) analyses (0.50 < α < 0.97 per Snell et al., 2011).
Brief-COPE factor analysis
For the present study, the 18 items of the Brief-COPE were subjected to an exploratory factor analysis. The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.85 (exceeding the recommended value of 0.6; Kaiser and Rice, 1974), and Bartlett’s test of sphericity was statistically significant (p < 0.001), suggesting the factorability of the correlation matrix. While scree plot inflection points suggested two or three factors, both examination of Eigenvalues greater than one and the factor matrix supported the extraction of two factors.
When two factors were extracted, 15 items loaded highly onto one of the two factors while 4 items did not load onto either item (including both Religious Coping items). This final solution accounted for 42.98% of total variance. Factor 1 was comprised of nine items (the subscales of Self-Distraction, Active Coping, Planning, Acceptance, and half of Use of Emotional Support), and accounted for 31.81% of the variance. Factor 1 was named Active Coping, as the items were characterized by productive efforts to change the problem itself or one’s way of thinking about the problem. Factor 2 was comprised of 5 items (the subscales of Denial, Humor, and half of Venting), and accounted for 11.18% of the variance. Factor 2 was named Avoidant Coping as it involves measures taken to deny or distract oneself from the problem.
The overall internal consistency was very strong (α = 0.87). Similarly, the Cronbach’s alphas for Factor 1 and Factor 2 were 0.82 and 0.76, respectively. The two factors were found to be internally consistent in that they were significantly positively moderately correlated (r = 0.55).
Cognitive emotion regulation questionnaire-18 (CERQ-18)
The CERQ-18 (Garnefski and Kraaij, 2006) assesses a participant’s cognitive strategies of emotion regulation in response to negative events. The CERQ-18 is an 18-question abbreviation of the 36-question original. Participants indicate the frequency of engagement with each strategy on a five-point Likert scale (1 = (almost) never; 5 = (almost) always). For the nine subscales, Cronbach’s alphas range from 0.68 to 0.81.
CERQ-18 factor analysis
For the present study, all 18 items of the CERQ-18 were subjected to an exploratory factor analysis. The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.87, and Bartlett’s test of sphericity was statistically significant (p < 0.001), suggesting the factorability of the correlation matrix. While scree plot inflection points suggested two or three factors, both examination of Eigenvalues greater than 1 and the factor matrix supported the extraction of two factors.
When two factors were extracted, all items loaded highly onto one of the two factors. This final solution accounted for 46.27% of total variance. Factor 1 was comprised of 11 items (the subscales of Acceptance, Positive Reappraisal, Positive Refocusing, Refocus on Planning, and Putting Into Perspective), and accounted for 33.38% of the variance. Factor 1 was named Psychological Flexibility in that it reflects an acceptance-based and adaptive response to the situation. Factor 2 was comprised of seven items (the subscales of Self Blame, Catastrophizing, and Other Blame), and accounted for 12.89% of the variance. Factor 2 was named Cognitive Distortions, as it reflects a tendency to catastrophize and blame distress on oneself and others. The remaining CERQ subscale, Rumination, was split evenly between these two factors.
The total scale had very good internal consistency (α = 0.88). Similarly, the Cronbach’s alphas for Factor 1 and Factor 2 were 0.86 and 0.83, respectively. Both factors were significantly positively moderately correlated (r = 0.48), suggesting they measure similar constructs, and demonstrating adequate internal consistency.
Fifteen-item five-factor mindfulness questionnaire (FFMQ-15)
The FFMQ-15 (Baer et al., 2012) is an abbreviation of the 39-question original, and assesses mindfulness through 15 items divided into five subscales: Observing, Describing, Acting with Awareness, Non-judgment, and Non-reactivity. Participants rate their frequency of practice of mindfulness skills with a five-point Likert scale (1 = never or very rarely true; 5 = very often or always true). The FFMQ-15 was selected because it evaluates mindfulness use and fidelity consistent with therapeutic intervention or otherwise informed practice over time. The FFMQ-15 has adequate reliability and validity (0.64 ⩽ α ⩽ 0.80; Gu et al., 2016).
Interpersonal support evaluation list (ISEL)
The ISEL measures how the participant perceives the types of social support available to them (Cohen et al.,1983). It consists of 12 items divided into 3 subscales, where participants indicate the accuracy of each item on a four-point Likert scale (0 = definitely false; 3 = definitely true). Sums can be calculated for the total measure, with higher scores for stronger perceived social support. The ISEL has reported alphas of 0.88–0.90 in the general population.
Locus of control (LOC)
LOC refers to the degree of control individuals feel they have over their lives. It was measured with a single seven-point Likert scale question: “How much control do you feel you have over your own life?” (1 = no control; 7 = complete control), where a higher score indicated a more internal LOC. The use of this question as a single-item measure of LOC is a limitation, though precedented by Helmick (1980) and found by Bugaighis and Schumm (1983) to correlate well with other full-length subscales (α > 0.40).
Assessing psychological distress
Screen for child anxiety related emotional disorders for adults (SCARED-A)
The SCARED-A (Van Steensel and Bögels, 2014) is a 71-item adult adaptation of the SCARED measure of symptoms of anxiety disorders. Participants rate their frequency of anxiety symptoms using a three-point Likert scale (0 = almost never; 2 = often) with higher scores indicating greater likelihood of meeting criteria for an anxiety disorder. The SCARED-A has strong convergent validity and a Cronbach’s alpha of 0.94 (Van Steensel and Bögels, 2014). For the present study, only the Panic (α = 0.85), Generalized Anxiety Disorder (α = 0.88), Social Anxiety Disorder (α = 0.88), and Obsessive-Compulsive Disorder (α = 0.71) subscales were used, which resulted in 44 questions (Van Steensel and Bögels, 2014).
Center for epidemiologic studies depression scale revised short form (CESD-R-10)
The CESD-R-10 (Miller et al., 2008) is 10-item abbreviation of the CESD-R, a self-report depression screener. Participants rate the frequency of DSM-5 symptoms of major depressive disorder on a five-point Likert scale (0 = not at all or less than one day; 4 = nearly every day for 2 weeks), with higher scores indicating greater likelihood of meeting criteria for a major depressive episode. The CESD-R-10 has strong validity and a Cronbach’s alpha of 0.86 (Miller et al., 2008).
COVID-19 pandemic distress scale (C19PDS)
The C19PDS is a self-authored measure created to assess how stressed or distressed the participant is by changes in their daily life due to the pandemic and concerns around the virus itself. It consists of 24 items that fall into two subscales, Disconnection/Restriction (DR) and Health Fears and Uncertainty (HFU). Items are scored on a five-point Likert scale (0 = not at all bothered; 4 = incredibly bothered), where higher scores indicate greater pandemic-related distress. Psychometric analyses showed strong internal consistency for the overall measure (α = 0.93), DR subscale (α = 0.92) and HFU subscale (α = 0.88). While many measures of distress during pandemics are tacitly clinical in nature, the C19PDS differentiates itself by assessing everyday stress and distress even before or beyond clinical intensity or duration. The C19PDS subscales have only small to medium correlations with the SCARED-A subscales and CESD-R-10, demonstrating discriminant validity (Brooks et al., 2022).
Results
Correlations
Table 2 illustrates the partial correlations of all study variables when controlling for age, with the exception of the age column itself, which displays simple correlations.
Partial correlation matrix controlling for age.
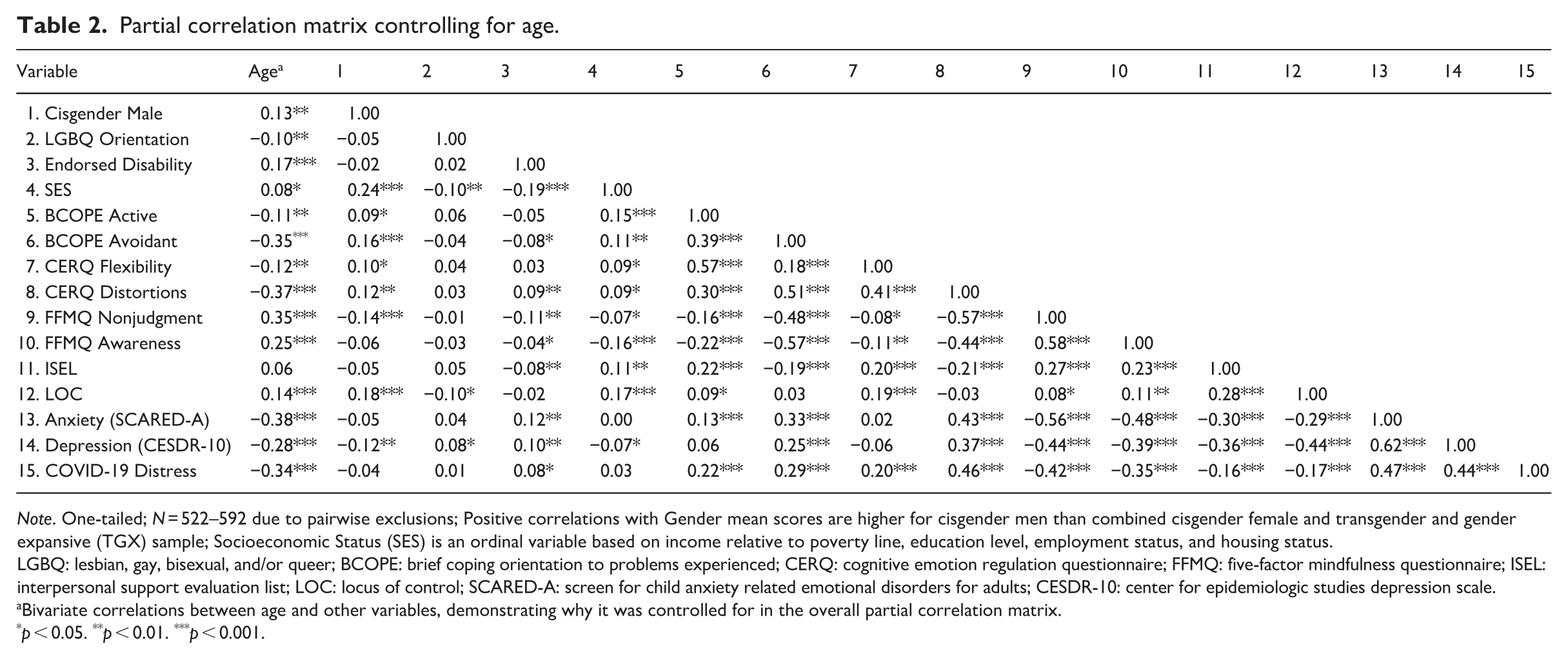
Note. One-tailed; N = 522–592 due to pairwise exclusions; Positive correlations with Gender mean scores are higher for cisgender men than combined cisgender female and transgender and gender expansive (TGX) sample; Socioeconomic Status (SES) is an ordinal variable based on income relative to poverty line, education level, employment status, and housing status.
LGBQ: lesbian, gay, bisexual, and/or queer; BCOPE: brief coping orientation to problems experienced; CERQ: cognitive emotion regulation questionnaire; FFMQ: five-factor mindfulness questionnaire; ISEL: interpersonal support evaluation list; LOC: locus of control; SCARED-A: screen for child anxiety related emotional disorders for adults; CESDR-10: center for epidemiologic studies depression scale.
Bivariate correlations between age and other variables, demonstrating why it was controlled for in the overall partial correlation matrix.
p < 0.05. **p < 0.01. ***p < 0.001.
Regression analyses
The prediction of depression and anxiety as outcome variables was examined by conducting two separate hierarchical multiple regressions. Participants missing demographic variables utilized in analyses were excluded from analyses, with final inclusions reflected in the degrees of freedom for each analysis. All assumptions for multiple regression analyses were analyzed and met.
After accounting for demographic variables (age and gender) in Step 1, the predictive value in explaining the variance in depression and anxiety was assessed with variables: Nonjudgement and Acting with Awareness (Step 2), Locus of Control (Step 3), Psychological Flexibility and Cognitive Distortions (Step 4), Interpersonal Support (Step 5), and Active Coping and Avoidant Coping (Step 6).
Concerning depression, as measured by the CESDR-10, all statistically significant predictors explained 47.3% of the variance in the sample (F (2, 505) = 11.53, p < 0.001). Statistically significant increases in R² were observed with the addition of Nonjudgement, Acting with Awareness, Internal LOC, CERQ Psychological Flexibility, CERQ Cognitive Distortions, and Interpersonal Support after accounting for age and gender. While age and gender accounted for 9% of the variance (F (2, 513) = 25.13, p < 0.001), Acting with Awareness and Nonjudgement accounted for 22% (F (2, 511) = 81.22, p < 0.001) and Locus of Control accounted for 13% (F (1, 510) = 112.48, p < 0.001). Psychological Flexibility and Cognitive Distortions accounted for 2% (F (2, 508) = 10.73, p < 0.001) of the variance when entered on Step 4 and Interpersonal Support accounted for just 1% (F (1, 507) = 11.53, p < 0.001) of the variance at Step 5. The addition of Active and Avoidant Coping at Step 6 did not significantly increment the predictive power for depression.
Concerning anxiety, as measured by the SCARED-A, all statistically significant predictors explained 51.7% of the variance in the sample (F (2, 505) = 4.61, p < 0.05). Demographic variables entered at Step 1 (age and gender) accounted for 15% of the variance (F (2, 513) = 44.77, p < 0.001), while Acting with Awareness and Nonjudgement accounted for 31.4% (F (2, 511) = 149.26, p < 0.001). At Step 3, Locus of Control accounted for 3% (F (1, 510) = 35.39, p < 0.001) of the variance while Psychological Flexibility and Cognitive Distortions accounted for 1% (F (2, 508) = 6.33, p = 0.002) when entered at Step 4. Finally, Interpersonal Support accounted for less than .01% (F (1, 507) = 4.61, p = 0.03) of the variance at Step 5. The addition of Active and Avoidant Coping at Step 6 did not significantly predict anxiety.
Mediation analyses
Coping strategies were analyzed as potential mediators of the relationship between pandemic distress and mental health outcomes with Hayes’ (2013) Macro PROCESS via the bootstrapping method. Analysis evaluated the indirect effect of pandemic distress on the mental health outcome variables via a coping skill, which is interpreted as statistically significant if its 5000 bootstrap sample bias-corrected 95% confidence interval excludes zero (Hayes, 2013). Mediation analyses were conducted to determine whether the relationships between pandemic related distress and depression or anxiety were mediated by coping responses to COVID-19 (Supplemental Figure 1). Significant direct and indirect effects were observed between pandemic distress and mental health outcomes. Consistent with regression analyses, pandemic distress retained direct relationships with depression and anxiety when accounting for coping responses. Psychological flexibility, cognitive distortions, mindful nonjudgement, interpersonal support, and locus of control partially mediated the relationship between pandemic distress and symptoms of clinical depression (Table 3). Cognitive distortions, mindful nonjudgement, mindful awareness, interpersonal support, and locus of control partially mediated the relationship between pandemic distress and symptoms of clinical anxiety (Table 4).
Coping skills mediating the relationship between pandemic distress and depression.
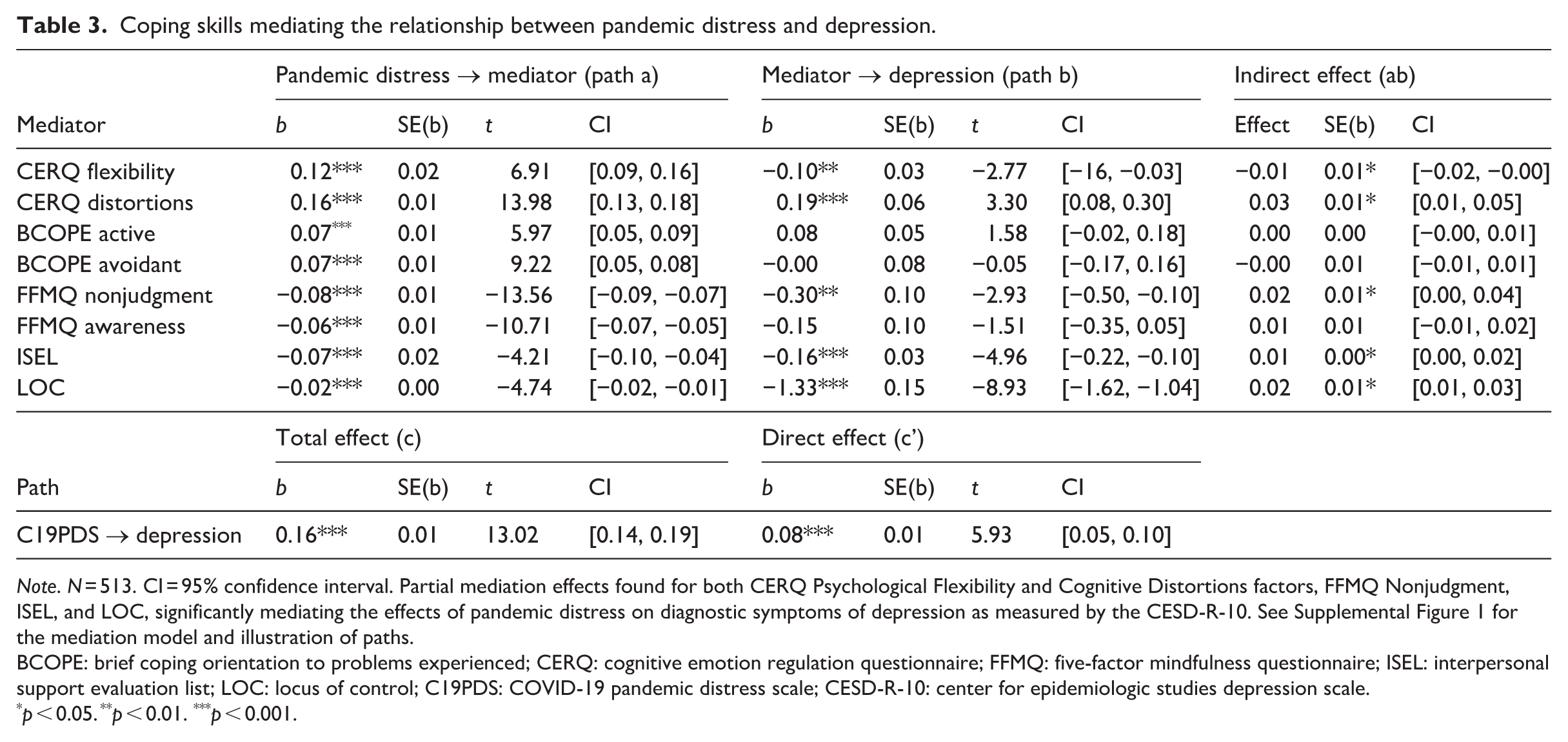
Note. N = 513. CI = 95% confidence interval. Partial mediation effects found for both CERQ Psychological Flexibility and Cognitive Distortions factors, FFMQ Nonjudgment, ISEL, and LOC, significantly mediating the effects of pandemic distress on diagnostic symptoms of depression as measured by the CESD-R-10. See Supplemental Figure 1 for the mediation model and illustration of paths.
BCOPE: brief coping orientation to problems experienced; CERQ: cognitive emotion regulation questionnaire; FFMQ: five-factor mindfulness questionnaire; ISEL: interpersonal support evaluation list; LOC: locus of control; C19PDS: COVID-19 pandemic distress scale; CESD-R-10: center for epidemiologic studies depression scale.
p < 0.05. **p < 0.01. ***p < 0.001.
Coping skills mediating the relationship between pandemic distress and anxiety.
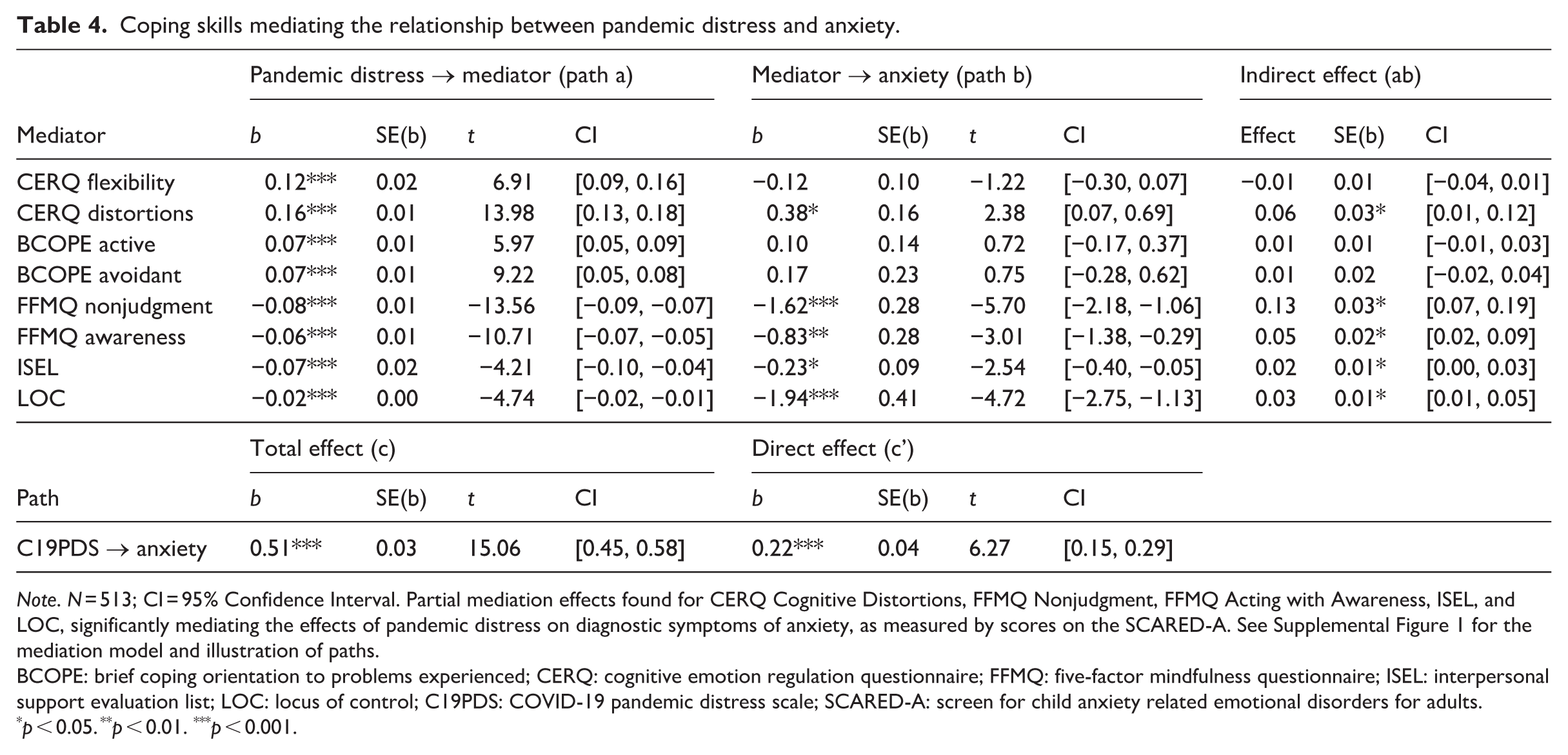
Note. N = 513; CI = 95% Confidence Interval. Partial mediation effects found for CERQ Cognitive Distortions, FFMQ Nonjudgment, FFMQ Acting with Awareness, ISEL, and LOC, significantly mediating the effects of pandemic distress on diagnostic symptoms of anxiety, as measured by scores on the SCARED-A. See Supplemental Figure 1 for the mediation model and illustration of paths.
BCOPE: brief coping orientation to problems experienced; CERQ: cognitive emotion regulation questionnaire; FFMQ: five-factor mindfulness questionnaire; ISEL: interpersonal support evaluation list; LOC: locus of control; C19PDS: COVID-19 pandemic distress scale; SCARED-A: screen for child anxiety related emotional disorders for adults.
p < 0.05. **p < 0.01. ***p < 0.001.
Discussion
This research found that mindfulness skills and locus of control powerfully predicted adults’ clinical symptoms of anxiety and depression during early-phase COVID-19. This held true even while controlling for their pandemic distress due to health risks, health anxiety, grief over loss of life, and the stress of uncertainty and disruption to daily rhythms during personal and governmentally mandated public health precautions. Age, gender, and a constellation of six high-powered coping strategies were able to explain about half of the variance in subjects’ anxiety and depression scores, more than double what pandemic distress scores alone explained. Analyses suggest it is not the stress itself, but how we respond to it and who we are, that impacts our mental health.
Age was a surprising negative correlate to pandemic distress in that older research subjects with greater health risks reported, on average, less distress during early phase COVID-19 and shelter-in-place restrictions than young people. This is replicated in other research, which some have interpreted as a result of young people’s need for cross-household mobility for social fulfillment, identity development, and to form new romantic connections; older people are more likely to have family as well as romantic connections within one household already (Levitt et al., 1993). Future public health policy and pandemic planning could take this into account to preserve the social development of young people.
The factors of cognitive distortions, mindful nonjudgment, perceived availability of social support, and locus of control (LOC) significantly mediated the connection between pandemic stress/distress and clinical symptoms of both anxiety and depression. More specifically, increases in cognitive distortions strengthened the relationship between pandemic distress and anxiety, while increases in mindful nonjudgement, mindful awareness, interpersonal support, and internal LOC weakened the effect. In addition, increases in cognitive distortions strengthened the relationship between pandemic distress and depression, while increases in psychological flexibility, nonjudgement, interpersonal support, and LOC weakened the effect. These cognitions and behaviors may serve as resilience and vulnerability factors impacting the extent to which stress is translated into clinical symptoms of psychological distress.
Mindfulness skills surpassed other coping approaches, predicting about a quarter of the variance in symptoms of depression and about a third of the variance in symptoms of anxiety in our sample. Mindful nonjudgment was particularly associated with psychological health. An internal LOC was also significantly related to better psychological health, as well as psychological flexibility and social support, in line with past research (Bachem et al., 2020). While there are many legitimate paths to resilience, some may be more direct than others.
In addition, psychological flexibility was found to mediate only the relationship between pandemic distress and depression, with lower average scores in depression for participants who had actively practiced acceptance, positive reappraisal, perspective-taking, and planning ahead in recent weeks. This held true even when controlling for levels of pandemic distress. It is not surprising that this factor of practical flexibility could be protective against depression; these skills overlap with psychotherapy interventions such as behavioral activation and Acceptance and Commitment Therapy, approaches with strong track records in treating chronic and recurrent depressive disorders (e.g. Kanter et al., 2006).
In parallel, mindful awareness was found to mediate only the relationship between pandemic distress and anxiety. Participants who had actively practiced mindful awareness in recent weeks had lower average scores in anxiety. It may be that mindful awareness has an effect in reducing the physiological reactivity or hypervigilance underlying many anxiety and worry disorders (e.g. Blanck et al., 2018).
Coping and resilience in the global majority
Because this sample is racially and ethnically diverse, ratings of subjects within racial and ethnic minorities may also be related to racist or xenophobic COVID-19 policies and rhetoric, or exacerbation of pre-pandemic racism-based distress (e.g. Devakumar et al., 2020). While the pandemic exacerbated stressors for marginalized groups, some also may possess resilience and coping skills forged through prior experiences of overcoming adversity. A previous analysis of the present data that examined the differential impact of COVID-19 based on social location found that African American identity had a uniquely positive association with protective internal locus of control (Brooks et al., 2022). Despite experiencing disproportionate effects of COVID-19, African American research subjects often exhibit higher levels of hope, resilience, and posttraumatic growth than their white European American counterparts (e.g. Willey et al., 2022). Litam et al. (2021) also found high levels of both discrimination and stress-related growth in an Asian, Asian American, and Pacific Islander sample during COVID-19, most strongly in those who sought psychotherapy. Future research could further explore unique coping trends by ethnicity, or evaluate cultural adaptation of coping interventions, which some suggest is the key to effectively disseminating mindfulness benefits via public health campaigns (Oman, 2025).
Strengths and limitations
The robust diversity of the present sample captured subcultures in the United States at the cost of purely simple random sampling. That and sample size are the main limitations of the study, limiting the number of factors that could be included in adequately-powered analyses. Capturing a broad range of coping strategies and experiences uniquely relevant to early-phase COVID-19 with “lockdown” restrictions was a value-add. However, this required the use of a novel measure for pandemic-related distress, which is a limitation due to its lack of external validation. Similarly, using a validated scale rather than a single item for locus of control would enhance construct validity in future research. The cross-sectional design was neither a strength nor a limitation. Participants were asked to draw upon the past couple of weeks when reporting their coping strategies and their distressed, sad, and anxious mood or symptoms. This allowed for analyses to focus on the short-term relationship between coping strategies and state anxiety or state depression, as is relevant to acute treatment efforts.
Clinical implications
The present results suggest that therapy interventions teaching and practicing mindful nonjudgment, increasing social support or the awareness thereof, facilitating an internal LOC, and reducing cognitive distortions, all carry potential psychological gains. Reducing blame would likely have beneficial effects on the broader community as well as within the individual (Bouguettaya et al., 2022). These appear relevant for resilience to both anxiety and depression, and hence may impact transdiagnostic processes driving other clinical symptoms as well (Harvey et al., 2004). Evidence is strong that practicing mindfulness skills is an impactful intervention to improve moment-to-moment resilience in the face of pandemic-related stress, and may reduce the likelihood of mental illness in the face of stress broadly (e.g. Antonini Philippe et al., 2021).
The power and impact of mindfulness when compared with a compendium of other coping strategies suggests that the teaching of coping skills could begin with mindfulness as a foundation. This is a concept long-practiced in Dialectical Behavioral Therapy (Linehan, 2015) and Mindfulness-Based Stress Reduction. These interventions can even be delivered asynchronously: while apps show mixed results, an 8-week online mindfulness-based intervention program designed specifically for COVID improved life satisfaction and decreased psychological distress in 100 adults (Ogino et al., 2024). Mindfulness skills are easily taught in individual and group settings at any age, and could be a vital tool to add to our standard schooling repertoire. Many well-developed training modules such as Mindful Schools are already in circulation (e.g. Smith et al., 2012), and have proven efficacy for low-income and ethnically diverse populations (Black and Fernando, 2014). This investment could lead to impressive results in how future generations cope. The broadest possible implication of this study is that incorporating mindfulness into public health campaigns and intervention efforts at all levels could be very fruitful in decoupling the stress of any large-scale disruption from clinical distress.
Conclusion
The broad findings of the present study illustrate the power of utilizing coping strategies across multiple domains: cognitive, emotional, social, self-evaluative (e.g. locus of control), and mindfulness based. Together, these factors explain a substantial portion of variance in symptoms of depression and anxiety during a pandemic. It could be that one of the main benefits of mindfulness is rooted in its resistance to categorization within the standard coping frameworks. Because mindfulness centers on a way of intentional being and responding to the world around and inside of a person, any other coping skill or strategy can be done more or less mindfully. Mindfulness may moderate the impact and efficacy of selected coping strategies (Zandi et al., 2021), which could explain how two mindfulness facets in the present regression analyses outperformed all other coping approaches. In this light, mindfulness emerges as a kind of lens that may magnify the power of other coping efforts, or rather, one skill to enhance them all.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261415744 – Supplemental material for One skill to rule them all? Coping strategies as mediators of depression and anxiety during early COVID-19
Supplemental material, sj-docx-1-hpq-10.1177_13591053261415744 for One skill to rule them all? Coping strategies as mediators of depression and anxiety during early COVID-19 by Cyrano Patton, Liya Levanda, Jordan Brooks, Amy Perez, Travis Salle, Jeraca Gayle and Huda Ajaz in Journal of Health Psychology
Footnotes
Ethical considerations
This study was approved by the Alliant International University Institutional Review Board (Protocol #2004176143A001).
Consent to participate
Written consent was attained.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Alliant Educational Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.