
Abstract

With national suicide rates on the rise by 35% since 1999 and concern that rates may be further exacerbated by the COVID-19 pandemic, 1 -3 suicide is a critical public health problem demanding the attention of public health agencies, especially at the local level. 4 -6 Yet, most suicide surveillance data are focused on state trends and often are not granular enough to inform local risk factors or be actionable by local officials. 2,7 This lack of county data may hinder the targeting of resources to communities or subpopulations at high risk for suicide where intervention may have the greatest effect. However, to our knowledge, 3 studies have been published in the past 2 years that examined county-level trends in suicide, suggesting that data can be used to identify localities with a high prevalence of suicides where prevention efforts can be focused. 8 -10 This approach is similar to the targeted, county-level approach that is used to combat other public health threats, such as HIV and the opioid epidemic. 11 -13 In this commentary, we examine literature on county trends in suicide and present our own findings from a brief county-level analysis using national data. We then outline opportunities for states to focus on county-level data and partner with local health departments (LHDs) to design data-driven and community-based approaches to suicide prevention.
Community-Based Approaches to Suicide Prevention
Local approaches to suicide prevention have traditionally involved a patchwork of singular interventions led by multiple agencies, including local champions, behavioral health organizations, and people with lived experience, instead of a coordinated approach rooted in a public health framework. 14,15 Since the release of the National Strategy for Suicide Prevention in 2001 and revision in 2012, recognition of suicide as a public health problem and the need to develop coordinated, community-based approaches to prevent its rise have increased. 4 Although recent publications have highlighted practical steps to implementing a comprehensive, community-based strategy, 5,15,16 most suicide prevention efforts continue to occur at the state level, 2,7 and LHDs have not been widely incorporated into these efforts.
Although little data exist that document the prevalence of LHD involvement in suicide prevention specifically, several studies found that a large percentage of LHDs are not involved in activities related to mental health or substance use—2 primary drivers of suicidal behavior. Data indicate that only about 25% of LHDs in small jurisdictions, 35% of LHDs in medium-size jurisdictions, and 44% of LHDs in large jurisdictions currently implement behavioral health programs. 17 Yet, evidence suggests that LHDs that engage in mental health activities can affect suicidal behavior in a community. A study published in 2019 demonstrated a reduction in suicide-related emergency department visits in counties where the LHD was engaged in mental health activities. 18 To better understand how often LHDs are integrated into state suicide prevention frameworks, we reviewed the statewide suicide prevention plans of the 43 states that have published such a plan online (as of January 2020, all plans had been created or updated in the last 10 years) and found that although 40 (93.0%) states highlight the importance of community-based strategies for preventing suicide, only 6 (14.0%) states discuss LHDs taking leadership roles in these efforts.
Although several notable barriers exist to LHD involvement in suicide prevention and mental health activities more broadly, including limited resources, funding, and lack of knowledge about behavioral health, one important barrier limiting LHD deployment of a public health approach is a lack of adequate county-level data on suicide. 15,19 Despite substantial improvements in access to basic suicide surveillance data that arose with the establishment of the Centers for Disease Control and Prevention’s (CDC’s) National Violent Death Reporting System (NVDRS) in 2002 and, more recently, the creation of the Wide-ranging Online Data for Epidemiologic Research (WONDER) and the Web-based Injury Statistics Query and Reporting System, 14,20,21 most data on suicide monitor trends at the state level. County-level data continue to be poorly integrated into prevention efforts. In our review of 43 state suicide plans, only 21 (48.8%) states provided any county-level data on suicide and only 14 (32.6%) states discussed using data to target regions at elevated risk for suicide. Data organized at the state level are often not specific or granular enough to be actionable by communities. These state-level analyses tend to overlook local areas with higher suicide risk in a state (eg, northern vs southern Florida or western vs eastern Oklahoma) or between states (eg, Appalachian or Ozark regions). 9,22 They also do not identify geographic areas with a low incidence of suicide, which can aid in understanding protective factors and important rural–urban differences. 22,23 Thus, without an understanding of local geospatial variation in suicide rates, including key drivers, local agencies cannot be easily empowered to intervene effectively in communities to reduce the rates of death by suicide.
Review of Studies on County Suicide Rates
One reason county-level data have not been widely incorporated is that direct counts of numbers of deaths by suicide tend to be low per county and, therefore, exhibit wide annual variability. 9,24 A high annual variability in the number of absolute suicide deaths per county makes county rates difficult to interpret and has led to a predominant reliance on state-level surveillance. 2 In effect, because state-level data show rates in a large geographic area, the county-to-county variability in suicide rates is flattened and potentially important county trends may be lost. However, 3 recent studies used spatial epidemiology methods, which improve the reliability of county-level data. Rossen et al 9 used spatiotemporal models to produce stable estimates of county suicide rates from 2005 to 2015. This study concluded that unlike geographic patterns of other causes of premature death, such as drug overdose, the geographic distribution of suicide was consistent during the 10-year study period. 9 Another study used spatial analysis to map excess risk for suicide at the county level during 1999-2016 and found a similar geographic distribution. 8 Finally, Sy et al used county-level data to identify 19 clusters of suicide in the 10 states with the highest suicide rates from 1999 to 2016.10
Identifying Counties at High Risk for Suicide
These recent studies demonstrate that county-level data can be used to produce stable estimates of suicide rates over time, making it possible to identify counties at persistently elevated suicide risk where targeted prevention efforts could have substantial impact. As federal and state leaders begin to think about how to target interventions to reduce rising suicide rates, they may consider several approaches to identifying counties at high risk for suicide. Three approaches could include (1) counties where suicide rates show the greatest increase over time, (2) counties with the highest persistent suicide rates, or (3) counties with the greatest absolute number of deaths by suicide.
To demonstrate these approaches, we used the CDC WONDER Compressed Mortality File Underlying Cause of Death database to analyze county suicide rates. 25 To produce stable county estimates, we aggregated age-adjusted suicide rates from 1999-2003 and 2014-2018, similar to methods used in previous studies. 8,9 Because the CDC WONDER database considers counties with fewer than 20 suicides to be statistically unreliable, 25 we excluded these counties in our analysis (the 1785 excluded counties represented 8.2% of the US population), resulting in an analytic sample of 1362 total US counties or county equivalents (eg, boroughs, census areas) representing 91.8% of the US population and 89.9% (204 588 of 227 501) of all suicides during 2014-2018.
During the period analyzed, the suicide rate increased in 1201 of 1362 (88.2%) counties, demonstrating locally increasing rates in nearly every geographic area of the country. In our attempt to identify 3 sets of counties at high risk for suicide, we then selected (1) the 50 counties with the greatest proportional increase in suicide rates from 1999-2003 to 2014-2018 (absolute change in suicide rate as a percentage of the 1999-2003 rate), (2) the 50 counties with the highest suicide rates in 2014-2018, and (3) the 50 counties with the greatest absolute number of suicides in 2014-2018 (Table).
Three approaches for identifying counties at high risk for suicide in the United States a
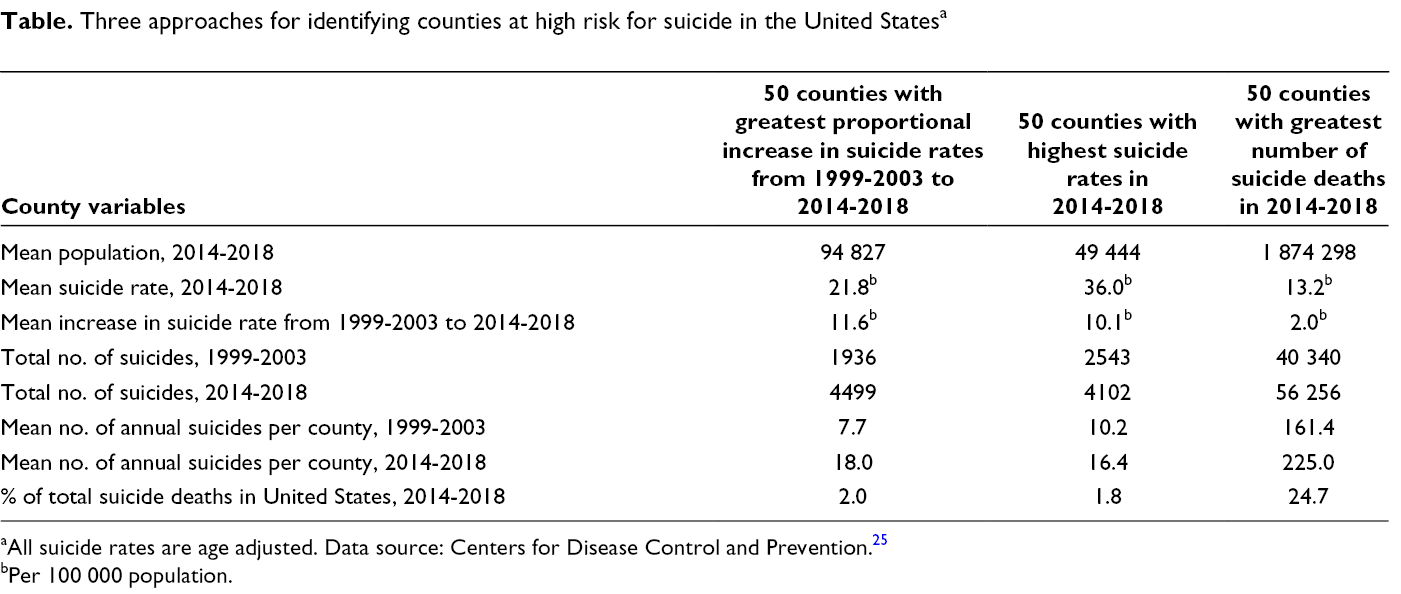
aAll suicide rates are age adjusted. Data source: Centers for Disease Control and Prevention. 25
bPer 100 000 population.
The 50 counties with the highest suicide rates and the 50 counties with the greatest change in suicide rates had high mean rates per 100 000 population of about 36 and 22, respectively. Although the number of suicides in these counties more than doubled during the period analyzed, the 50 counties with the highest suicide rates and the 50 counties with the greatest change in suicide rates still only accounted for 1.8% and 2.0%, respectively, of all suicides in the United States in 2014-2018, largely because of their small populations of about 50 000 and 95 000 people, respectively. In contrast, the 50 counties with the greatest number of deaths by suicide had suicide rates similar to the national average in 2014-2018 (13.6 per 100 000 population) but accounted for nearly 25% of all suicides in the United States, primarily because of their large populations. Policy makers must then choose whether to target prevention efforts in less populated counties, where suicide rates are the highest and increasing the fastest, or in counties with a larger population, where suicide rates are lower but where a greater number of lives could be saved. A small reduction or plateau in suicide rates in these large counties would have a substantial effect on the national rate, whereas a larger reduction in these smaller counties with a high and often long-term prevalence of suicide would not produce as substantial a reduction on the national rate.
Our analysis also demonstrates some of the challenges of tracking county-level data. Although our analysis produced stable estimates of suicide rates in counties where most of the US population lives, it excluded a large number of counties. Although the approach we used to examine changes in suicide rates in groups of counties has limitations, we assert that detailed county analyses, absolute numbers, rates, and trends should be incorporated into state plans. County-level data can be highly informative for planning targeted interventions, as discussed herein.
Public Health Implications and Future Directions
Despite the aforementioned limitations, our brief analysis demonstrates that county-level data can be used to focus attention on areas with a large number of annual suicide deaths and areas with abnormally high rates of suicide that are increasing faster than average national rates. Our study builds on several recent studies 8,9 that began to examine county rates by providing an in-depth discussion of how data might be used by state and local officials to target prevention in areas at high risk for suicide. Just as county-level data have been used to target interventions for other major public health threats, 11,12 community-based approaches to suicide prevention will require successful integration of county-level data.
An initial step toward this goal is to have more states compile county-level data to evaluate local variation in suicide rates across the state. According to our review of state plans, most states do not integrate county-level data and even fewer states are using those data to target areas with high rates of death by suicide. Two states that are tracking county-level data on suicide in innovative ways are Colorado and South Dakota. Colorado developed a data visualization tool that uses local NVDRS data to identify areas with a high prevalence of suicides and populations at high risk for suicide. 26 In addition to using death certificate data, states should consider incorporating data on various types of suicidal behavior, including thoughts, attempts, and nonsuicidal self-injury. Key partners that can provide these data include medical examiners and coroners, hospitals and emergency departments, poison control centers, public and private mental health care systems, crisis response services and crisis lines, correctional systems, and agencies that serve young people. 7 The Substance Abuse and Mental Health Services Administration’s National Survey on Drug Use and Health includes data on suicidal thoughts, plans, and attempts, and these data could be incorporated into planning. 27 South Dakota also created an interactive data dashboard that not only depicts data on the number of county suicides but began to incorporate emergency department data on self-inflicted injury. 28 In addition, the Robert Wood Johnson Foundation County Health Rankings & Roadmaps is a resource that states can use to compile county-level data on important correlates of suicidal behavior, including alcohol use, overdose deaths, firearm fatalities, unemployment, and lack of social connectedness (https://www.countyhealthrankings.org).
Once states have compiled accessible data, several considerations could be taken into account when deciding how to target interventions. Our analysis demonstrated 3 possible approaches to identifying counties at high risk for suicide and the potential limitations of each. An optimal approach would likely include a combination of these 3 approaches, considering smaller counties with the highest rates and greatest change in rates of suicide, in addition to more populated counties with a large number of deaths by suicide. Additional analyses to identify populations at high risk for suicide in counties also play a critical role in deciding which areas to target. In addition to examining quantitative data, states should consider contextual and community factors that may act as facilitators or barriers to suicide prevention. Factors to consider may include the presence of a local public health infrastructure, community readiness and ownership, local champions and partners, and availability of sustainable funding. 5 In assessing these factors, local public health officials may consider conducting an environmental scan of the local suicide prevention infrastructure or a local inventory of suicide prevention activities, which may help identify which regions or subpopulations are currently being served and what gaps exist. The presence of identifiable gaps in services for specific populations at high risk for suicide, including American Indian/Alaska Native people, lesbian/gay/bisexual/transgender populations, justice-involved young people, and military veterans, may help tailor and target interventions. 4
As states focus on areas at high risk for suicide, they should consider leveraging the resources and strengths of LHDs and empower them to lead efforts in their communities. LHDs can serve as community chief health strategists and often have intimate knowledge of a region, including an understanding of local populations and related suicide risk factors. 29,30 They also often have working relationships with key community partners and access to important types of data. Greater collaboration between state and local agencies may help coordinate activities in suicide prevention and avert situations in which agencies are working in isolation. State agencies may support LHDs in many ways, including partnering on applications to federal grants, such as the Substance Abuse and Mental Health Services Administration’s Garrett Lee Smith suicide prevention grants and Zero Suicide grants, and providing training and technical assistance on evidence-based practices, data collection, and program evaluation. State support is particularly important to ensure that suicide prevention does not become another unfunded responsibility of LHDs. With state support, LHDs can take a vital leadership role by serving as organizational hubs to convene community partners in suicide prevention, prioritizing strategic approaches, mobilizing funding, and driving collective action. 29 LHDs can be instrumental in convening traditional community members such as health care providers, social service agencies, school systems, and suicide prevention coalitions. LHDs can also convene nontraditional partners, such as employers, housing authorities, faith-based organizations, news media, and first responders. In convening these partners, LHDs could lead the development of county suicide prevention plans. Although most states have a statewide plan, in our review, only 7 of 43 (16.3%) states mentioned having localities produce suicide prevention plans. By strategically engaging these partners using a data-driven process, LHDs can lead a community-wide approach to suicide prevention.
Conclusion
Innovative community-based approaches are needed to stem the rise of suicide rates in the United States. Until recently, a lack of adequate county-level data on suicide has limited the deployment of targeted prevention strategies. Multiple recent studies, including the brief analysis we describe here, demonstrate that county-level data can be used to identify areas at elevated risk for suicide where interventions can be strategically targeted to save lives. States may consider compiling local data on suicide and suicidal behavior to better understand community risk and protective factors and populations at high risk for suicide. As states look to target interventions in areas at high risk for suicide and, most recently, communities highly affected by COVID-19, they may leverage the resources and strengths of LHDs, which often have working relationships with key partners and intimate knowledge of their community. By using a data-driven and community-based approach, it may be possible to slow suicide rates and shed light on a growing but preventable problem.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.