
Abstract
Objectives
Up-to-date information on the occurrence of drug overdose is critical to guide public health response. The objective of our study was to evaluate a near–real-time fatal drug overdose surveillance system to improve timeliness of drug overdose monitoring.
Methods
We analyzed data on deaths in the King County (Washington) Medical Examiner’s Office (KCMEO) jurisdiction that occurred during March 1, 2017–February 28, 2018, and that had routine toxicology test results. Medical examiners (MEs) classified probable drug overdoses on the basis of information obtained through the death investigation and autopsy. We calculated sensitivity, positive predictive value, specificity, and negative predictive value of MEs’ classification by using the final death certificate as the gold standard.
Results
KCMEO investigated 2480 deaths; 1389 underwent routine toxicology testing, and 361 were toxicologically confirmed drug overdoses from opioid, stimulant, or euphoric drugs. Sensitivity of the probable overdose classification was 83%, positive predictive value was 89%, specificity was 96%, and negative predictive value was 94%. Probable overdoses were classified a median of 1 day after the event, whereas the final death certificate confirming an overdose was received by KCMEO an average of 63 days after the event.
Conclusions
King County MEs’ probable overdose classification provides a near–real-time indicator of fatal drug overdoses, which can guide rapid local public health responses to the drug overdose epidemic.
Keywords
In 2017, approximately 70 000 people died of fatal drug overdoses in the United States, making drug overdose the leading cause of death among people aged 18-49. 1,2 A timely understanding of local drug overdose trends is important for prioritizing resources and targeting services.
Monitoring fatal drug overdoses has traditionally relied on vital statistics, a registry of births and deaths managed by state and territory agencies. Death records in vital statistics are based on death certificates. Only medical examiners (MEs) or coroners are authorized to certify drug overdose deaths; these certifications are aided by laboratory testing of decedent specimens. Limited funding for death investigation systems and toxicology laboratories in the United States is widely acknowledged. 3,4 The National Center for Health Statistics indicates that death certificate records for drug overdose deaths are not available for analysis until an average of 4 months after the death date. 5
To support timely prevention and response activities, state and local health jurisdictions have explored more expedient options than reliance only on toxicology testing and death certificates to assess the epidemiology of drug overdoses, such as using syndromic surveillance platforms, 6 making suspected drug overdose a notifiable condition, 7 or integrating multiple data streams as part of comprehensive drug overdose surveillance systems. 8 With few exceptions, 9,10 local jurisdictions generally do not use ME data directly for monitoring drug overdoses.
King County (Washington) has a population of approximately 2.2 million people and includes Seattle, 38 smaller cities and towns, and large unincorporated areas. The King County Medical Examiner’s Office (KCMEO) investigates all sudden and unexpected, violent, suspicious, or unnatural deaths, including potential fatal drug overdoses. 11 In 2017, KCMEO investigated 383 toxicologically confirmed drug and alcohol deaths, representing 15% of all deaths investigated, for a rate of 17.6 toxicologically confirmed drug and alcohol deaths per 100 000 King County residents. 12
In March 2017, in response to concerns from public health and law enforcement agencies about delays in monitoring drug overdoses, KCMEO initiated a system to document probable overdoses at the time of death investigation without waiting for toxicology results. After 12 months of implementation, we evaluated KCMEO’s near–real-time fatal overdose surveillance system to assess its potential to guide rapid local responses to the drug overdose epidemic.
Methods
King County MEs’ Near–Real-Time Surveillance System
MEs classify the likelihood of fatal overdose for each decedent on the basis of a postmortem examination and death investigation records (eg, death scene description and photos, medical records, and interviews with witnesses and next of kin). Medicolegal investigators document in their narrative reports and photographs any evidence of drug use at the scene of death. 13 Investigators collect drug paraphernalia (eg, syringes, glass pipes, pill containers) and substances present at the scene and identify drugs through toxicology testing. At daily rounds, MEs collectively discuss the circumstances and clinical characteristics of each decedent and systematically assess whether the probable cause of death was drug overdose. For this study, MEs defined a probable overdose as a death in which 2 or more probable overdose indicators were present in the death investigation or clinical examination (Box). Because the purpose of the surveillance system is to identify an increase in unintentional deaths associated with recreational drug use that could signal an increase in lethal drug circulation, MEs did not classify deaths as probable overdose if they suspected the deaths to involve only alcohol, cannabis, or medications unlikely to be used for recreational purposes (eg, acetaminophen, digoxin) or if drug toxicity was not the primary cause of death (eg, traffic collision, injury that occurred under the influence of drugs).
Probable overdose indicators used by medical examiners to classify deaths as probable overdoses for the near–real-time surveillance of fatal drug overdoses, King County, Washington, 2017-2018
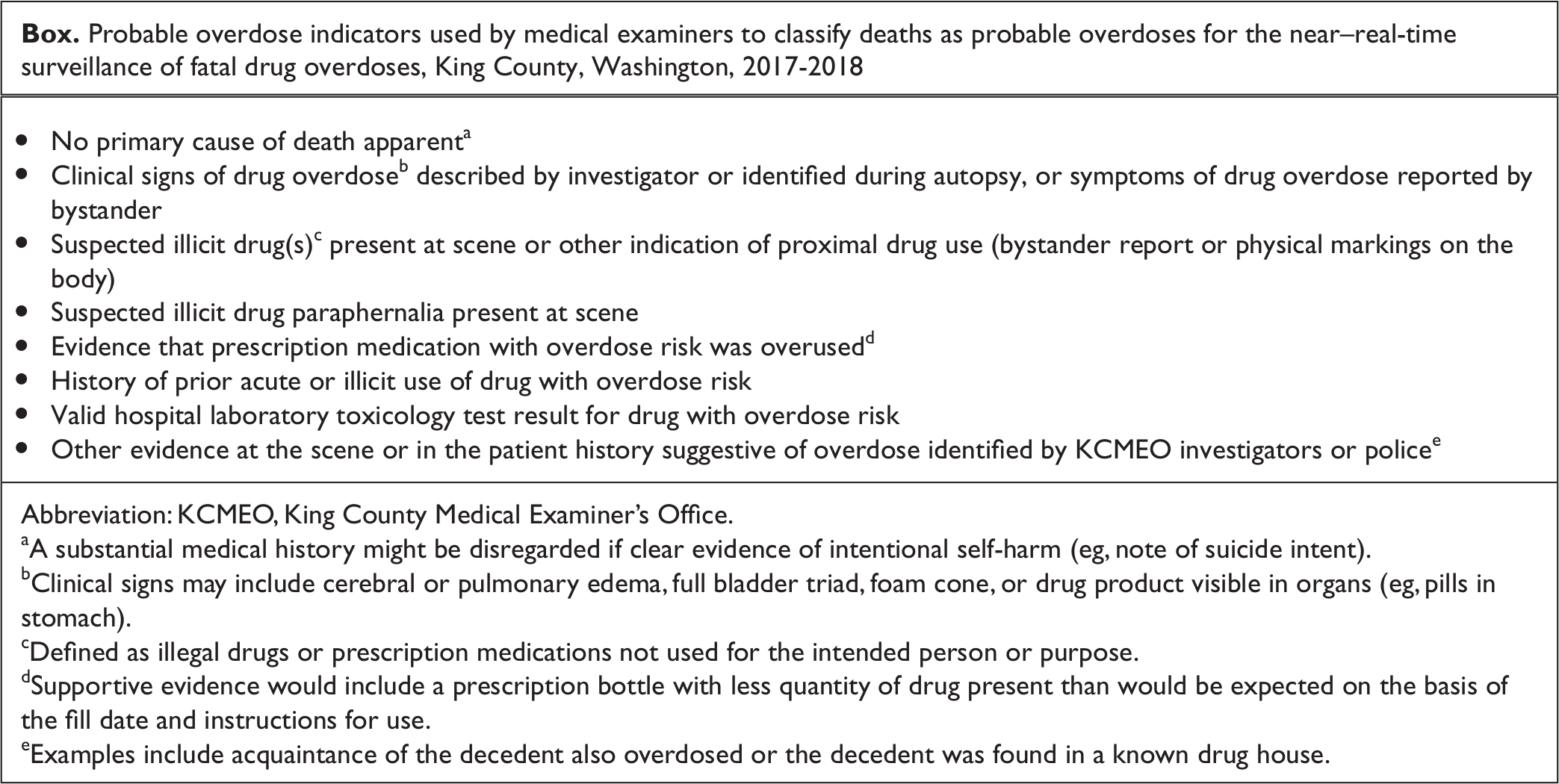
aA substantial medical history might be disregarded if clear evidence of intentional self-harm (eg, note of suicide intent).
bClinical signs may include cerebral or pulmonary edema, full bladder triad, foam cone, or drug product visible in organs (eg, pills in stomach).
cDefined as illegal drugs or prescription medications not used for the intended person or purpose.
dSupportive evidence would include a prescription bottle with less quantity of drug present than would be expected on the basis of the fill date and instructions for use.
eExamples include acquaintance of the decedent also overdosed or the decedent was found in a known drug house.
For our evaluation, scene-of-death investigation, postmortem examination, medical records, and information supplied by families of the decedent were the sources of information on demographic characteristics, medical history, and social history of the decedent. An epidemiologist external to KCMEO abstracted all data from the decedent’s medical record. We dichotomized housing status as having a residence or experiencing homelessness, with the latter designation used if the decedent had no record of address and scene-of-death investigation supported this designation. Postmortem examination typically includes a full autopsy to determine cause and manner of death. Deaths in KCMEO’s jurisdiction that do not require autopsy include the following: decedents aged ≥60 years without evidence of physical injury or illicit or excessive drug use; decedents who died in a hospital with an established cause of death other than overdose and whose death had no legal concerns; and decedents with self-inflicted firearm injury with an exit wound and no projectile(s) to recover from the body. MEs collect blood and vitreous fluid from all decedents except in situations of advanced postmortem decomposition.
Toxicology Testing
The Washington State Patrol (WSP) Toxicology Laboratory tests postmortem blood and vitreous specimens for all deaths in which no obvious nonoverdose cause of death was indicated (eg, gunshot wound), deaths in which ongoing criminal investigations involved the decedent, traffic fatalities, and most deaths in which an autopsy was performed.
WSP toxicology analyses include head-space gas chromatography for ethanol and other volatiles, screening for general classes of drugs by enzyme-multiplied immunoassay technique or basic (alkaline) drugs by gas chromatography–mass spectrometry, and confirmation and quantitation of specific drugs by gas chromatography–mass spectrometry and liquid chromatography–mass spectrometry. WSP methods generally cannot detect less common synthetic drugs (eg, synthetic cannabinoids, synthetic cathinones [ie, bath salts], novel fentanyl analogs); if MEs suspect these drugs, they submit the specimen to a private laboratory (NMS Labs, Inc). For deaths in which morphine is detected in the blood but 6-acetylmorphine was not, WSP’s laboratory performs additional testing on vitreous fluid to detect presence of 6-acetylmorphine, which indicates heroin as the blood morphine source. Other evidence of blood morphine being caused by heroin, rather than pharmaceutical morphine, comes from the scene-of-death investigation (eg, presence of drug substance, paraphernalia indicating heroin use) or circumstances of death (eg, history of heroin use).
We categorized other opioids (nonheroin) and other prescription drugs by the drugs identified by toxicology testing that are found in legal prescriptions regardless of whether they were legally procured or illicitly manufactured, the latter of which rarely occurs.
Death Certification
MEs complete and enter death certificates 14 into the Washington Electronic Death Registration System, usually within 24 hours of postmortem examination. For suspected overdose deaths pending toxicology testing, MEs complete the final death certificate by affidavit only after the report of drug testing was returned from WSP’s laboratory. MEs amend the death certificate by affidavit for deaths not suspected to be caused by overdose if routine toxicology testing subsequently indicates a drug overdose caused the death. We defined a confirmed overdose as a certified death 14 with an immediate or underlying cause of death of acute drug intoxication, as informed by toxicology testing.
Evaluation Criteria
The cause-of-death statement (as documented in Section 32 of the death certificate 14 ) among decedents who underwent routine toxicology testing served as the gold standard for the evaluation of sensitivity, specificity, positive predictive value (PPV), and negative predictive value of the MEs’ probable overdose classification during March 1, 2017–February 28, 2018. We calculated these metrics by standard methods. 15 We assessed differences in demographic characteristics by using Pearson χ2 tests for categorical variables and 1-way analysis of variance for continuous variables. We conducted all analyses using SAS version 9.4 (SAS Institute, Inc). The Centers for Disease Control and Prevention reviewed this project and determined it to be nonresearch, public health response.
Results
Confirmed Drug Overdoses
During the 12-month evaluation period, KCMEO investigated 2480 deaths. Of these, 1429 (58%) had a full autopsy and 1389 (56%) underwent toxicology testing. Of deaths with toxicology testing, MEs confirmed and certified as overdose deaths 361 (26%) drug overdoses with opioids, stimulants, or other types of euphoric drugs (eg, benzodiazepines, antidepressants) (Table 1). Of the 361 overdose deaths, 263 (73%) involved an opioid, including heroin (44%; n = 159), other opioids such as methadone and oxycodone (26%; n = 103), and fentanyl and its analogs (11%; n = 39) (Figure 1). One hundred ninety-one (53%) overdose deaths involved stimulants, including methamphetamine (38%; n = 136) and cocaine (21%; n = 74), and 92 (25%; n = 92) deaths involved benzodiazepines. Of all overdose deaths, 232 (64%) were attributed to a combination of ≥2 drug substances; the median number of drugs identified in 1 decedent by toxicology testing was 2 (range, 1-6). The most common probable overdose indicator was a history of drug use (n = 200; 55%), drug paraphernalia at the scene of death (n = 169; 47%), and drug product at scene or other evidence of recent drug use (n = 151; 42%) (Table 2).
Comparison of medical examiners’ probable drug overdose classification with gold standard death certification, King County, Washington, March 1, 2017–February 28, 2018 a
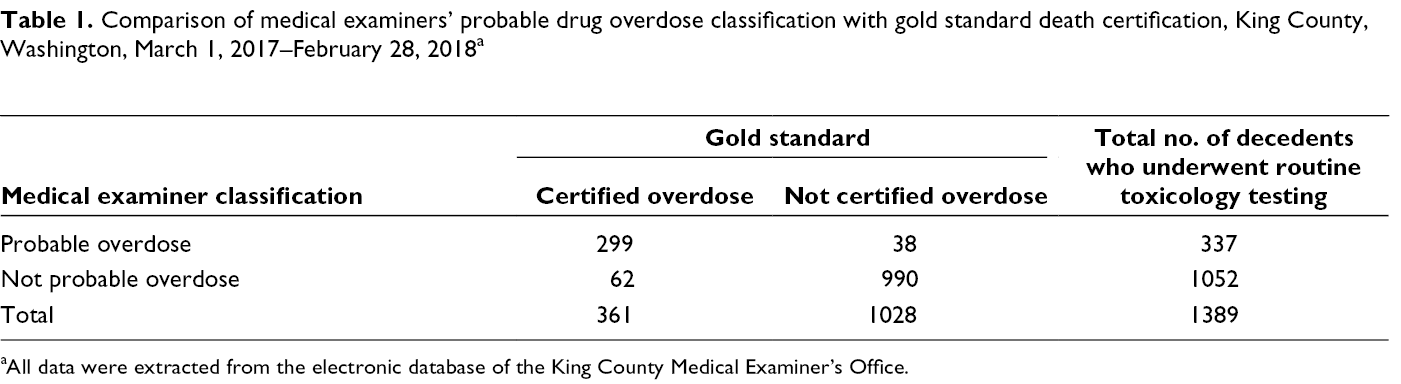
aAll data were extracted from the electronic database of the King County Medical Examiner’s Office.
Selected probable overdose indicators from death investigation for toxicologically confirmed drug overdoses (N = 361) and medical examiner–classified probable overdoses, King County, Washington, March 1, 2017–February 28, 2018 a
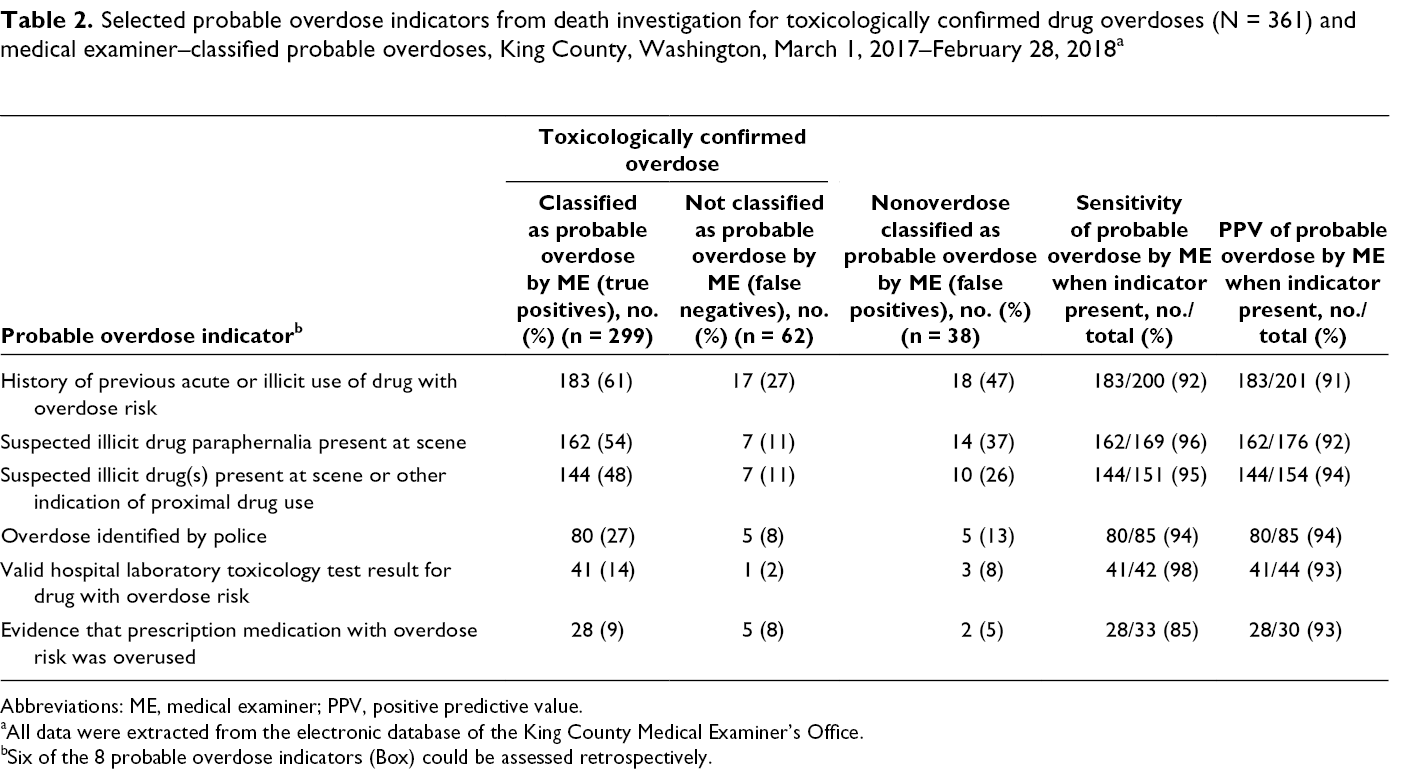
Abbreviations: ME, medical examiner; PPV, positive predictive value.
aAll data were extracted from the electronic database of the King County Medical Examiner’s Office.
bSix of the 8 probable overdose indicators (Box) could be assessed retrospectively.
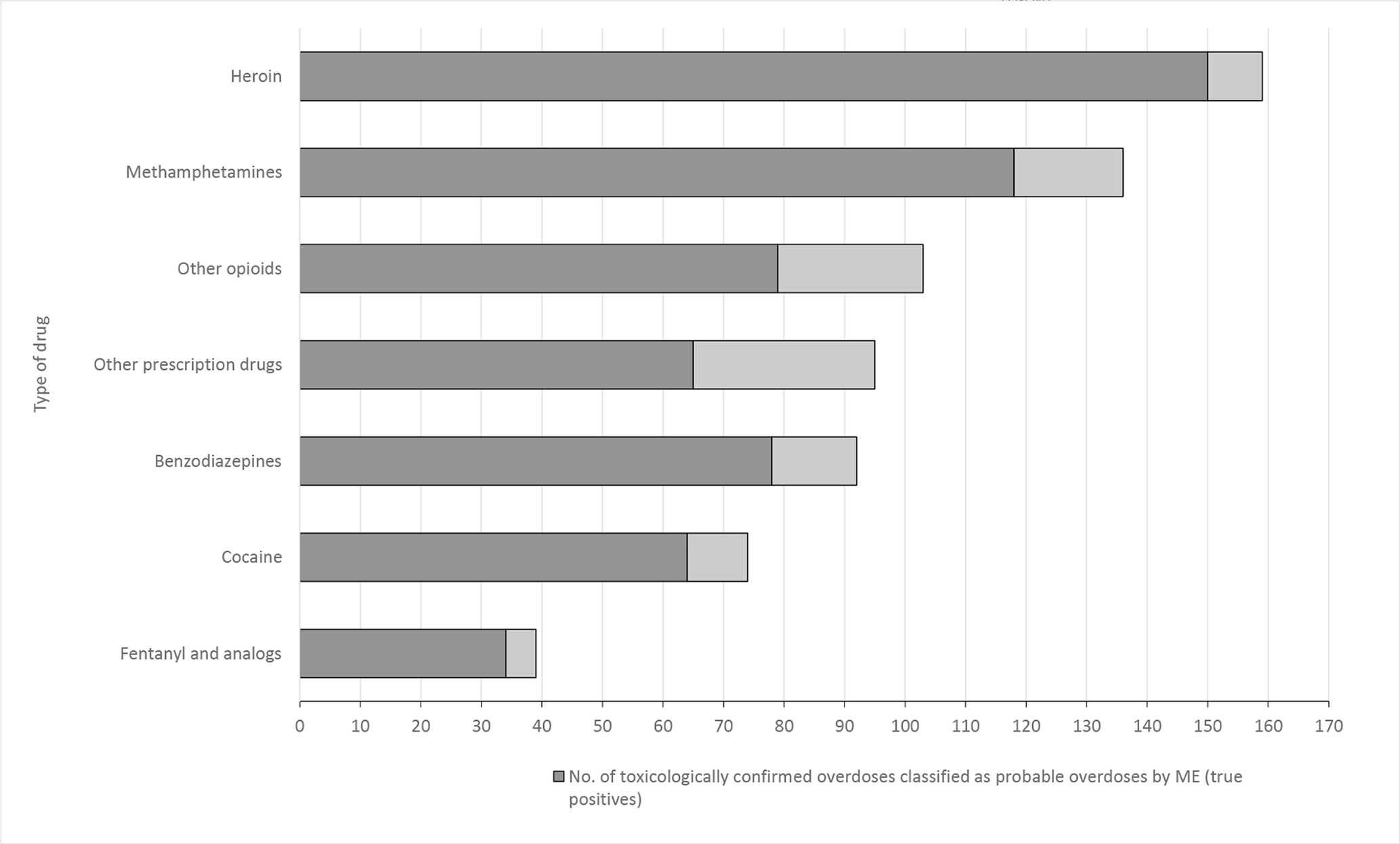
Drugs identified through toxicology testing among confirmed drug overdoses by whether the medical examiners correctly classified the death as a probable overdose, King County, Washington, March 1, 2017–February 28, 2018. A death could involve multiple drug classes. Other opioids and other prescription drugs were defined by the drug(s) identified by toxicology testing that are found in legal prescriptions regardless of whether they were legally procured or illicitly manufactured. All data were extracted from the electronic database of the King County Medical Examiner’s Office. Abbreviation: ME, medical examiner.
Most confirmed drug overdoses occurred among males (70%) and decedents who were White (81%), followed by Black (10%) (Table 3). Overall, 18% of confirmed drug overdoses were among people experiencing homelessness. Most (67%) deaths occurred at a place of residence.
Demographic and scene-of-death characteristics of confirmed and probable drug overdoses, King County, Washington, March 1, 2017–February 28, 2018 a
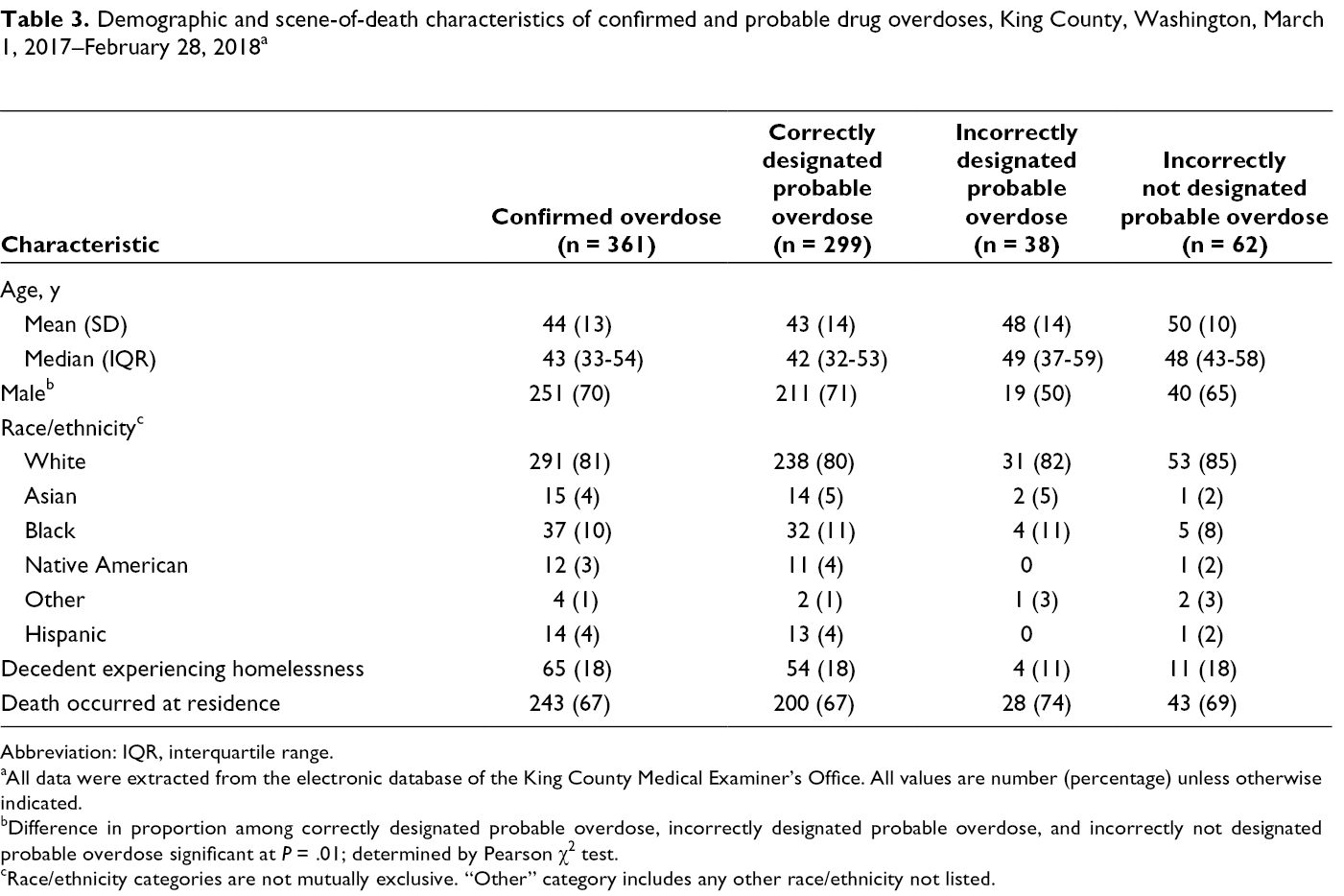
Abbreviation: IQR, interquartile range.
aAll data were extracted from the electronic database of the King County Medical Examiner’s Office. All values are number (percentage) unless otherwise indicated.
bDifference in proportion among correctly designated probable overdose, incorrectly designated probable overdose, and incorrectly not designated probable overdose significant at P = .01; determined by Pearson χ2 test.
cRace/ethnicity categories are not mutually exclusive. “Other” category includes any other race/ethnicity not listed.
Accuracy of KCMEO Near–Real-Time Surveillance System
During the 12-month evaluation period, MEs classified 337 deaths as probable overdoses (Table 1). MEs correctly classified 299 probable overdoses of the 361 toxicologically confirmed drug overdoses (true positives), for a sensitivity of 83% (95% CI, 79%-87%) and a PPV of 89% (95% CI, 85%-92%). Weekly counts ranged from 2 to 14 for confirmed overdoses and 1 to 17 for probable overdoses (Figure 2). Trends in probable drug overdoses closely matched trends in confirmed drug overdoses.
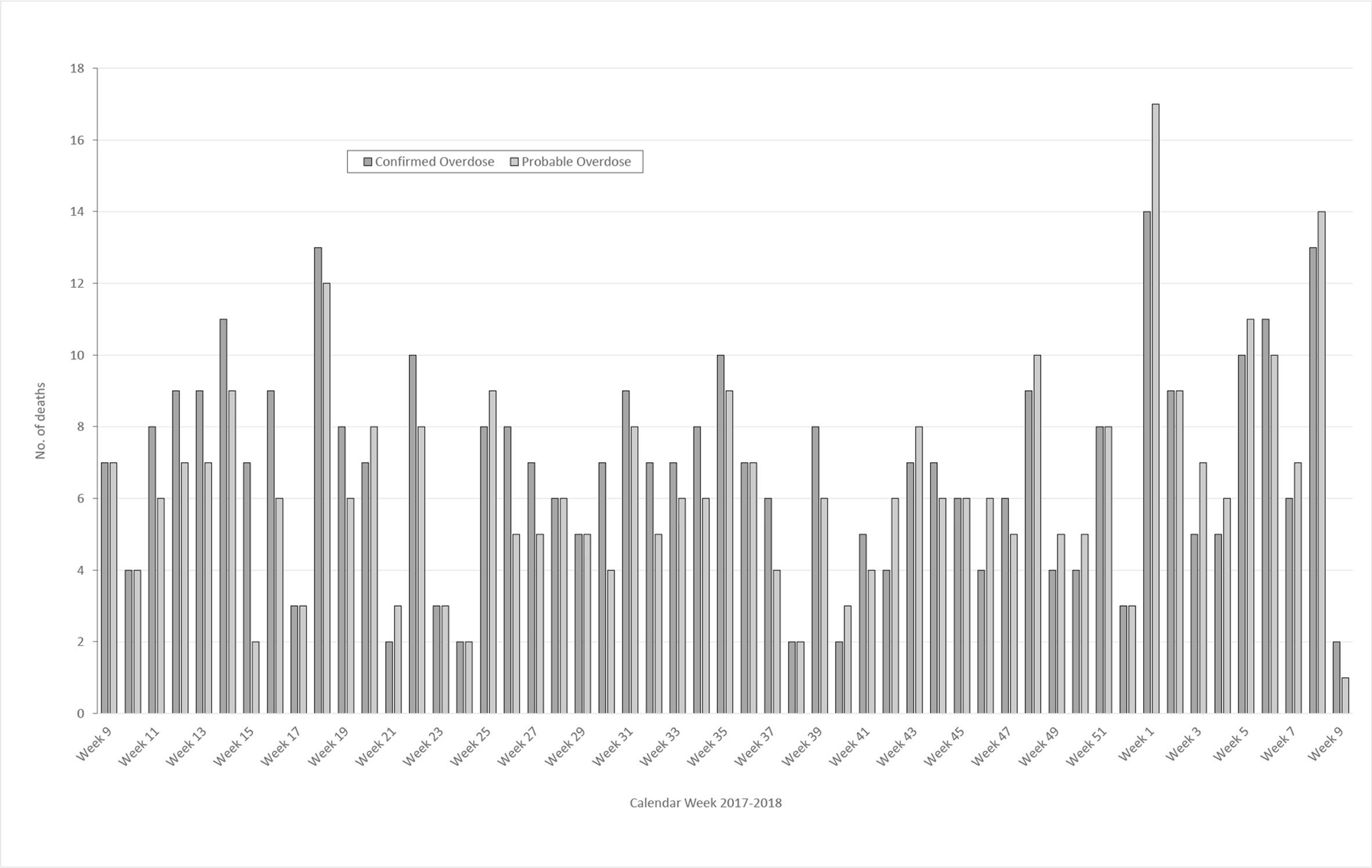
Weekly trends in confirmed and probable drug overdose deaths, King County, Washington, March 1, 2017–February 28, 2018. All data were extracted from the electronic database of the King County Medical Examiner’s Office.
MEs classified 38 deaths as probable overdoses that were not confirmed by toxicology testing (false positives). MEs did not classify as probable overdose 62 deaths that toxicology testing confirmed as drug overdoses (false negatives). MEs’ probable overdose classification performed best when physical evidence of drug use was at the scene of death. When drug paraphernalia was present, sensitivity was 96% and PPV was 92%; when drug product or evidence of recent use was present, sensitivity was 95% and PPV was 94% (Table 2).
Demographic characteristics of race, ethnicity, housing status, and location of death were similar across true positives, false positives, and false negatives (Table 3). The percentage of male decedents was higher among true positives (71%; 211 of 299) than among false positives (50%; 19 of 38) (χ2 = 6.0, P = .01). The mean (SD) age of decedents was higher among false negatives (50 [10] years) than among true positives (43 [14] years) (F = 4.76, P = .03).
Of the 299 true positives, 192 (64%) were attributed to a combination of ≥2 drugs; 183 (61%) decedents had a history of illicit drug use; 162 (54%) had drug paraphernalia at the scene of death; and 144 (48%) had evidence of drug products or recent drug use at the scene (Table 2). Of the 299 true positives, 163 (55%) deaths involved a stimulant, 150 (50%) involved heroin, 79 (26%) involved other opiates, 78 (26%) involved benzodiazepines, and 34 (11%) involved fentanyl. Other prescription drugs, such as antidepressants and anticonvulsants, were involved in 65 (22%) overdose deaths.
Among 38 false positives, chronic drug abuse was listed as a contributory cause for 16 (42%) deaths. The most common primary cause of death (n = 17; 45% of decedents) among false positives was cardiovascular disease. Infectious etiologies, such as Streptococcal pneumoniae and Staphylococcus aureus, were noted in 6 deaths and chronic ethanolism or alcohol withdrawal syndrome in 5 deaths. Other causes were endocrine disease (eg, diabetes), liver disease, gastrointestinal disease, respiratory disease, and deaths with no apparent anatomic or toxicological cause. Of the 38 false positives, 18 (47%) occurred among decedents with a history of illicit drug use, and 14 (37%) had drug paraphernalia at the scene of death.
Among 62 false negatives, 17 (27%) decedents had a history of illicit drug use, 7 (11%) had drug paraphernalia at the scene of death, and 7 (11%) had drug products or evidence of recent drug use at the scene. Forty (65%) involved ≥1 drug. Twenty-eight (45%) false negatives involved a stimulant, 24 (39%) involved other opiates, 14 (23%) involved benzodiazepines, 9 (15%) involved heroin, and 5 (8%) involved fentanyl. Other prescription drugs were involved in 29 (47%) false negatives.
Timeliness of Information on Fatal Drug Overdoses
Overall, dates of autopsy (100%), toxicology results received (95%), and certification of confirmed overdoses (94%) were available among all probable overdose deaths. The median time from death to MEs’ probable overdose classification was 1 day (interquartile range [IQR], 1-2 days; range, 0-51 days); toxicology results received by KCMEO was 59 days (IQR, 46-75 days; range, 21-138 days); and certification was 63 days (IQR, 51-80 days; range, 17-149 days).
Lessons Learned
Use of MEs’ probable overdose classification for near–real-time surveillance of fatal drug overdoses can be a reliable and timely early warning system for drug overdoses. Approximately 90% of the deaths classified as a probable overdose were ultimately confirmed as drug overdose deaths, and 83% of confirmed fatal drug overdoses were correctly identified as probable overdoses. The closely matched weekly counts of confirmed overdoses and probable overdoses indicate that MEs’ near–real-time surveillance is a reliable early indicator of overdose trends. The system performed especially well for drug overdoses in which drug paraphernalia or drug products were at the scene.
On average, our system allowed an assessment of fatal overdose trends approximately 2 months before drug overdoses were confirmed by toxicology and certified in vital records. Two months is likely a conservative estimate, because the WSP laboratory received temporary supplemental funding during the evaluation period to improve timeliness of toxicology testing.
Baseline demographic characteristics of decedents whose deaths were identified as true positives, false positives, or false negatives were similar, indicating that the probable overdose classification was not affected by systematic bias in data on race, ethnicity, housing status, or other measured factors. The probable overdose indicators also helped prevent contextual bias in probable overdose assessments. Decedents whose deaths were identified as true positives or false positives were significantly different by sex. Among decedents for whom MEs incorrectly classified the death as probable overdose, the percentage of males and females was 50-50, but for confirmed overdoses, approximately 70% were male. Decedents were significantly older among false negatives than among true positives; this difference might be explained by the higher prevalence of comorbidities among older people.
MEs classified 38 deaths as probable overdoses that were not confirmed by toxicology testing (ie, false positives). For example, in the presence of drug paraphernalia, MEs classify a death as probable overdose by acute drug intoxication, but subsequent autopsy may reveal the death was caused by a disease related to chronic, long-term substance use disorder. Uncontrolled diabetes may also explain false positives, as ketoacidosis might give rise to symptoms resembling drug intoxication and insulin syringes could be interpreted as drug paraphernalia. Other possible explanations for false positives include an extended period of opioid-induced respiratory depression before death, during which time the drug(s) in a decedent’s blood can metabolize below the limits of detection or reporting.
Toxicologically confirmed overdose deaths that were not classified by MEs as a probable overdose (false negatives) occurred in 62 cases (17% of confirmed overdose deaths). Only 11% of overdose deaths identified as false negatives were associated with drug paraphernalia at the scene of death, compared with 54% of overdose deaths correctly classified as probable overdose. Various drugs were involved in the overdose deaths determined to be false negative. Prescription drugs, including other opioids, were more frequently represented than heroin. For prescription drugs, signs of use, drug(s) ingested, or paraphernalia might be missing at the time of scene investigation.
The surveillance system described in this study is analogous to syndromic surveillance commonly used for other conditions. Rapid detection of fatal drug overdoses is desirable to identify signals of emerging drug threats, such as synthetic opioids with high fatal overdose potential. Local health jurisdictions might use these signals in several ways to prevent additional morbidity and mortality from drug overdoses. These approaches include increasing the availability of naloxone, geographically targeting distribution of naloxone, providing academic details for health care providers, developing public communications for health care providers and vulnerable populations, and notifying law enforcement partners working to interrupt the drug supply chain. The surveillance system also allows for prioritized toxicology testing of deaths that MEs classify as probable overdose. As a result of our evaluation, Public Health–Seattle & King County developed a public-facing web-based dashboard that includes monthly counts of both confirmed drug overdoses and probable overdoses pending confirmation. 16
MEs’ probable overdose classification is not intended to replace toxicology testing, which remains the gold standard for detecting the array of drugs causing death. Therefore, it is important to continue building capacity of death investigation systems and local toxicology laboratories.
This study had several limitations. First, drug overdose deaths could have been missed. Of all deaths investigated by KCMEO, toxicology testing was performed on the specimens of 56% of decedents. However, the death records of decedents without toxicology testing clearly indicated alternative causes of death, making it unlikely that drug overdoses would be missed. All blood specimens that underwent toxicology testing were screened by enzyme-multiplied immunoassay technique, which is sensitive for detecting general classes of drugs, and 93% of specimens were screened for basic drugs, including fentanyl, by gas chromatography–mass spectrometry. The limit of detection of the basic drug screen for fentanyl is 5 ng/mL; fentanyl-only overdoses may have been missed if the quantity was below the limit of detection. One-third of all decedents classified as probable overdoses underwent additional testing for fentanyl and novel synthetic opioids; for the rest, these synthetic drugs might not have been detected at WSP. Second, MEs did not document the specific probable overdose criteria fulfilled by each decedent at the time of assessment, and so we were unable to evaluate probable overdose criteria that could not be captured retrospectively; that is, no apparent primary cause of death or other evidence at the scene or in the patient history suggested overdose to KCMEO investigators or police not captured by the other criteria. These criteria may have performed less well than those evaluated. Third, we were unable to evaluate criteria by drug type, because most overdoses involve a combination of drugs, or by route of administration, because this detail is often not confirmed by scene investigation.
KCMEO’s near–real-time probable overdose surveillance system requires few additional resources and can be implemented with simple training. Until more resources and better tools are available to facilitate rapid toxicology testing to quickly confirm drug overdose deaths, solutions such as the one described by our study provide a valuable option to guide timely public health responses.
Footnotes
Acknowledgments
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.