
Abstract
Objectives
Indian Health Service (IHS) screening rates for Chlamydia trachomatis are lower than national rates of chlamydia screening in the Southwest. We describe and evaluate the effect of a public health intervention consisting of electronic health record (EHR) reminders to alert health care providers to screen for chlamydia at an IHS facility. We also conducted an awareness presentation among health care providers on chlamydia screening.
Methods
We conducted our intervention from November 1, 2013, through October 31, 2015, at an IHS facility in the Southwest. We implemented algorithms that queried database values to assess chlamydia screening performance in 6 clinical departments. We presented data on the screening performance of clinical departments and health care providers (de-identified) in the awareness presentations. We re-queried database values 1 and 2 years after implementation of the EHR reminder intervention to evaluate before-and-after screening rates, comparing data among all patients and among female patients only.
Results
We found small, sustained relative increases in chlamydia screening rates during the 2012-2015 evaluation period: 20.8% pre-intervention to 24.9% and 24.2% one and two years postintervention, respectively, across all patients; 32.3% preintervention to 36.6% and 35.6% one and two years postintervention, respectively, among female patients. Increases in clinical department–specific screening rates varied and were most prominent in internal medicine (35.8% preintervention to peak 65.8% postintervention). The 1 clinic (obstetrics–gynecology) that did not receive an awareness presentation showed a consistent downward trend in screening rates, although absolute rates were consistently higher in that clinic than in other clinics.
Conclusions
Awareness presentations that offer feedback to health care providers on screening performance, heighten provider awareness of the importance of chlamydia screening, and promote development of novel provider-initiated screening protocols may help to increase screening rates when combined with EHR reminders.
The most commonly reported sexually transmitted infectious disease in the United States is Chlamydia trachomatis. In 2018, more than 1.75 million cases of chlamydia were reported in the United States; the latest available analysis suggests that chlamydia treatment costs are at least approximately $516.7 million. 1,2 Chlamydia is associated with HIV coinfection, leading to further treatment cost. 1,3 -5 Young adults and adolescents have a disproportionately high number of chlamydia infections: in 2018, the overall US prevalence of chlamydia was 539.9 cases per 100 000 adults aged 18-24, with the greatest number of cases affecting females aged <20. 1,3
Sexually transmitted diseases (STDs) are particularly prevalent in racial/ethnic minority populations, with American Indian/Alaska Native (AI/AN) people ranking second highest among all racial/ethnic groups in the prevalence of STDs. 1 In 2018, the chlamydia incidence rate of 1146.3 cases per 100 000 AI/AN people was 4.1 times the national rate among non-Hispanic White people. 1 In addition, AI/AN populations face socioeconomic barriers to accessing health care: 28% lived below the federal poverty level in 2014. 6 AI/AN people incur large transportation costs in attempting to access health care; they also face social stigma related to seeking health care for STDs. 7,8
The US Preventive Services Task Force (USPSTF) recommends that sexually active women aged <25, pregnant women of any age, and nonpregnant women of any age at high risk for STDs be screened annually for chlamydia. 2 Primary and secondary prevention strategies for chlamydia have historically relied on such age-based annual screening, with demonstrated reduction in morbidity. 2,3 The national screening rate is at only 40%-50%, however, and was 38% among female AI/AN populations in a study published in 2011. 1,5
The Indian Health Service (IHS) is a federal health agency in the US Department of Health and Human Services charged with addressing the health care and public health needs of federally recognized American Indian tribes in the United States. Approximately 2.2 million people are enrolled in 573 tribes across 36 states. In 1 IHS area in the Southwest, regional chlamydia incidence rates consistently exceeded both national and IHS average incidence rates during 2003-2015 and, during that time, incidence increased. 9 In 2015, case rates per 100 000 people were 926.8 in the Southwest, 693.6 in the IHS, and 478.8 in the nation. 9
In 2013, an IHS facility in New Mexico implemented an electronic health record (EHR) reminder system to improve chlamydia screening in its catchment population. Other studies have documented improvement in screening rates when EHR reminder systems were complemented by additional support for clinical staff members. 10,11 Measuring health care provider–based outcomes and sharing results with those providers, together with a clinical reminder follow-up, are key steps in the success of EHR-based reminders. 12 Building on the EHR reminder system initiated in 2013, we conducted a chlamydia awareness presentation in July 2014 to support clinical staff members in chlamydia screening. We assessed the effect of the EHR reminders and the awareness presentation during 2 years.
Methods
Performance Data on Chlamydia Screening
The IHS study site at which our initiative was implemented provides multidisciplinary inpatient and outpatient care to a large expanse of IHS-covered territory in the Southwest. Active services at the facility include internal medicine, pediatrics, urgent care, emergency room, obstetrics–gynecology, general surgery, anesthesia, radiology, pathology, psychiatry, ophthalmology, otolaryngology, and urology. The facility has an average yearly workload of approximately 250 000 outpatient encounters and 5800 inpatient admissions.
On November 1, 2013, the IHS study site implemented an EHR-based reminder system for prompting standard chlamydia screening. The EHR reminder consisted of an alarm-clock icon that is standard for other metrics of preventive care in the lower–left-hand corner of the Chart Overview screen. Reminders did not disrupt EHR workflow and could be bypassed by the physician provider.
We reviewed the EHR database to collect data on the proportion of patients screened for chlamydia before implementation of the EHR reminder system and during the first year and second year after implementation of the EHR reminders. We developed algorithms to assess and evaluate screening performance in 6 clinical departments and by 68 health care providers. We obtained health care provider names from the IHS electronic mailing system and clinical department names from the facility database. We did not review or store individualized patient data, and we did not collect any data through direct intervention or interaction with patients. Thus, institutional review board approval was not required, in full accordance with National Institutes of Health human subjects research guidelines.
Chlamydia Awareness Presentation Conducted Among Health Care Providers
Expecting that increases in chlamydia screening would be temporary if the presentation addressed only awareness among health care providers, we designed our awareness presentation with 2 additional purposes in mind: (1) to solicit input from health care providers on how best to incorporate chlamydia screening into the clinic, which would increase health care provider buy-in, and (2) to spark discussion of novel department-initiated chlamydia screening protocols. We conducted an awareness presentation that comprised a brief lecture-format presentation on the EHR reminder system and review of chlamydia epidemiology in the AI/AN population. We prepared data on the chlamydia screening rates of 6 core clinical departments and presented this information to 5 clinical departments during a 2-week period in July 2014: emergency department, urgent care clinic, internal medicine, family medicine, and pediatrics. We prepared a presentation for the obstetrics–gynecology department, but we did not present it because of unanticipated logistical reasons.
We presented anonymized data on health care provider performance in histogram format. We compared all data with data in national guidelines. 1 Presentations focused on the following: (1) potential gaps in health care provider knowledge on chlamydia screening, (2) potential opportunities to include chlamydia screening in clinics, and (3) exploration of independent, department-initiated chlamydia screening protocols. We studied 6 clinical departments for pre– and post–EHR reminder implementation evaluation.
Two clinical departments, internal medicine and pediatrics, implemented new screening protocols before year 2 post–EHR reminder implementation as a result of discussions during the awareness presentation. Pediatrics implemented population-wide screening for all patients aged >16 years in the pediatric population. Internal medicine implemented standing orders for STD testing among all patients admitted to general medical wards and gave nursing support staff immediate access to testing supplies, reducing the task load among physician providers and facilitating chlamydia screening.
Evaluation of Intervention
We collected data on chlamydia screening from the facility’s EHR system. We queried for a validated urine nucleic acid amplification test used since 2011 to diagnose chlamydia infection. The data set included values from all patients who (1) were not deceased, (2) visited a specified health care provider in a specified clinical department during a specified period, (3) were within the eligible disease screening age range at the time of visit, (4) were screened, and (5) were eligible but not screened.
We defined date ranges as follows: pre–EHR reminder implementation (November 1, 2012–October 31, 2013); year 1 post–EHR reminder implementation (November 1, 2013–October 31, 2014); and year 2 post–EHR reminder implementation (November 1, 2014–October 31, 2015). To confirm the absence of trends in screening rates before November 1, 2012, we also tabulated data from November 1, 2011, through October 31, 2012 (2011-2012).
We collected data on patients aged 13-30. Anecdotal evidence from local health care providers suggests that sexual activity in the regional population begins approximately at age 13. Given the natural history of chlamydia, we assumed that symptomatic patients were a negligible fraction of patients tested. 13 We also assumed that the rates of decrease in STD incidence and in sexual activity were negligible in our study population. Outside laboratory testing was not a factor in the database values analyzed: nearly all nucleic acid amplification tests for chlamydia were performed onsite.
Statistical Analysis
We used Excel 2016 (Microsoft Corporation) to tabulate and display data. First, we counted the number of chlamydia screening–eligible patient visits and, of those visits, the number of patients who were screened, and we calculated proportions for each of the 6 clinical departments. We counted visits and calculated proportions for both male and female patients (overall) and for female patients only. We used χ2 goodness-of-fit tests to compare differences in screening rates, with P < .05 considered significant. Because we did not review or store individualized patient data, we externally validated our data-gathering algorithms with independent database experts at the IHS study site.
We used an interrupted time-series analysis for trendline evaluation of our discrete, single-event intervention. At the time of this analysis, in 2016, we did not have data beyond the year 2 post–EHR reminder implementation, which precludes meaningful trendline analysis. Because of our study design and our inability to analyze individualized patient data, and because our data were at the population level, we could not calculate confidence intervals or interquartile ranges for our proportions.
Results
Overall, 8775 chlamydia screening–eligible patients were seen during 2011-2012; 8638 were seen in the pre–EHR reminder period; 8485 were seen during year 1 post–EHR reminder implementation; and 8407 were seen during year 2 post–EHR reminder implementation. Of these chlamydia screening–eligible patients, chlamydia screening occurred at increased rates in years 1 and 2 post–EHR reminder implementation (Table 1). During 2011-2015, of 34 305 screening-eligible patients, 18 000 (52.8%) were seen at least once in the emergency department and 17 914 (52.2%) were seen at least once in the urgent care clinic. The emergency department and urgent care clinic accounted for 46.3% (4135 of 8932) and 59.3% (5293 of 8932) of all chlamydia screening tests ordered, respectively. We found no significant trends in the number of chlamydia screening–eligible patients encountered at the IHS study site over time.
Number of chlamydia screenings performed, by clinical department, as a percentage of chlamydia screening–eligible patients before and after implementation of an electronic health record (EHR) reminder intervention at an Indian Health Service facility in the US Southwest, 2011-2015 a
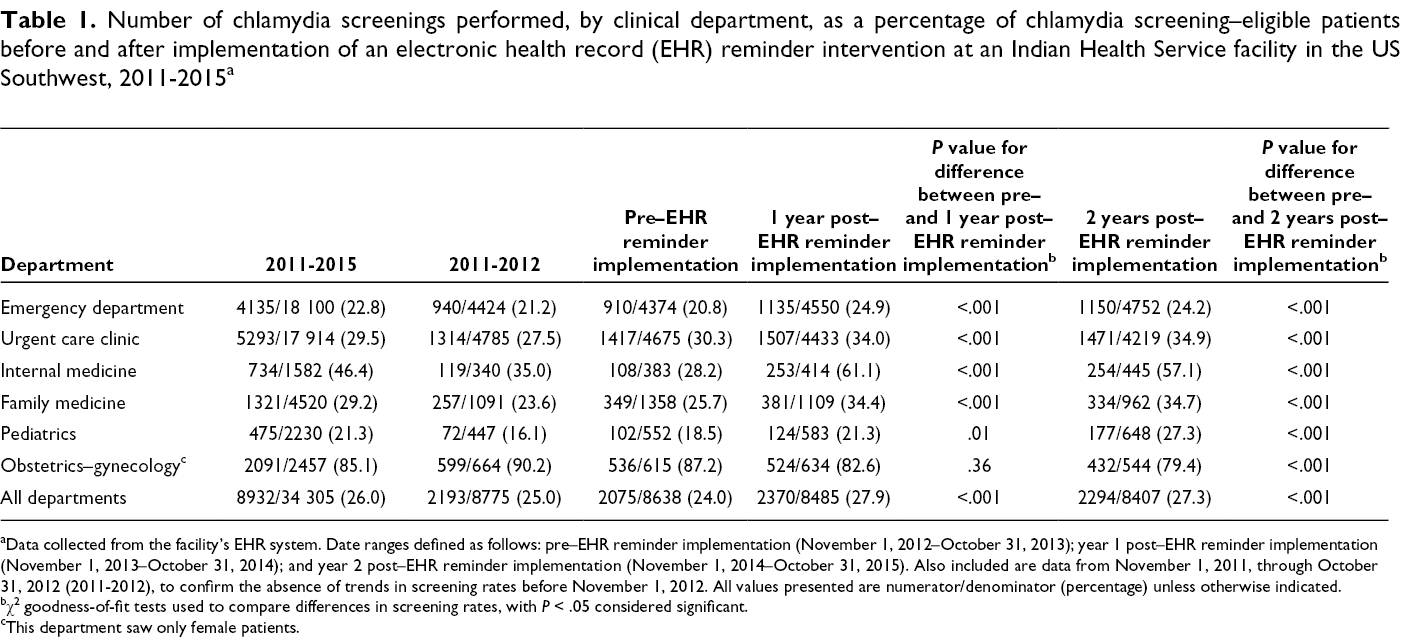
aData collected from the facility’s EHR system. Date ranges defined as follows: pre–EHR reminder implementation (November 1, 2012–October 31, 2013); year 1 post–EHR reminder implementation (November 1, 2013–October 31, 2014); and year 2 post–EHR reminder implementation (November 1, 2014–October 31, 2015). Also included are data from November 1, 2011, through October 31, 2012 (2011-2012), to confirm the absence of trends in screening rates before November 1, 2012. All values presented are numerator/denominator (percentage) unless otherwise indicated.
bχ2 goodness-of-fit tests used to compare differences in screening rates, with P < .05 considered significant.
cThis department saw only female patients.
Facility-wide, the IHS study site demonstrated a significant increase in chlamydia screening from 2011 to 2015: 24.0% (2075 of 8638) pre–EHR reminder implementation to 27.9% (2370 of 8485) and 27.3% (2294 of 8407) in year 1 and year 2 post–EHR reminder implementation, respectively (Table 1). The proportions of chlamydia screening performed increased significantly from pre–EHR to post–EHR reminder implementation in the 5 departments that attended the chlamydia screening awareness presentation (Table 1). The internal medicine clinic improved most, increasing from 28.2% (108 of 383) pre–EHR reminder implementation to 61.1% (253 of 414) in year 1 and 57.1% (254 of 445) in year 2 post–EHR reminder implementation. The chlamydia screening rate declined significantly in obstetrics–gynecology, from 87.2% (536 of 615) pre–EHR reminder implementation to 79.4% (432 of 544) in year 2 post–EHR reminder implementation. Trends in female-specific chlamydia screening rates were similar to trends overall (Table 2). Facility-wide rates increased significantly, from 35.2% (1709 of 4862) pre–EHR reminder implementation to 38.1% (1808 of 4751) in year 1 and 37.2% (1764 of 4737) in year 2 post–EHR reminder implementation. The internal medicine clinic demonstrated the largest increase in screening rates: 35.8% (69 of 193) pre–EHR reminder implementation to 65.8% (133 of 202) in year 1 and 61.1% (140 of 229) in year 2 post–EHR reminder implementation, a peak 83.8% relative increase. Female-specific chlamydia screening rate increases in the pediatric clinic were significant only by year 2 post–EHR reminder implementation (28.6% [88 of 308] to 36.0% [126 of 350]), a 25.9% relative increase.
Number of chlamydia screenings among females, by clinical department, as a percentage of all female chlamydia screening–eligible patients before and after implementation of an electronic health record (EHR) reminder intervention at an Indian Health Service facility in the US Southwest, 2011-2015 a
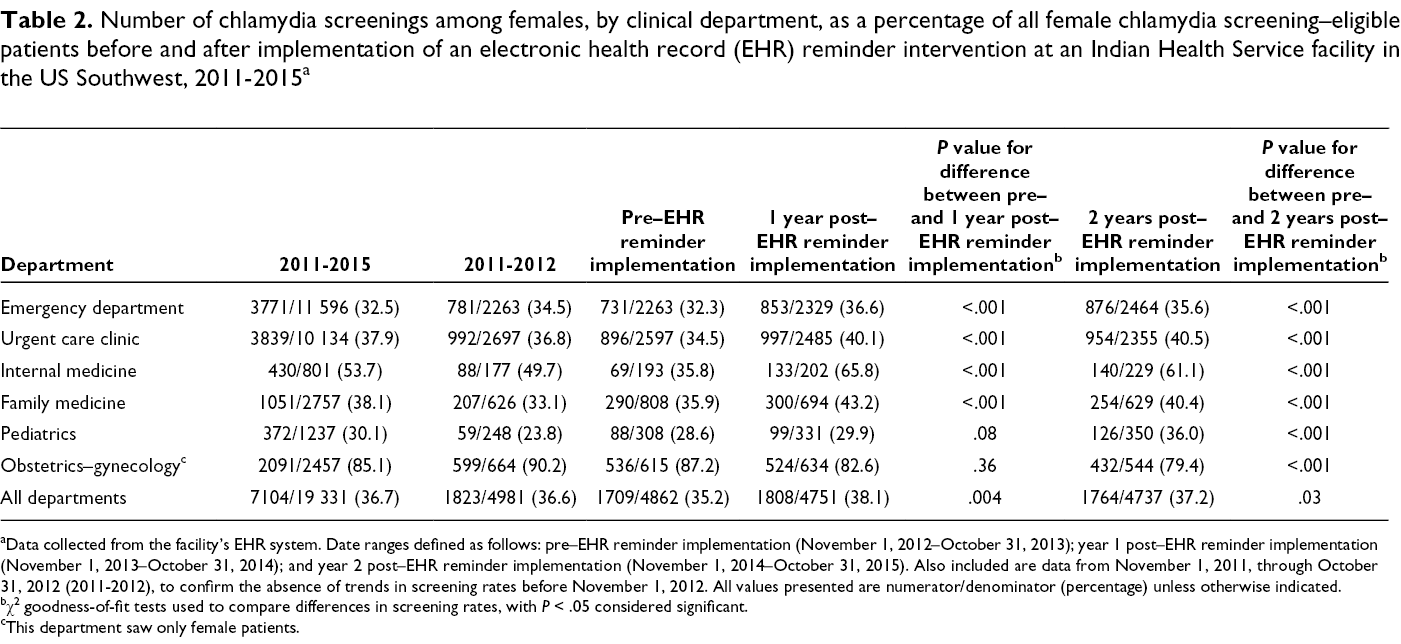
aData collected from the facility’s EHR system. Date ranges defined as follows: pre–EHR reminder implementation (November 1, 2012–October 31, 2013); year 1 post–EHR reminder implementation (November 1, 2013–October 31, 2014); and year 2 post–EHR reminder implementation (November 1, 2014–October 31, 2015). Also included are data from November 1, 2011, through October 31, 2012 (2011-2012), to confirm the absence of trends in screening rates before November 1, 2012. All values presented are numerator/denominator (percentage) unless otherwise indicated.
bχ2 goodness-of-fit tests used to compare differences in screening rates, with P < .05 considered significant.
cThis department saw only female patients.
Discussion
In this retrospective study, an IHS facility combined EHR reminders with a data-driven awareness presentation to clinical departments and health care providers and elicited feedback from health care providers to develop novel screening policies in an ongoing improvement process. Such an approach, integrating multiple modalities previously shown to increase screening rates, 10 was correlated with sustained improvement in chlamydia screening rates during a 2-year evaluation period. EHR reminders alone—without the awareness presentation—had no positive effect, although only 1 clinical department did not receive the awareness presentation. Our findings suggest that EHR reminder systems coupled with adjunct measures, such as an awareness presentation, could result in lasting effects on hospital screening rates for chlamydia and other STDs.
Although small, our study’s EHR component is similar to EHR components in other investigations. 8 -12,14 -19 Studies have shown, however, that EHR reminders alone have a limited positive effect on preventive care: in a review of 28 trials of EHR-based screening reminders, the median improvement rate for the measures evaluated was 4.2%. 14 -19 “Alert fatigue”—induced by information overload—may limit the benefits of EHR reminder systems. Evaluations of alert fatigue and barriers to clinical decision support systems highlight the effect of these factors on health care providers. 20 -23 Other strategies to increase STD screening have included, in isolation, recruiting champions of STD screening and implementing cognitive interventions (eg, guiding health care providers through workshops to increase confidence in offering chlamydia screening). 10,24
Without a control cohort, we cannot rigorously attribute any increase in screening to our awareness presentation alone. We do, however, suggest that the awareness presentation may have had some effect: the lack of increase in chlamydia screening rates in obstetrics–gynecology may have been due to a lack of awareness about health care provider performance. All clinics had significant increases in screening from pre–EHR reminder implementation to year 1 and year 2 post–EHR reminder implementation. In addition, the awareness presentation qualitatively induced discussion and development of new screening protocols, most prominently in internal medicine and pediatrics. The nonsignificant decline during year 2 post–EHR reminder implementation in 4 clinics may have been due to a lack of awareness of health care provider performance during that period; the effect of the intervention may decline if feedback on the performance of health care providers is not sustained.
We found that internal medicine and pediatrics, the 2 clinical departments each consistently seeing <7% of chlamydia screening–eligible patients and accounting for <10% of chlamydia screenings performed in the IHS facility, demonstrated the most improvement in screening rates. In comparison, the emergency department and the urgent care clinic, together seeing approximately two-thirds of chlamydia screening–eligible patients and accounting for approximately half of the chlamydia screenings performed in the IHS facility, demonstrated small improvements in screening rates. The cause of this difference was likely multifactorial: the emergency department and urgent care clinic are not traditionally viewed as responsible for chlamydia screening and, thus, may not have adjusted their clinical practices to the extent that the internal medicine or pediatrics departments did. For a minority of chlamydia screening–eligible patients, patient preferences or extenuating circumstances, such as cultural barriers, may have precluded chlamydia screening.
The overall short-term increases in chlamydia screening we observed at the IHS study site were, thus, modest. At a systems level, we note several obstacles, the most prominent of which were health care provider turnover and transient shortages of health care providers. Other persistent barriers to increases in chlamydia screening rates at our IHS facility exist at a population level. Traditionally, discussion of sexual practices is considered taboo in the culture of some AI/AN tribes. We felt that screening policies organically developed with the help of health care providers who have daily contact with American Indian patients would be those most likely to navigate barriers to increased screening. Most strikingly, the facility’s emergency department recently developed an automated chlamydia screening protocol for all screening-eligible patients that incorporates testing during the emergency department encounter with outpatient follow-up by a public health nurse, similar in design to other STD screening protocols. 25 Several other departments continue to develop additional chlamydia screening policies.
Non–clinic-based STD screening protocols are of interest because of their capacity to reach populations at risk of STDs who engage sporadically with the health care system. Several studies have demonstrated the efficacy of such protocols in these populations. 26 -28 In particular, an observational cohort study published in 2015 reported high response rates and positive feedback for self-administered STD screening tests among young AI/AN adults. 25 Given the implementation of new chlamydia screening protocols in the emergency department and urgent care clinic at our IHS study site, we anticipate increases in chlamydia screening rates in the immediate future.
Future strategies for improving chlamydia screening rates will continue to involve non–clinic-based STD screening with self-swab or self-collection and follow-up by a public health nurse. HIV case detection rates increased substantially at clinics in North Carolina that have routine, opt-out HIV testing programs; such practices might be applied to increase chlamydia screening rates. 29 An express testing system, consisting of urine/serum specimen submission without physical examination, resulted in increased chlamydia screening rates and cost savings. 30 Chlamydia screening among AI/AN populations occurs most frequently during prenatal care visits, family planning/contraception visits, and visits for STD symptoms; we hope to develop protocols for health care engagement at these points of contact. 5
Limitations
This study had several limitations. First, without control groups, we could not determine whether the combined components of the intervention were significantly more effective than each component alone. However, our findings have empirical value. We lend further support to the concept that pairing EHR reminders with an awareness presentation may result in increased screening of diseases, and we hope to spark further application of the concept across other quality improvement areas. Second, our study was limited by the lack of patient medical record review and a relative paucity of patient data; use of patient records would have allowed us to validate our algorithms with medical record review via statistical sample analysis. We controlled for a lack of individualized patient data by externally validating our logic with independent database experts at the IHS study site. Third, the increases in chlamydia screening rates at the facility may have been artificially dampened by the large proportion of women who used obstetrics–gynecology as their sole point of health care contact.
A potential fourth limitation is that we queried data for both male and female patients according to USPSTF recommendations. 2 Although the USPSTF has not found sufficient evidence that regular chlamydia screening among males should occur, it does recommend at least a consideration of screening males in areas with high prevalence of this disease. Asymptomatic chlamydial infections in both men and women may be an important reservoir of recurrent infection. Given the large prevalence of chlamydia in our catchment area and USPSTF recommendations, we deemed that a screening protocol for both sexes with an expanded age range was appropriate for our patient population.
Conclusions
Measuring outcomes and sharing performance results are best integrated into clinical processes. Screening rates appear to be enhanced through reinforcement, such as health care provider–specific performance feedback. Budgetary constraints, gaps in patient education, and delays in obtaining the results of testing with potential lack of follow-up are additional practical limiting factors. In a busy clinical setting, EHR reminders alone may not be enough to improve important quality measures, and alert fatigue may play a role. EHR reminders are optimally combined with enhanced provider awareness and solicitation of provider feedback, to galvanize the development of novel facility-specific screening policies. Other clinical strategies, including automated testing protocols, may also add benefit. Although STD testing and other preventive care may be more appropriately triaged to follow-up care clinics in an emergency department or urgent care setting, the challenges of follow-up in specific patient populations must be considered.
Footnotes
Acknowledgments
Dr Hughes is currently affiliated with Johns Hopkins Medical Institutions, Baltimore, Maryland.
Authors’ Note
The findings expressed in this presentation are those of the authors and do not necessarily reflect the views of the Indian Health Service.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support with respect to the research, authorship, and/or publication of this article.