
Abstract
The incidence of syphilis infections is on the rise, particularly among African American men and men who have sex with men, and it is reaching epidemic levels in these communities throughout the United States. Although syphilis is relatively inexpensive to treat and cure and is a predictor for HIV incidence among men and transgender women who have sex with men, rates of co-screening for syphilis are low in the emergency department setting, with a dearth of literature on this topic since the 1990s and early 2000s. In this case study, we describe an operational model for routine syphilis screening implemented in June 2017 at the University Hospitals Cleveland Medical Center in Cleveland, Ohio. We describe the advantages of screening using a reverse testing algorithm rather than the traditional method and the necessity of partnering with the Cleveland Department of Public Health for both diagnostic and follow-up logistics.
Keywords
The trend of routinizing screening for HIV infection in US emergency departments (EDs) has led to an increase in the number of patients linked to care and initiating antiretroviral treatment. 1,2 The increase in screening has led not only to the development of more efficient, validated screening tools, such as the Denver HIV Risk Score, 3,4 but also to co-testing for other chronic infections, such as hepatitis C virus, and highlights the importance of the ED’s role in public health interventions. 5,6
The incidence of syphilis infections is on the rise, particularly among African American men and men who have sex with men, and it is reaching epidemic levels in these communities throughout the United States. 7 Although syphilis infection is relatively inexpensive to treat and cure and is a predictor for HIV infection among men and transgender women who have sex with men, 8 co-screening occurs infrequently in the ED setting. 9,10 Historically, the initial test for syphilis screening has involved a labor-intensive nontreponemal test (rapid plasma reagin). Recently, however, the reverse testing algorithm has proved noninferior, even superior, to the traditional algorithm (Figure 1). 11 -14 It begins with an automated treponemal test (immunoglobulin G [IgG]) performed on a Siemens ADVIA Centaur Syphilis Assay, which provides results within hours. Compared with the nontreponemal test, the reverse testing algorithm at the population level is slightly more costly and may result in treatment of false-positives. 15
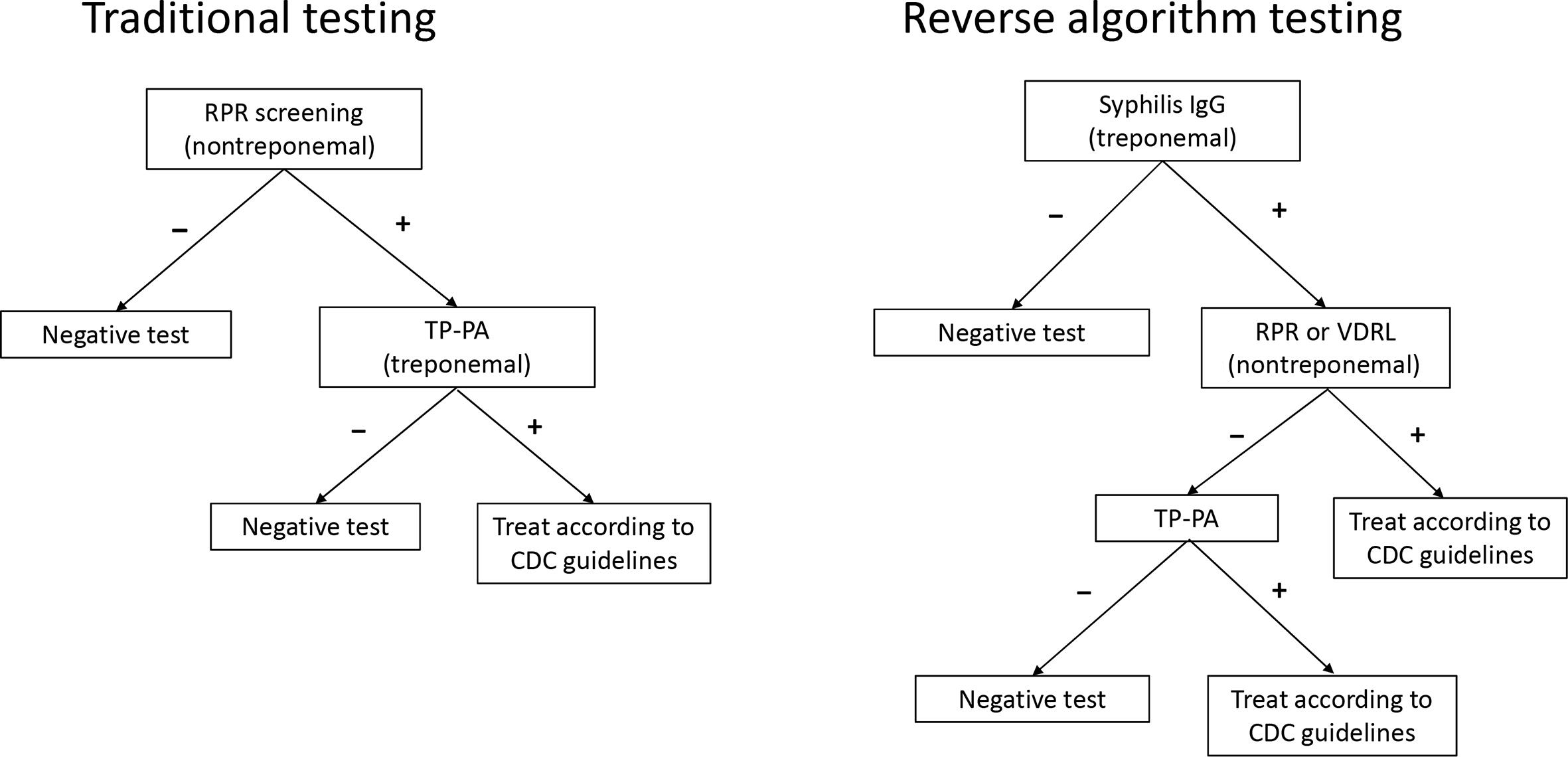
Traditional syphilis testing vs reverse algorithm testing. Traditional testing begins with a nontreponemal study, which is labor intensive and dependent on subjective interpretations of results. The reverse algorithm testing method uses a treponemal test (immunoglobulin G [IgG] or total antibody) for initial screening, which can be performed quickly on automated immunoassay analyzers and allows for greater throughput. Treponemal screening may also be more sensitive in detecting cases of secondary and late or latent syphilis. Abbreviations: CDC, Centers for Disease Control and Prevention; RPR, rapid plasma reagin; TP-PA, treponema pallidum particle agglutination assay; VDRL, venereal disease research laboratory.
Research on syphilis testing in the ED conducted in the early 1990s and 2000s showed that ED physicians do not routinely test for syphilis based on Centers for Disease Control and Prevention recommendations 16 ; it also documented the prevalence of syphilis and the demographic characteristics of patients with syphilis in single-institution studies. 16 -18 Since then, the scientific literature on syphilis testing in the ED has been scant. A study published in 2019 examined the evaluation of rapid syphilis testing in the ED. 19 A commentary published in 2020 describes how ED physicians from the University of Chicago used the electronic health record to bundle syphilis testing with HIV testing, which led to a dramatic increase in monthly syphilis testing (from 250 tests to >1200 tests per month) and high rates of positivity. 20 A study published in 2020 describes how the ED at Homestead Hospital in Miami–Dade County, Florida, similarly triggered syphilis testing as part of its routine HIV/hepatitis C virus opt-out screening infrastructure when patients presented with symptoms associated with sexually transmitted infections. 21 Using a reverse testing algorithm, the authors of that study tested 4806 patients, of whom 59 were confirmed positive for syphilis. Although early data from the 1990s suggest computerized reminders in the electronic health record do not increase testing, 22 advances in technology and a renewed focus on public health might explain differences in syphilis testing with computerized reminders across 3 decades.
Despite recent research, literature on how to set up a syphilis screening program in the ED is lacking. In this case study, we describe the rationale and operational model for, and the preliminary outcomes of, a syphilis screening program in the ED at an urban level 1 trauma center in East Cleveland, Ohio.
Purpose
Ohio had 1221 cases of syphilis in 2018 (740 cases of primary and secondary syphilis and 481 cases of early latent syphilis), a steady increase from previous years. 23 The incidence of syphilis has risen steadily (from 2.3 to 12.7 cases per 100 000 population from 2013 to 2017) in Cuyahoga County, Ohio, particularly among African American men aged 20-44. 23 University Hospitals Cleveland Medical Center (UHCMC) is a level 1 trauma center in Cuyahoga County serving a >95% African American population from East Cleveland. Many patients receive their primary care from this location, and many are seen for symptomatic sexually transmitted diseases. Testing for syphilis with a single point-of-care test in the ED is not commonly implemented because of the poor performance of some point-of-care tests and the limited positive predictive value of the results given the relatively low prevalence of disease in certain populations. 24,25
IgG antibodies (automated treponemal test) or rapid plasma reagin (nontreponemal test) are common initial tests for the diagnosis of syphilis; however, IgG antibodies (and in some circumstances nontreponemal tests) can remain positive long after treatment of the disease. Therefore, a single test in the ED is not adequate to make a conclusive diagnosis of active syphilis. 26 Secondary confirmatory tests, which return results within 24-48 hours and require follow-up by the ED physician who ordered the test, are needed to differentiate between a positive result indicating an active or untreated infection and a positive result indicating a previously treated infection (ie, a false-positive result). 24,25 In the traditional testing algorithm, the initial test is a nontreponemal test, a manual and time-consuming test performed by laboratory personnel that is not suitable for high-volume screenings. However, because of the advent of enzyme immunoassays and fully automated chemiluminescent immunoassays, a reverse testing algorithm is now available, in which the initial test is the automated treponemal test. This test is completed quickly, is appropriate for large-scale screenings, and allows for detection of previous treated infection with improved specificity. 27,28
Despite a more automated reverse testing algorithm compared with nontreponemal testing, 29,30 the challenge persists that treponemal IgG antibodies often remain positive for life and even after treatment, although 15%-25% of patients treated during the primary stage may be serologically nonreactive after 2 or 3 years. 26 If a history of past treatment is not known, the interpretation of treponemal IgG antibodies is difficult. Syphilis screening tests are finalized long after the patient is discharged from the ED. As such, unless a history of syphilis infection and confirmed treatment is documented in the medical record, the ED physician, during or after shift, would have to call the department of health (because syphilis is a reportable disease, 31 the public health department usually has this information) or request medical records from other institutions to gather this information—an unrealistic if not overwhelming expectation. Thus, knowledge of a history of syphilis infection and treatment is critical to the decision to treat a patient who has a positive syphilis screening test that is then confirmed by reverse testing.
Cuyahoga County has seen a steady rise in the incidence of primary and secondary syphilis cases, from 2.3 cases per 100 000 population in 2013 to 12.7 cases per 100 000 population in 2017. 23 A similar increase occurred in the incidence of early latent syphilis cases during this period, from 0.9 cases per 100 000 population in 2013 to 5.0 cases per 100 000 population in 2017. 23 These increases are consistent with increases in numerous US cities. 32 In September 2017, the UHCMC Department of Emergency Medicine in collaboration with the MetroHealth Medical Center in Cleveland and the Cleveland Department of Public Health (CDPH) created the HIV/Syphilis Testing and Care Collaborative. This platform (Table) has introduced syphilis screening to our standardized protocol for HIV screening. The HIV/Syphilis Testing and Care Collaborative was viewed as exempt by the University Hospitals Institutional Review Board and was classified as a quality improvement project.
Title, location, and role of participants in the HIV/Syphilis Testing and Care Collaborative, University Hospitals Cleveland Medical Center, Cuyahoga County, Ohio, 2014-2018 a
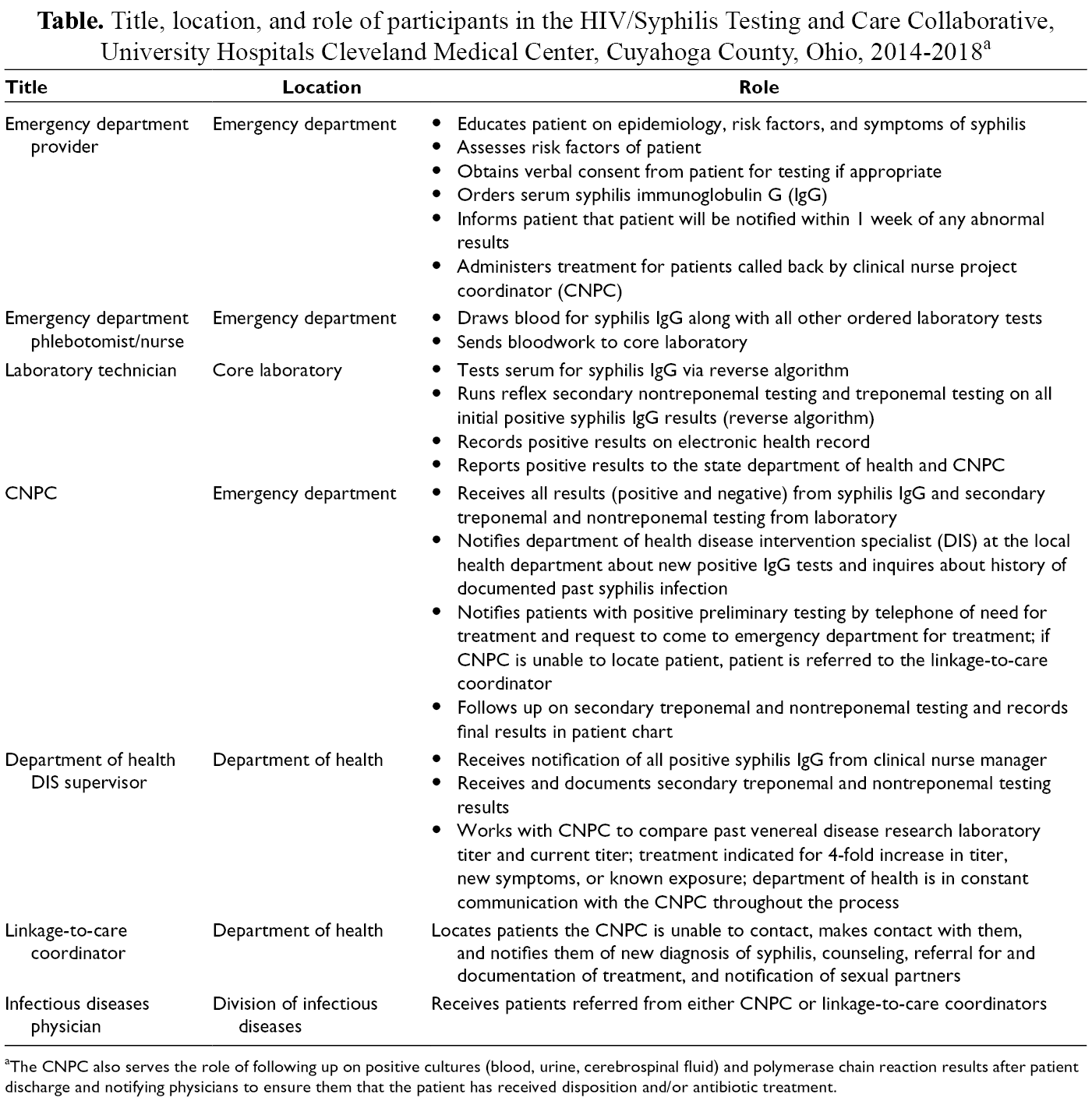
aThe CNPC also serves the role of following up on positive cultures (blood, urine, cerebrospinal fluid) and polymerase chain reaction results after patient discharge and notifying physicians to ensure them that the patient has received disposition and/or antibiotic treatment.
Methods
To put syphilis testing in the ED into a clinical perspective, it is important to understand not only the fast-paced environment of the ED but also the time frame in which all laboratory tests return in relation to others. In our ED, it is standard to test for treponemal IgG antibodies and HIV antibody/antigen (opt-out screening) concomitantly with gonorrhea/chlamydia by nucleic acid amplification testing (NAAT) and trichomonas testing by wet preparation with reflex to NAAT. The turnaround time for the treponemal IgG antibodies (preliminary result), the HIV 1/2 antigen/antibody test (preliminary result), and the wet preparation (final result) is approximately 1 hour, whereas the gonorrhea/chlamydia/trichomonas NAAT and any positive syphilis or HIV confirmatory testing finalizes in 24-72 hours—long after the patient is discharged. If patients leave the ED before test results are available, they are given a discharge sheet explaining the process of testing follow-up and linkage to care if treatment is needed. Our clinical nurse project coordinator follows all syphilis and HIV confirmation testing and the gonorrhea/chlamydia/trichomonas NAAT performed in the ED and then contacts patients with positive results to facilitate treatment and follow-up. All positive HIV and syphilis tests are referred to CDPH.
Laboratory analysis of all syphilis tests systemwide are performed at our core laboratory on the UHCMC main campus using the reverse testing algorithm. Initial screening in the ED consists of treponemal IgG antibodies (treponemal test) by chemiluminescent immunoassays. If a serum automated treponemal test is positive, a serum venereal disease research laboratory (VDRL, a nontreponemal blood test) is performed. If both tests are positive, this result indicates an active, recently treated, or incompletely treated syphilis infection, and treatment is indicated. For positive automated treponemal test/negative VDRL results, another treponemal test, the treponema pallidum particle agglutination assay (TP-PA), is performed. A treponemal-positive/VDRL-negative/TP-PA–positive test indicates a latent or previously treated syphilis case, whereas a negative TP-PA indicates a false-positive automated treponemal test. For treponemal-positive/VDRL-negative/TP-PA–positive testing, current titers are compared with archived titers at the CDPH, and treatment is indicated for a 4-fold increase in titer, reported new symptoms, or known reexposure to syphilis.
Because syphilis is a reportable disease, 31 and because CDPH’s health information repository is statewide, we can determine a history of syphilis treatment more effectively by accessing CDPH’s health information repository than by examining UHCMC’s electronic health records. CDPH’s health information repository is particularly useful in cities where multiple health care systems operate. Furthermore, public health infrastructure exists through CDPH to ensure linkage to care and patient notification, which is available without additional cost. The collaboration between CDPH and UHCMC relieves the burden on the ED physician, who would otherwise be responsible for follow-up, interpretation of test results, and linkage to care.
Outcomes
From June 1 to November 31, 2018, we screened 1122 patients for syphilis at the UHCMC ED. Nearly all patients were screened in our low-acuity “fast track” (Figure 2), were aged <40 years, and were African American. We identified 38 (3.4%) syphilis treponemal-positive samples: 26 were from patients with a previous diagnosis and treatment, and 4 were false-positives. Overall, we diagnosed 8 (0.7%) new cases of syphilis among high-risk, sexually active patients who were asymptomatic for syphilis at the time of screening and otherwise would not have been diagnosed. All received treatment according to Centers for Disease Control and Prevention recommendations. The cost of these tests in our hospital system were bundled into the cost of the ED patient encounter.
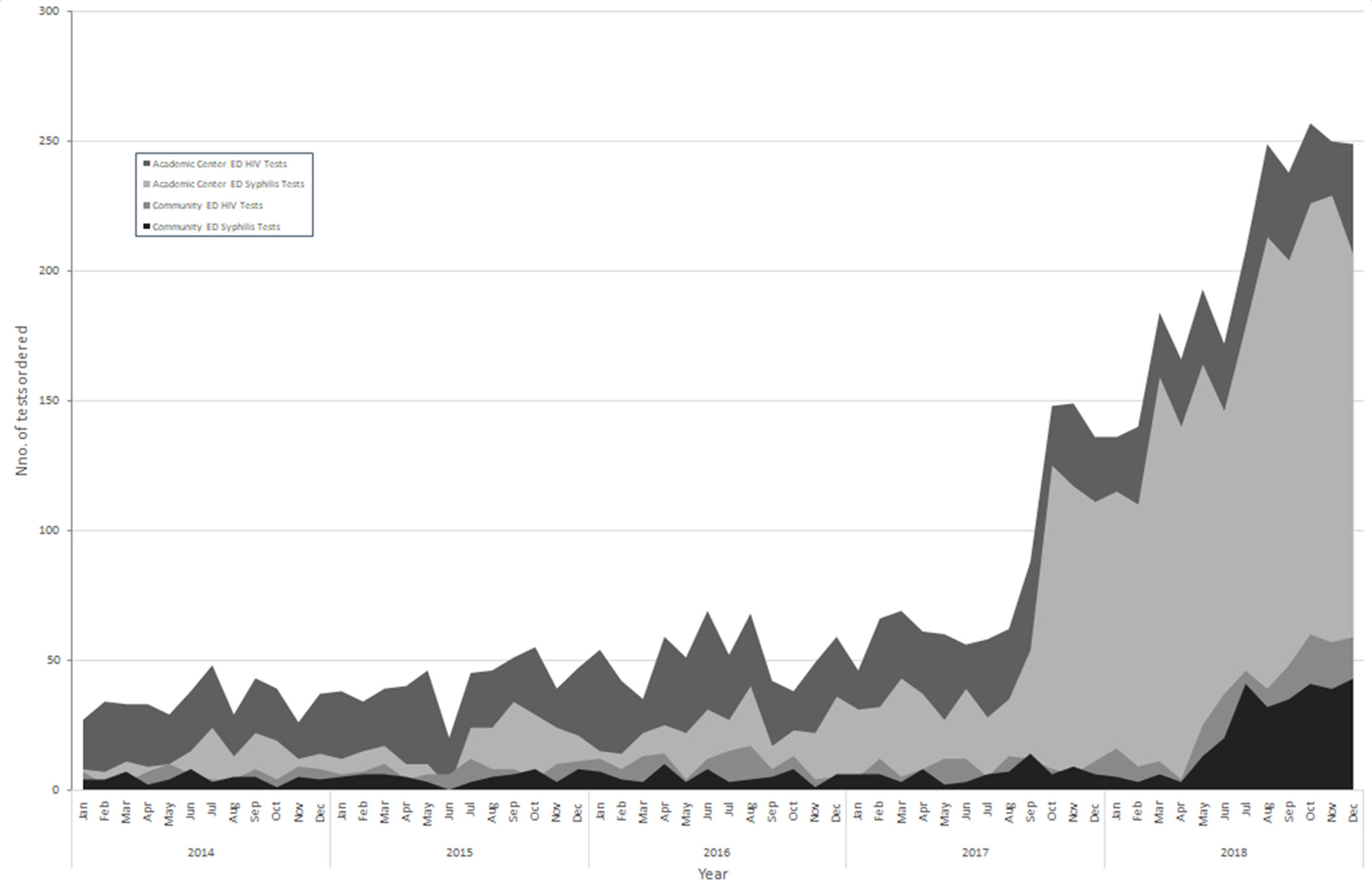
Outcomes of the HIV/Syphilis Testing and Care Collaborative (HIVTCC), University Hospitals Cleveland Medical Center, Cuyahoga County, Ohio, 2014-2018. The graph shows trends in the number of HIV tests and syphilis tests performed at the UHCMC main campus (UHCMC emergency department [ED]) compared with the trend of testing in the community after implementation of the HIVTCC in June 2017. Education began at the main campus and gradually filtered into the community, likely explaining the 9-month lag in the rise of testing in the community EDs.
Lessons Learned
The epidemiological trend of increased incidence of syphilis infections among marginalized populations who use the ED for care, including cities such as Cleveleand, 33,34 suggests that this clinical environment may benefit from co-testing of syphilis along with other sexually transmitted infections. 35,36 Syphilis testing is more complicated than HIV screening because of the use of both traditional and reverse testing algorithms and the dependence on knowledge of past infection and treatment. To overcome these challenges, the UHCMC HIV/Syphilis Testing and Care Collaborative uses the reverse testing algorithm, starting with the automated treponemal test and, when this test is positive, additional testing with VDRL. The automated treponemal test is especially useful for mass screening because it has a quick turnaround time and requires less manual labor than initial nontreponemal testing in the traditional algorithm. Another way to overcome the challenges with syphilis testing is the creation of a robust, collaborative initiative among the ED, department of infectious diseases, core laboratory, and local health department for routine syphilis screening in the ED, and the success of this program depends on buy-in from all of these entities, along with ED administration. This collaboration moves the onus of patient follow-up from the ED physician to another entity (CDPH) so that ED throughput is not negatively affected. The collaboration benefits from access to the archived records of known syphilis infections throughout Ohio, historical data on patient titers, and the resources of the county to follow up on and treat people with newly diagnosed syphilis. From an operational perspective, we recommend a similar setup for EDs interested in syphilis screening, particularly in high-incidence states such as Florida, Georgia, New York, and Texas, each of which has an incidence of syphilis that is 2-3 times that of Ohio; the incidence in California is 8 times higher than in Ohio. 37
The model presented here can either be replicated as a stand-alone program or incorporated into an ED-based HIV screening program that uses serum-based testing. Although the model may be slightly more costly for EDs that do not bundle the cost of care, 14 it is designed to increase the definitive treatment of undiagnosed syphilis among vulnerable populations by minimizing barriers to screening, 28 which maximizes buy-in from ED providers. In addition, this model may facilitate buy-in by minimizing the work of testing follow-up by ED physicans, which is an unrealistic if not impossible task in the busy ED setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the AIDS Funding Collaborative.