
Abstract
Objectives
Childcare is an important setting for nutrition; nearly half of young children in the United States participate in licensed childcare, where they consume up to two-thirds of their daily dietary intake. We compared state regulations for childcare with best practices to support breastfeeding and healthy beverage provision.
Methods
We reviewed regulations for childcare centers (centers) and family childcare homes (homes) in effect May–July 2016 and rated all 50 states for inclusion (1 = not included, 2 = partially included, 3 = fully included) of 12 breastfeeding and beverage best practices. We calculated average ratings for 6 practices specific to infants aged 0-11 months, 6 practices specific to children aged 1-6 years, and all 12 practices, by state and across all states. We assessed significant differences between centers and homes for each best practice by using McNemar–Bowker tests for symmetry, and we assessed differences across states by using paired student t tests.
Results
States included best practices in regulations for centers more often than for homes. Average ratings (standard deviations) in regulations across all states were significantly higher in centers than in homes for infant best practices (2.1 [0.5] vs 1.8 [0.5], P < .001), child best practices (2.1 [0.6] vs 1.8 [0.6], P = .002), and all 12 best practices combined (2.1 [0.5] vs 1.8 [0.6], P < .001).
Conclusions
Although best practices were more consistently included in regulations for centers than for homes, many state childcare regulations did not include best practices to support breastfeeding and the provision of healthy beverages. Findings can be used to inform efforts to improve regulations and to reduce differences between centers and homes.
Nearly half of children younger than age 5 in the United States regularly attend licensed childcare, 1 where they receive up to two-thirds of their daily nutrition. 2 Nearly 1 in 6 children aged 2-5 years in the United States has obesity. 3 Exclusively breastfeeding for the first 6 months of life may reduce a child’s risk of obesity, 4 and childcare is associated with early weaning from breastfeeding. 5 Consumption of sugar-sweetened beverages contributes to obesity, 6 and childcare is associated with higher sugar-sweetened beverage consumption in children. 7 However, policies that support breastfeeding and encourage healthy beverages in childcare can improve children’s beverage nutrition and may help prevent obesity.8,9
Organized childcare, often subdivided into childcare centers (centers) and family childcare homes (homes), are required to be licensed in nearly all states. Although legal definitions for centers and homes vary by state, centers often care for more children, have more staff members, and have larger facilities than homes. Regulations may differ for centers and homes across the United States because each state has oversight of regulations. In addition to state regulations, licensed centers and homes can participate in the federal Child and Adult Care Food Program (CACFP), which provides reimbursement for meals and snacks that follow standards on infant formula, breast milk, milk, juice, water, and food served to income-eligible infants and children. 10 In some states, licensed centers and/or homes are mandated to meet CACFP nutrition standards regardless of CACFP participation. The CACFP standards were updated in 2017 to allow centers and homes to be reimbursed for expressed breast milk or when a mother directly breastfeeds a child on-site. 10 The updates further restricted juice from being served more than once per day and required that milk for children aged 1 year be unflavored whole milk and that milk for children aged 2-5 years be unflavored 1% or fat-free milk. 10
The objectives of this study were to (1) describe variations in best practices for breastfeeding and beverages among infants and children included in childcare licensing and administrative regulations in all 50 states and (2) identify differences in best practices for breastfeeding and beverages between centers and homes.
Methods
Data Collection
In this cross-sectional study, we used legal analytic methods to evaluate childcare licensing and administrative regulations for homes and centers in all 50 states for inclusion of best practices related to nutrition, as previously described. 11 Briefly, the evaluation focused on reviewing regulations for childcare settings that were identified on state government websites and downloaded from May to July 2016. We identified nutrition best practices within the regulations for obesity prevention with either demonstrated evidence for effectiveness in the published literature or practices identified by the American Academy of Pediatrics, American Public Health Association, and the National Resource Center for Health and Safety in Child Care and Early Education. 12 Four independent researchers (2 research staff members at the Harvard T.H. Chan School of Public Health and 2 postdoctoral fellows at the Johns Hopkins Bloomberg School of Public Health) coded regulations into 4 categories for inclusion of best practices in regulations using a common research tool with standardized coding guidelines. The categories were “not addressed or mentioned,” “partially met or recommended,” “fully met or required,” and “not applicable/known statutory impact.” 11 Known statutory impact refers to state-specific laws that apply to childcare providers that are not included in state childcare licensing or administrative regulations. The coders used the category “not applicable” for 1 state (Louisiana) in which homes are exempt from licensure; we included no regulations for homes in Louisiana in the review. The coders used the category “known statutory impact” for 1 state (California), which has a childcare beverage law that is separate from regulations. 13 The coders coded states as “mixed” when they had different regulations across various classifications of centers and/or homes (eg, small day care centers, infant care centers, small and large day care homes, group childcare homes). The coders further categorized best practices into those specific to infants (aged 0-11 months) and those specific to children (aged 1-6 years) or if they applied to both infants and children (for 1 best practice related to CACFP; Table 1).
Breastfeeding and beverage best practices and coding for inclusion in childcare regulations, United States, 2016 a
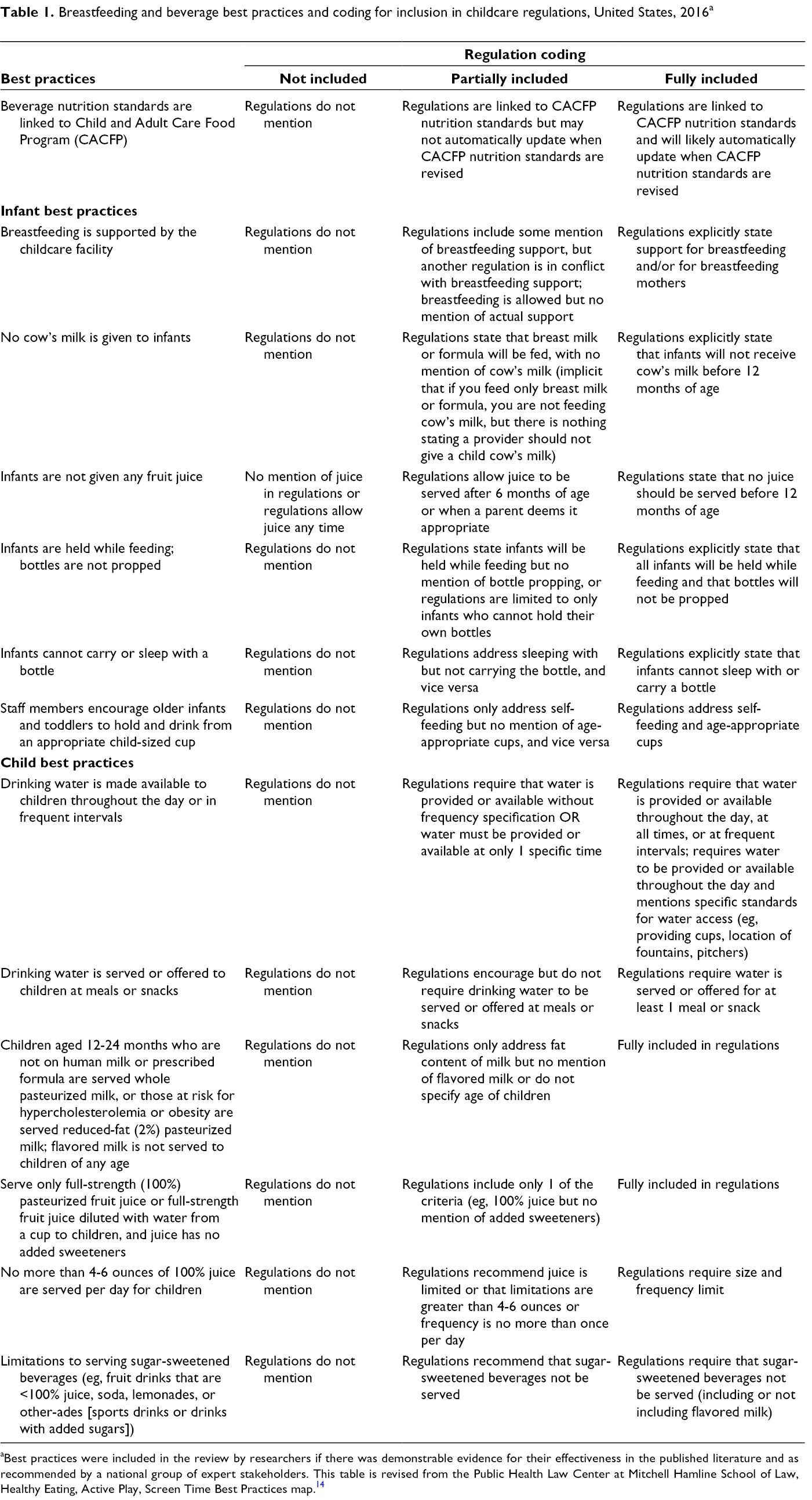
aBest practices were included in the review by researchers if there was demonstrable evidence for their effectiveness in the published literature and as recommended by a national group of expert stakeholders. This table is revised from the Public Health Law Center at Mitchell Hamline School of Law, Healthy Eating, Active Play, Screen Time Best Practices map. 14
In 2018, 2 researchers (R.T. and S.N.) independently recoded the data set (1 = not included, 2 = partially included, or 3 = fully included) using EpiData Software (Odense Denmark, EpiData Association). For the best practices for which California’s childcare beverage law applied, the researchers assigned ratings according to requirements found in the law. The researchers assigned ratings for states coded as mixed by selecting the type of center or home licensed to care for the greatest number of children; when the maximum number of children was not listed, researchers selected the type of care with “large,” “group,” or “certified” included in the name. (This occurred for Maryland, New Mexico, Oregon, West Virginia, and Tennessee.) The researchers evaluated each state for whether regulations were linked to CACFP nutrition standards and whether they were automatically updated (rated as 3) or not automatically updated (rated as 2) in response to federal revisions to CACFP nutrition best practices, such as revisions that occurred in 2017. 10 The 2 researchers (R.T. and S.N.) discussed the <5% of assigned ratings found to be discordant in EpiData to reach consensus for the final coding.
Final ratings for each state for inclusion of each best practice in regulations are available from the authors upon request. This study did not require institutional review board approval because it did not involve human subjects.
Data Analysis
We computed frequency and proportion by rating each of the 12 beverage best practices for all 50 states for centers and homes. We calculated differences in the inclusion of each best practice in state regulations between centers and homes using the McNemar–Bowker test of symmetry. We also calculated the mean (SD) of state ratings for the inclusion of best practices for infants, children, and infant and child best practices combined for all states. We calculated differences in average ratings between centers and homes for all states using a 2-tailed t test. We conducted all analyses using Microsoft Excel 15.27 (Microsoft Corporation) and Stata/SE version 15.1 (StataCorp LLC), with P < .05 considered significant. We developed visualizations of state ratings for center and home regulations using Tableau version 9.1 (Tableau Software, LLC).
Results
We found no significant differences in the proportion of states that did not include, partially included, or fully included CACFP nutrition standards in childcare regulations for centers and homes (Table 2). Eighteen states included CACFP nutrition standards in childcare regulations, which were automatically updated to the revised CACFP standards for centers (Alaska, Arkansas, Colorado, Connecticut, Georgia, Hawaii, Iowa, Louisiana, Minnesota, Montana, New Jersey, New Mexico, New York, North Carolina, Oklahoma, Rhode Island, South Carolina, and Utah), and 11 states included CACFP nutrition standards in childcare regulations for homes (Alaska, Arkansas, Connecticut [group day care homes], Hawaii, Iowa, New Mexico, North Carolina, Rhode Island, South Carolina [group childcare homes], Utah, and Washington). Twelve states included CACFP nutrition standards in childcare regulations but may not have automatically updated to the revised CACFP standards for centers (Alabama, California, Maryland, Massachusetts, Michigan, Nebraska [not preschools], North Dakota [not preschools], Ohio [not publicly funded childcare], Oregon, Virginia, West Virginia, and Wisconsin), and 12 states included CACFP nutrition standards in childcare regulations but may not have automatically updated to the revised CACFP standards for homes (Alabama, Delaware, Maryland, Massachusetts, Michigan, Montana, Nebraska, North Dakota, Ohio, Oregon, Virginia, and Wisconsin).
Difference between childcare centers and family childcare homes in frequency and proportion of states that included breastfeeding and beverage best practices in regulations, United States, July 2016 a
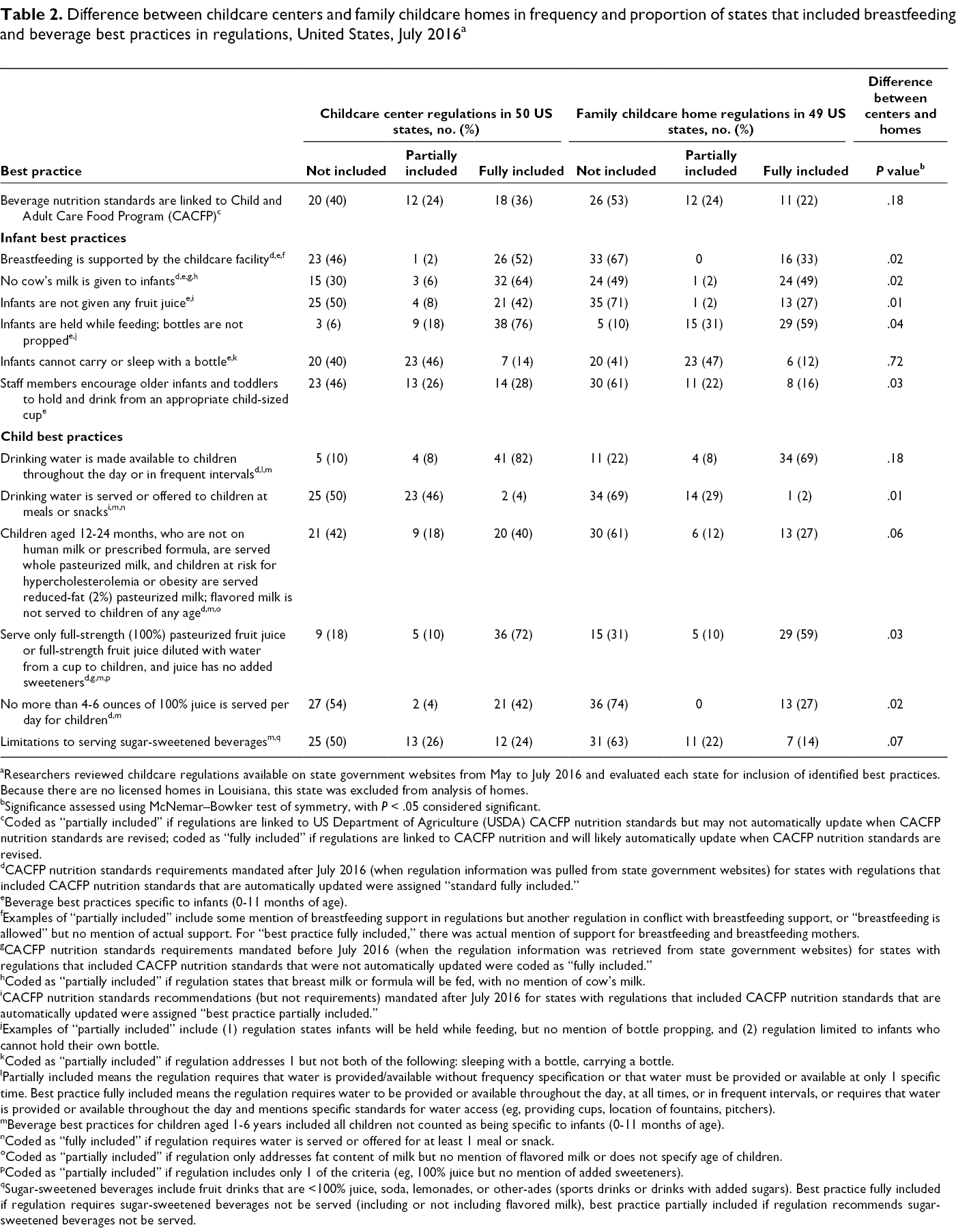
aResearchers reviewed childcare regulations available on state government websites from May to July 2016 and evaluated each state for inclusion of identified best practices. Because there are no licensed homes in Louisiana, this state was excluded from analysis of homes.
bSignificance assessed using McNemar–Bowker test of symmetry, with P < .05 considered significant.
cCoded as “partially included” if regulations are linked to US Department of Agriculture (USDA) CACFP nutrition standards but may not automatically update when CACFP nutrition standards are revised; coded as “fully included” if regulations are linked to CACFP nutrition and will likely automatically update when CACFP nutrition standards are revised.
dCACFP nutrition standards requirements mandated after July 2016 (when regulation information was pulled from state government websites) for states with regulations that included CACFP nutrition standards that are automatically updated were assigned “standard fully included.”
eBeverage best practices specific to infants (0-11 months of age).
fExamples of “partially included” include some mention of breastfeeding support in regulations but another regulation in conflict with breastfeeding support, or “breastfeeding is allowed” but no mention of actual support. For “best practice fully included,” there was actual mention of support for breastfeeding and breastfeeding mothers.
gCACFP nutrition standards requirements mandated before July 2016 (when the regulation information was retrieved from state government websites) for states with regulations that included CACFP nutrition standards that were not automatically updated were coded as “fully included.”
hCoded as “partially included” if regulation states that breast milk or formula will be fed, with no mention of cow’s milk.
iCACFP nutrition standards recommendations (but not requirements) mandated after July 2016 for states with regulations that included CACFP nutrition standards that are automatically updated were assigned “best practice partially included.”
jExamples of “partially included” include (1) regulation states infants will be held while feeding, but no mention of bottle propping, and (2) regulation limited to infants who cannot hold their own bottle.
kCoded as “partially included” if regulation addresses 1 but not both of the following: sleeping with a bottle, carrying a bottle.
lPartially included means the regulation requires that water is provided/available without frequency specification or that water must be provided or available at only 1 specific time. Best practice fully included means the regulation requires water to be provided or available throughout the day, at all times, or in frequent intervals, or requires that water is provided or available throughout the day and mentions specific standards for water access (eg, providing cups, location of fountains, pitchers).
mBeverage best practices for children aged 1-6 years included all children not counted as being specific to infants (0-11 months of age).
nCoded as “fully included” if regulation requires water is served or offered for at least 1 meal or snack.
oCoded as “partially included” if regulation only addresses fat content of milk but no mention of flavored milk or does not specify age of children.
pCoded as “partially included” if regulation includes only 1 of the criteria (eg, 100% juice but no mention of added sweeteners).
qSugar-sweetened beverages include fruit drinks that are <100% juice, soda, lemonades, or other-ades (sports drinks or drinks with added sugars). Best practice fully included if regulation requires sugar-sweetened beverages not be served (including or not including flavored milk), best practice partially included if regulation recommends sugar-sweetened beverages not be served.
We found significant differences between centers and homes in the proportion of states that did not include, partially included, or fully included best practices in regulations for 5 infant best practices and 3 child best practices (Table 2). A higher proportion of states were more likely to fully include best practices in regulations for centers than for homes for the following infant best practices: breastfeeding is supported by the childcare facility, cow’s milk is given to infants, infants are not given any fruit juice, infants are held while feeding (bottles are not propped), and staff members encourage older infants and toddlers to hold and drink from an appropriate child-sized cup. The 3 child best practices that were more common among centers than among homes were drinking water is served or offered to children at meals or snacks, providers serve only full-strength (100%) pasteurized fruit juice or full-strength fruit juice diluted with water from a cup to children and juice has no added sweeteners, and no more than 4-6 ounces of 100% juice is served per day for children.
The infant best practice “infants are held while feeding and bottles are not propped” was fully included in regulations by most states for centers (76%) and homes (59%; Table 2). The infant best practice “infants cannot carry or sleep with a bottle” was the least likely best practice to be fully included for centers (14%) and homes (12%). The child best practice “drinking water is made available to children throughout the day or in frequent intervals” was fully included in regulations by most states for centers (82%) and homes (69%). The child best practice “drinking water is served or offered to children at meals or snacks” was fully included by few states for centers (4%) and homes (2%). The child best practice “limitations to serving sugar-sweetened beverages” (which included provisions such as fruit drinks that are <100% juice, soda, lemonades, sports drinks, or drinks with added sugars) was also fully included in only 12 states for centers (Arizona, California, Colorado, Illinois, Indiana, Maryland, Mississippi, New Jersey, New York, North Carolina, Oklahoma, and Rhode Island) and 7 states for homes (Arizona, California, Maryland, Mississippi, New York, North Carolina, and Rhode Island).
For centers, the states with the highest average ratings were Colorado, Montana, New Jersey, New Mexico, New York, Oklahoma, and Rhode Island (all 2.8), and the states with the lowest average ratings were Idaho (1.0), South Dakota (1.1), and Maine, Pennsylvania, and Wyoming (all 1.2; Figure 1). For homes, the states with the highest average ratings were Rhode Island (2.8), New Mexico (2.8), and North Carolina (2.7), and the states with the lowest average ratings were Idaho (1.0), Maine (1.1), and South Dakota (1.1; Figure 2). No state fully included all infant and child best practices for centers or homes.
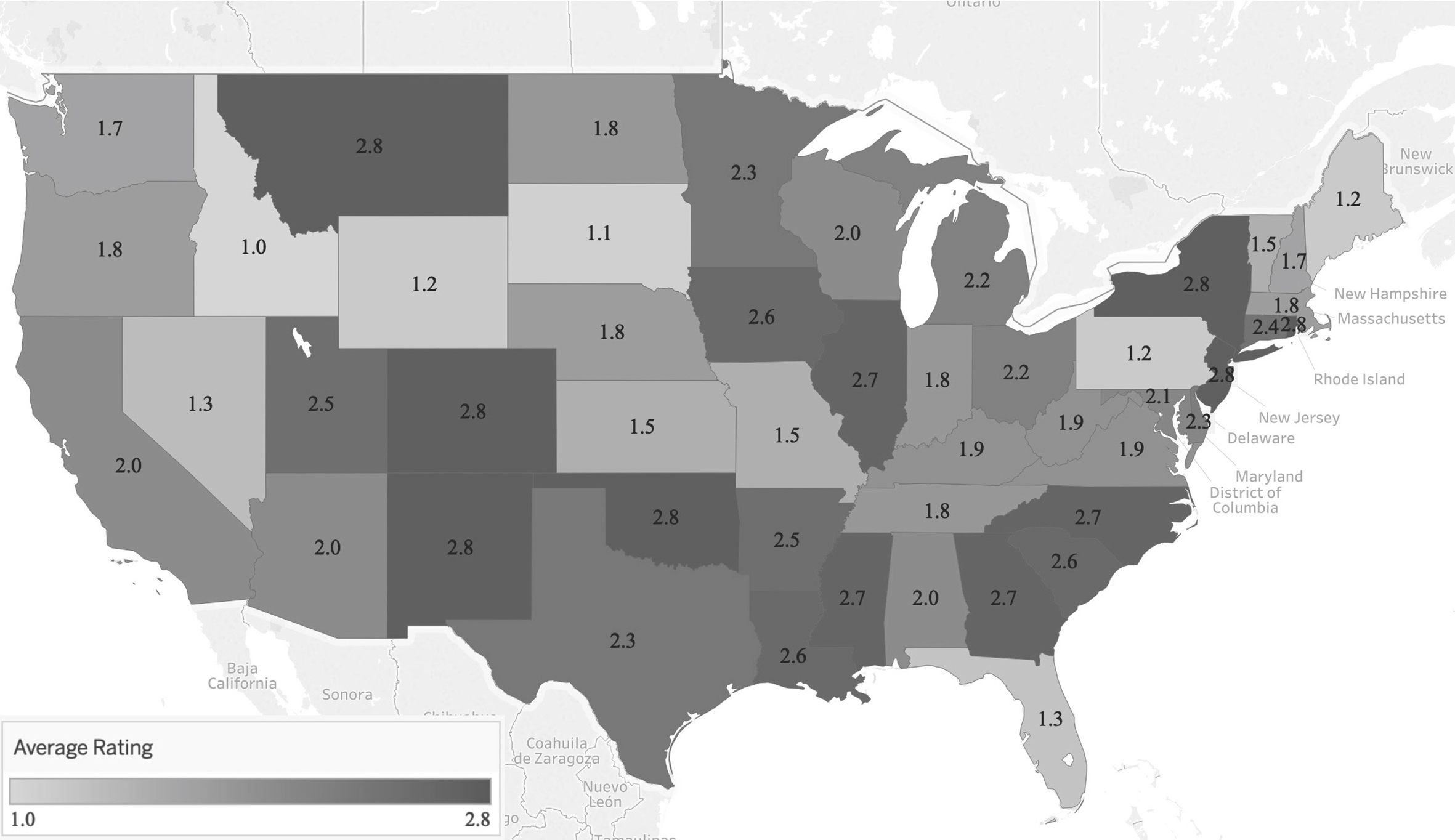
Average state rating for inclusion of 12 best practices for breastfeeding and beverages in regulations for childcare centers in 50 US states, July 2016. State regulations for childcare centers were evaluated for inclusion of 12 best practices for breastfeeding and beverages. Average ratings (1 = best practice not included, 2 = best practice partially included, 3 = best practice fully included) are presented for each state. Not pictured are Alaska (2.6) and Hawaii (2.5).
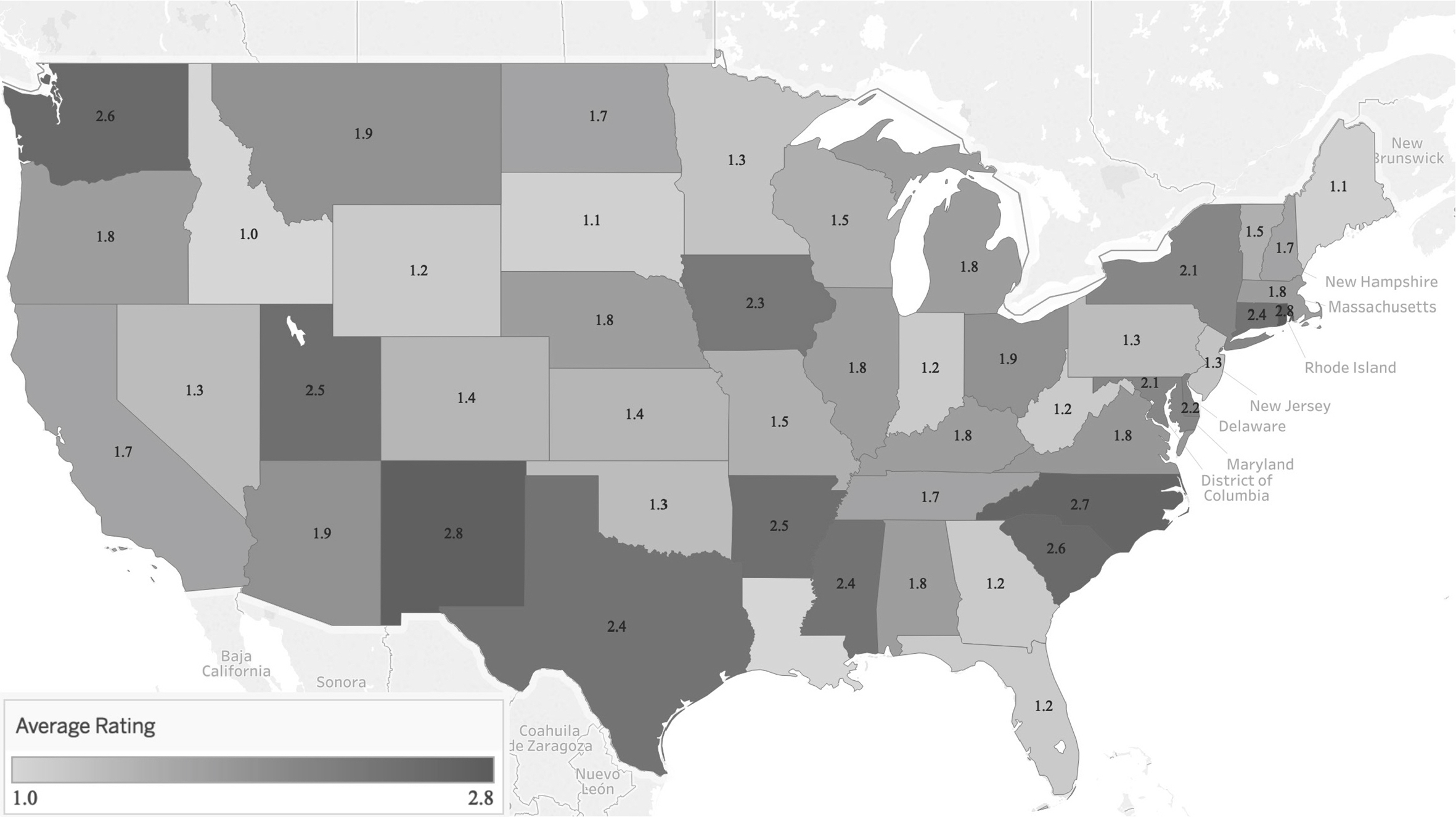
Average state rating for inclusion of 12 best practices for breastfeeding and beverages in regulations for family childcare homes in 49 US states, July 2016. State regulations for family childcare homes were evaluated for inclusion of 12 best practices for breastfeeding and beverages. Average ratings (1 = best practice not included, 2 = best practice partially included, 3 = best practice fully included) are presented for each state. Not pictured are Alaska (2.6) and Hawaii (2.5). Because there are no licensed homes in Louisiana, this state was excluded from analysis of homes.
Most states had higher (n = 26 states) or equal (n = 20 states) average ratings for centers than for homes, except for Pennsylvania, Texas, and Washington. Average ratings (SD) for all state regulations for centers vs homes had a higher average rating for inclusion of the 6 infant best practices (2.1 [0.5] vs 1.8 [0.5], t = 4.16, P < .001), 6 child best practices (2.1 [0.6] vs 1.8 [0.6], t = 3.27, P = .002), and 12 infant and child best practices combined (2.1 [0.5] vs 1.8 [0.6], t = 3.82, P < .001).
Discussion
Many breastfeeding and beverage best practices were not included or were only partially included in regulations in most states, suggesting substantial room for improvement. Infant best practices with low levels of inclusion by most states were for prohibiting infants from carrying or sleeping with a bottle, encouraging older infants to use a cup, not providing fruit juice to infants, and supporting breastfeeding. Several child best practices had low levels of inclusion by most states, including the best practice to avoid serving sugar-sweetened beverages. The best practice that drinking water be offered or served to children at meals and snacks had low levels of inclusion by most states, yet most states included the best practice that drinking water be made available to children throughout the day or in frequent intervals. Although many states included the best practice that only 100% juice be served to children, few states included limits to the volume of 100% juice served each day.
We also found substantial variation among states in the inclusion of breastfeeding and healthy beverage best practices in childcare regulations. Studies of childcare regulations had similar findings.8,15,16 In addition, in most states, centers included more breastfeeding and beverage best practices in childcare regulations than homes did. This finding is similar to the finding of a 2008 study that centers had more infant feeding regulations than homes did. 15 In addition, childcare regulations incorporated CACFP nutrition standards—and, thus, beverage best practices—in more than half of states for centers but for fewer than half of states for homes. This difference in inclusion of CACFP nutrition standards may contribute to the variation between regulations for centers and homes in overall inclusion of breastfeeding and beverage best practices.
Given the potential for population-level impact of strong organizational policies, 17 improvements in childcare breastfeeding and beverage policies could similarly have meaningful effects on children’s diets and body mass index. Studies suggest that childcare sites participating in CACFP reported offering more nutritious foods and healthier beverages than nonparticipating sites did.18-21 Similarly, studies in California suggest that the childcare beverage law that went into effect in 2012 resulted in an increase in healthier beverage offerings as reported by childcare sites.22-24
People in lower-income households are more likely to rely on homes than on centers, and the reverse is true for higher-income households. 25 In addition, the policies under which childcare settings operate should promote obesity-related health equity among young children. 26 Nutrition policy actions are found to be effective only when tailored to the socioeconomic and demographic characteristics of the settings they seek to support. 27 Studies suggest that cost may be a barrier to improving nutrition in childcare settings; however, policies that restrict serving unhealthy beverages may actually incur a cost saving for childcare sites.28,29 Given that many home providers live in low-income households themselves, and many face challenges in maintaining their personal well-being, 26 it is important that policies directed at homes are accompanied with adequate support in the form of technical assistance and training resources.
Limitations
This study had several limitations. First, our analysis did not measure implementation practices of existing regulations. Studies documenting childcare provider practices, whether observed or reported, suggest that provider practices are not fully consistent with policy requirements.22-24,30-32 Thus, future studies should evaluate the implementation of regulations, association with the actual beverage consumption of infants and children, and facilitators and barriers to implementation by childcare providers. Second, our study did not evaluate differences in best practices stratified by the size of the family childcare home (eg, small and large), so it may not accurately represent regulations for home providers. The evaluation of best practices for homes could be stratified according to the size of homes, as has been done for other childcare policy evaluations, 33 which could provide information on the type of technical assistance and training resources needed for homes. Third, the regulations in each state may have been modified since the original 2016 review; as such, they may not represent regulations in place at the time of this publication. Fourth, we applied a single code to centers or homes in each state based on the most predominant subcategory included by that state as a center or home; thus, it may not represent the policies for each of the various subcategories of that setting.
Conclusions
Inclusion of breastfeeding and beverage best practices in childcare regulations differs among states. In most states, best practices are incorporated in regulations for centers rather than for homes. States are encouraged to align childcare regulations to include best practices for breastfeeding and beverages and to standardize regulations between licensed childcare settings to ensure that breastfeeding is supported and healthy beverages are provided to all children, regardless of whether they are in a center or home.
Footnotes
Acknowledgments
The authors thank Erica Kenney and Rebecca Mozaffarian from the Harvard T.H. Chan School of Public Health and Sarah Gonzalez-Nahm and Elyse Grossman from the Johns Hopkins Bloomberg School of Public Health for their support with coding development and data collection; Lilly Nhan, Shelly Mandel, Kaela Plank, and Hannah Thompson from the University of California Nutrition Policy Institute for their data analysis guidance; and Paul Rogé from the University of California, Berkeley, for identifying funding for an undergraduate student researcher to support this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the National Heart, Lung, and Blood Institute of the National Institutes of Health under award no. R25HL125451 and the American Cultures Engaged Scholarship from the University of California, Berkeley. The Robert Wood Johnson Foundation Healthy Eating Research Program (grants 72062 and 73391) funded the initial data collection for this project.