
Abstract
Objectives
More than 16 000 graduate degrees in public health are awarded annually. Yet only 14% of the governmental public health workforce has formal public health training of any kind, and 8% has a master of public health (MPH) degree. We characterized the differences among governmental staff members with master’s degrees across US health departments.
Methods
We used data from the 2017 Public Health Workforce Interests and Needs Survey, a national survey of state and local public health departments (43 669 responses; response rate, 48%). We examined the characteristics of the workforce by educational attainment and compared respondents who had obtained a “terminal” (ie, highest degree obtained) MPH degree with respondents who had obtained a terminal non–public health (non-PH) master’s degree.
Results
Respondents who had a non-PH master’s degree were as likely as respondents who had an MPH degree to hold a supervisory role (43% vs 41%; P = .67). We found only 1 significant difference between the 2 groups: respondents aged ≤40 with a terminal MPH degree were significantly less likely than respondents aged ≤40 with a non-PH master’s degree to earn more than the national average salary (adjusted odds ratio = 0.67; 95% CI, 0.47-0.97; P = .03).
Conclusions
We found only marginal differences in career outcomes for people working in governmental public health who had a terminal MPH degree vs a terminal non-PH master’s degree. This finding does not necessitate a full reconsideration of the MPH as it relates to governmental public health practice but a greater recognition that there are multiple paths into practice.
A growing number of accredited schools and programs of public health are producing more graduates with public health degrees than ever before. As of 2019, there were 67 accredited schools of public health and 122 accredited programs, up from 20 schools in the early 1970s. 1 -3 Data from 2018 indicate that approximately 16 000 graduate degrees are conferred from accredited institutions in the United States each year, with as many as 3000 more from non–Council on Education for Public Health (CEPH)-accredited institutions. 2,4 The increase in availability of public health academic programs has not been met with a concomitant and equal rise in the education profile of the state and local public health workforce; recent studies indicate that most governmental employees do not have formal public health training. 5,6 The 2017 Public Health Workforce Interests and Needs Survey (PH WINS) indicated that only 14% had a public health degree at any level (ie, undergraduate, master’s, or doctoral) and only 8% had a master of public health (MPH) degree. 5 The 2016 National Profile of Local Health Departments (LHDs) survey from the National Association of County and City Health Officials (NACCHO) indicated that 25% of top executives at LHDs had a graduate degree in public health. 7 This percentage was up from 19% reported in 2005 8 but not significantly different from the earliest NACCHO profile in 1990, which reported that 23% of top executives at LHDs held a graduate degree in public health. 9 Like the NACCHO profile, the Association of State and Territorial Health Officials profile provides limited data on public health education for staff members; however, it does report the educational attainment of health department leadership. The proportion of state health officials who had an MPH degree increased from 33% in 2007, to 40% in 2012, to 44% in 2016. 10 -12
The decline in the movement of public health graduates into governmental public health agencies 2,13 and the modest levels of formal public health training among leaders in public health practice contribute to the “vicious cycle of disconnect between public health academia and practice.” 14 The Institute of Medicine’s landmark report in 1988, The Future of Public Health, 15 addressed this disconnect by recommending that schools of public health emphasize public health practice and match the educational program to the scope of public health practice. In response, Johns Hopkins University developed the Public Health Faculty/Agency Forum in 1990, which led to the Council on Linkages Between Academia and Public Health Practice, with a primary focus on competencies in public health practice. 16 Other training needs frameworks have emerged in recent years, including the strategic skills framework developed by the National Consortium for Public Health Workforce Development. 17
Another major set of training needs frameworks relates to formal public health education. CEPH, which predated the 1988 Institute of Medicine report, has regularly issued revised accreditation criteria, the emphasis of which has shifted to expected competencies of public health graduates. 18 Accreditation standards in the most recent revision (2016) are the culmination of work that began in 2011 through the Association of Schools and Programs of Public Health (ASPPH) as the Framing the Future initiatives to reimagine the academic preparation and degrees needed now and in the future. 19,20 Especially for an MPH degree, the revised accreditation standards focus on graduates’ achievement and demonstration of competencies required for the workforce. However, evidence is needed to determine whether this process results in a more effective partnership between academia and governmental public health practice than the previous standard and whether graduates are suitably trained for and can obtain positions in governmental public health agencies.
Despite efforts to redevelop the MPH degree in the 21st century, the low number of public health workers with an MPH degree begs the question: How do job outcomes differ in practice for people with an MPH degree vs another master’s degree? We used data from a large-scale workforce survey to characterize educational attainment of the governmental public health workforce, with a focus on people with a master’s degree. We examined differences between people with and without formal public health education and examined gaps in training and skills between the 2 groups.
Methods
Our analysis focused primarily on staff members at state health agencies (SHAs) and LHDs. We used data from PH WINS, a national survey of SHA and LHD staff members conducted in 2017; the survey is described elsewhere. 21 Briefly, the survey assessed perceptions of the workplace environment, job satisfaction, training needs related to job skills and abilities, and demographic characteristics of the public health workforce. The PH WINS sampling approach consisted of a complex design across 2 major frames. First, the survey conducted a census of participating SHAs and used balanced repeated replication weights to adjust for nonresponse and regional totals for SHA central office (SHA-CO) staff members. The local frame was more complex. Large health departments (members of the Big Cities Health Coalition, an association of the largest LHDs in the United States) 22 were sampled with certainty, as were LHDs located in nondecentralized states (where LHDs are operated by the SHA). 23 LHDs from decentralized states were sampled by US Department of Health and Human Services region and size (LHDs serving ≤250 000 people and LHDs serving >250 000 people). To be eligible for inclusion in PH WINS, LHDs had to have at least 25 staff members and serve at least 25 000 people. Balanced repeated replication weights were used to adjust for sampling design and nonresponse at the local level. The SHA-CO frame had 17 136 respondents (response rate, 35%), and the LHD frame had 26 533 respondents (response rate, 59%).
Our analytic approach consisted of descriptive and inferential analyses. First, we examined data on workforce characteristics by educational attainment, with a focus on respondents who had a master’s degree. We compared data on respondents who had obtained a “terminal” (ie, highest degree obtained) MPH degree with data on respondents who had obtained a terminal non–public health (non-PH) master’s degree. Then, we conducted bivariate comparisons of self-assessed importance and ability to perform tasks perceived as important for day-to-day work and workforce environment by educational attainment. We used design-adjusted Rao-Scott χ2 and Tukey tests for multiple comparisons to compare variables of interest based on educational attainment. Although only 14% of the workforce has a public health degree at any level, most public health department staff members who have any type of public health degree have an MPH. As such, respondents with a terminal MPH degree were the primary focus of the analyses.
Finally, to compare career-related outcomes among early-career and mid-career public health staff members, we conducted logistic regression examining the relative odds of an outcome among a set of 6 dependent variables for respondents aged ≤40, with the primary independent variable of interest being educational attainment (MPH vs non-PH master’s degree). The dependent variables of interest were whether respondents held a supervisory position or higher (public health managers and executives), whether their earnings were more than the national average, whether they were earning more than their state agency’s average, whether they were somewhat or very satisfied with their job, whether they were somewhat or very satisfied with their pay, and whether they were considering leaving their organization in the next year. We finalized models by using Akaike Information Criterion and stratified them by setting (SHA vs LHD). We managed and analyzed data by using Stata version 15.1 (StataCorp LP). The Centers for Disease Control and Prevention determined this study was not human subjects research. The NORC Institutional Review Board determined that PH WINS was exempt.
Results
Overall, 14% (95% CI, 12%-15%; weighted n = 24 795) of respondents working in governmental public health had a public health degree or a public health degree of any type. At the SHA-CO level, 19% had a public health degree (95% CI, 18%-20%; weighted n = 9942). At the LHD level, 12% (95% CI, 10%-14%; weighted n = 14 853) had a public health degree.
Approximately 4% (95% CI, 4%-5%; weighted n = 7745) had a bachelor’s degree in public health, 10% (95% CI, 9%-11%; weighted n = 17 670) had a master’s degree in public health (any type), and 1% (95% CI, 1%-2%; weighted n = 2482) had a doctoral degree in public health. A significantly higher percentage of men than women had a public health degree (16% vs 13%; P = .02). Attainment is moderated by setting (SHA-CO level: 19% vs 20% [P = .71]; LHD level: 15% vs 11% [P = .05]). An estimated 8% (95% CI, 7%-9%; weighted n = 14 034) of the workforce had an MPH degree; 12% (95% CI, 11%-13%; weighted n = 6278) at the SHA-CO level and 6% (95% CI, 5%-8%; weighted n = 7756) at the LHD level. Seven percent (95% CI, 6%-8%; weighted n = 12 084) had an MPH as their terminal degree. Respondents with a terminal MPH degree comprised half of all staff members with any type of public health degree. Approximately 17% (95% CI, 14%-21%; weighted n = 30 618) of the workforce had a terminal non-PH master’s degree. Among respondents with a non-PH master’s degree, 46% had a master of arts or master of science degree, 13% had a master of business administration (MBA) degree, 10% had a master of science in nursing (MSN) degree, 8% had a master of social work (MSW) degree, 7% had a master of public administration (MPA) degree, 1% had a master of public policy (MPP) degree, and 15% had another master’s degree.
About 79% (95% CI, 77%-81%; weighted n = 10 311) of respondents with a terminal MPH degree were women, and 76% (95% CI, 75%-77%; weighted n = 23 104) of respondents with a terminal non-PH master’s degree were women (P < .001) (Table 1). We found significant differences in the race/ethnicity of respondents who had an MPH degree vs a terminal non-PH master’s degree, specifically for Asian staff members. We also found significant differences in type of master’s degree by age. Nineteen percent (95% CI, 16%-22%; weighted n = 14 008) of respondents aged ≤40 had a terminal MPH degree, and 7% (95% CI, 6%-8%; weighted n = 9431) of respondents aged >40 had a terminal MPH degree (P < .001). Compared with respondents who had a non-PH master’s degree as their terminal degree, respondents who had an MPH degree as their terminal degree were approximately as likely to hold a supervisory role (43% vs 41%; P = .67). Respondents with a terminal MPH degree were less likely than respondents with a terminal non-PH master’s degree to indicate they were planning to retire by 2020 (12% vs 23%; P < .001). However, respondents with a terminal MPH degree were more likely than respondents with a terminal non-PH master’s degree to indicate they were considering leaving in the next year for reasons other than retirement, although this difference was not significant (34% vs 26%; P = .08). Among respondents working in the public health sciences, 16% had a terminal MPH degree and 21% had a non-PH terminal master’s degree (P < .001).
Demographic characteristics of state and local governmental public health staff members, United States, 2017
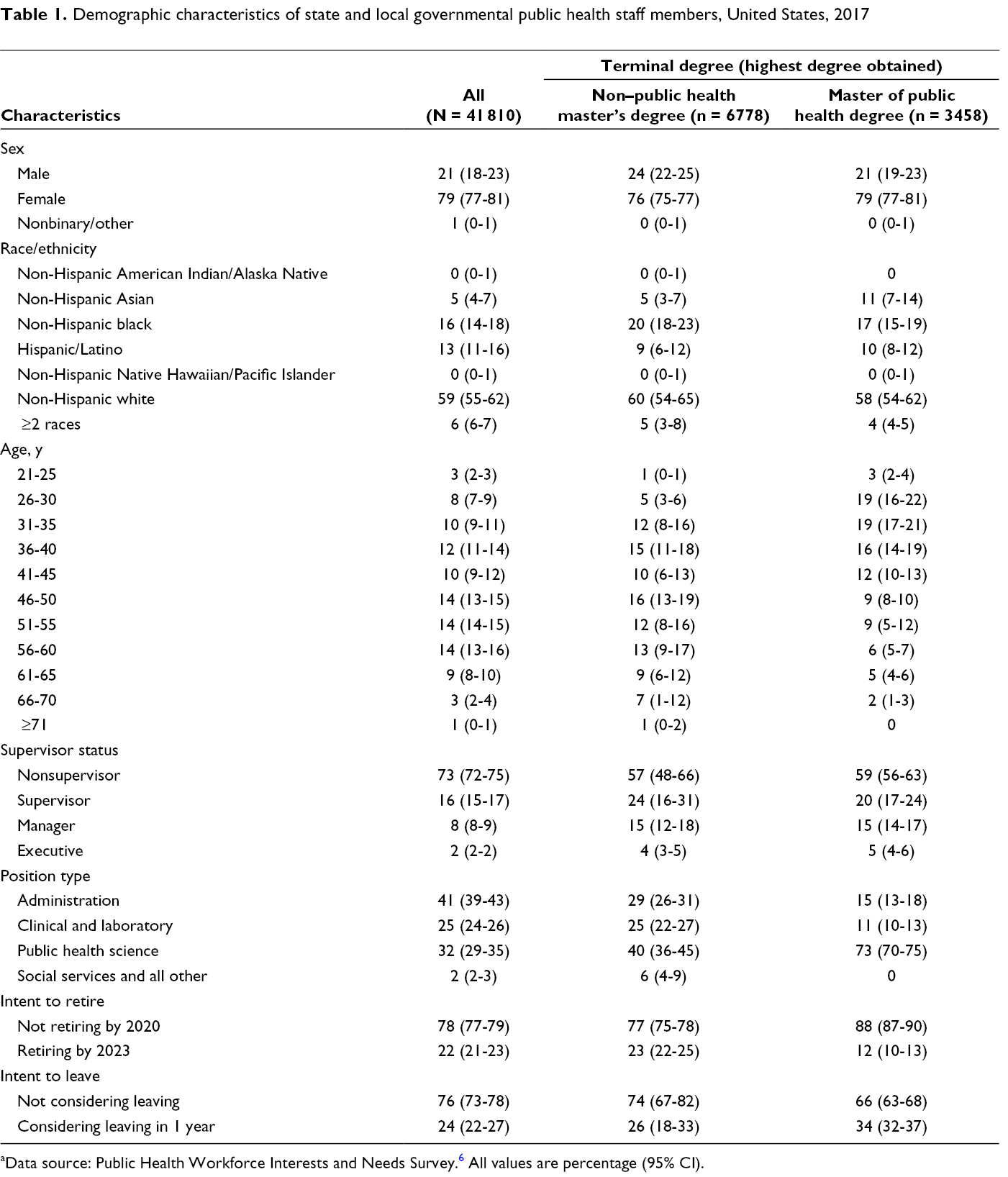
aData source: Public Health Workforce Interests and Needs Survey. 6 All values are percentage (95% CI).
Workplace Environment and Training Needs
We found differences in perceptions about workforce environment among respondents with terminal MPH degrees vs terminal non-PH master’s degrees (Table 2). Compared with respondents who had a non-PH master’s degree, respondents who had a terminal MPH degree were more likely to indicate that, within their organizations, creativity and innovation were rewarded (48% vs 44% [P = .01] for SHAs and 48% vs 45% [P = .20] for LHDs) and that supervisors or team leaders in their work unit support employee development (79% vs 72% [P = .002] for SHAs and 78% vs 77% [P = .77] for LHDs). Furthermore, at LHDs, respondents with a terminal MPH degree were more likely than respondents with a terminal non-PH master’s degree to indicate that they had a good relationship with their supervisor (87% vs 83% [P = .08] for SHAs and 85% vs 80% [P = .03] for LHDs). Respondents were asked multiple questions about their skills and abilities, which were collapsed into training needs by strategic skill domains (Table 3). For 5 of 8 domains for SHA-CO staff members, we found a significant difference in skill gaps between respondents who had a terminal MPH degree and respondents who had a terminal non-PH master’s degree: effective communication (15% vs 22%; P = .002), data for decision-making (26% vs 17%; P < .001), cultural competency (31% vs 36%; P < .001), budget and financial management (48% vs 57%; P < .001), and cross-sectoral partnerships (33% vs 29%; P = .01). For LHDs, the significant difference was in effective communication (11% vs 18%; P = .02). For LHDs, the only strategic skill for which respondents who had an MPH degree reported a smaller but significant skill gap than respondents who had a non-PH master’s degree was in using data for decision-making.
Perceptions of workplace environment, by setting and educational attainment, among people with master of public health (MPH) degrees and non–public health (non-PH) master’s degrees, United States, 2017 a
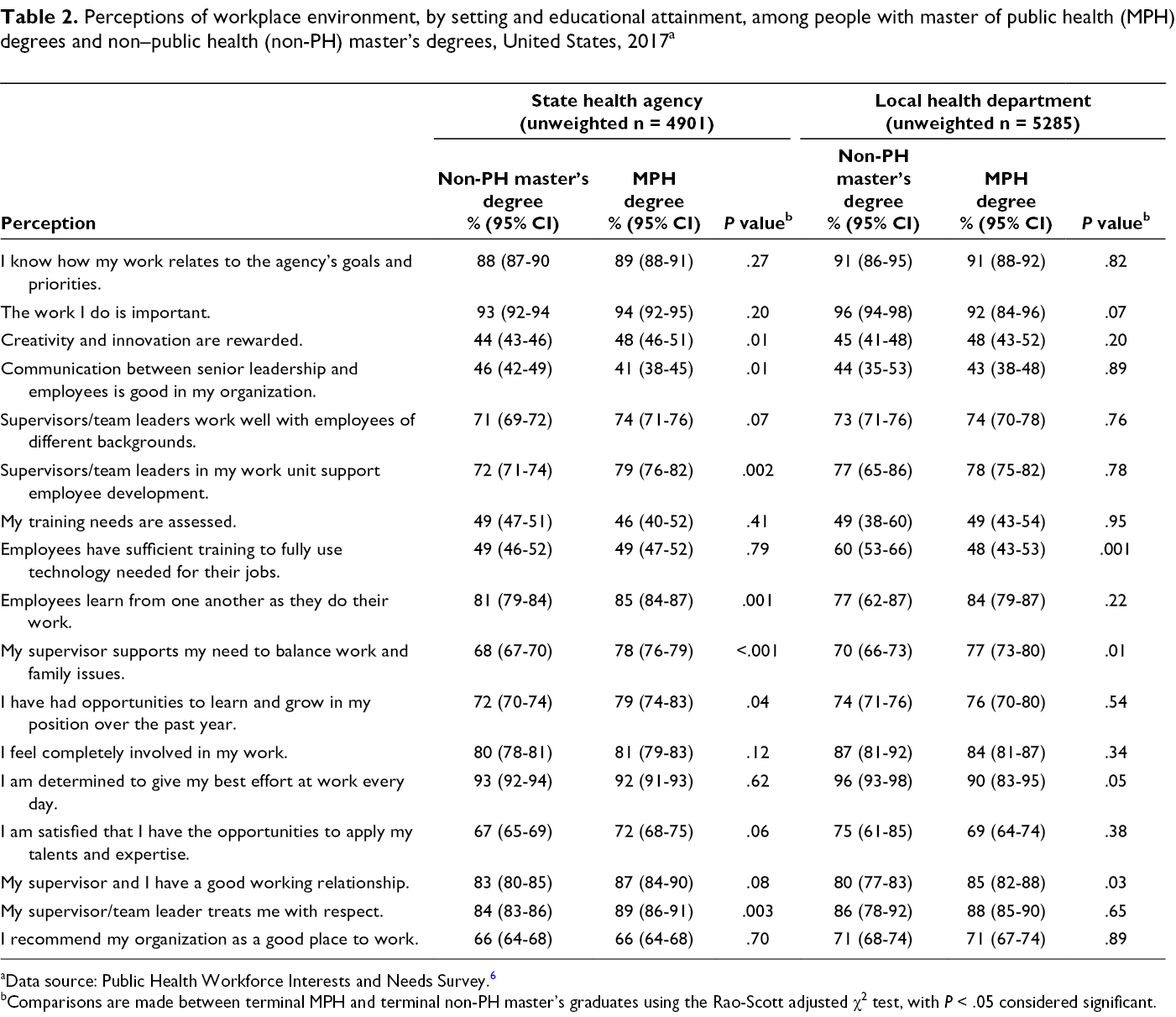
aData source: Public Health Workforce Interests and Needs Survey. 6
bComparisons are made between terminal MPH and terminal non-PH master’s graduates using the Rao-Scott adjusted χ2 test, with P < .05 considered significant.
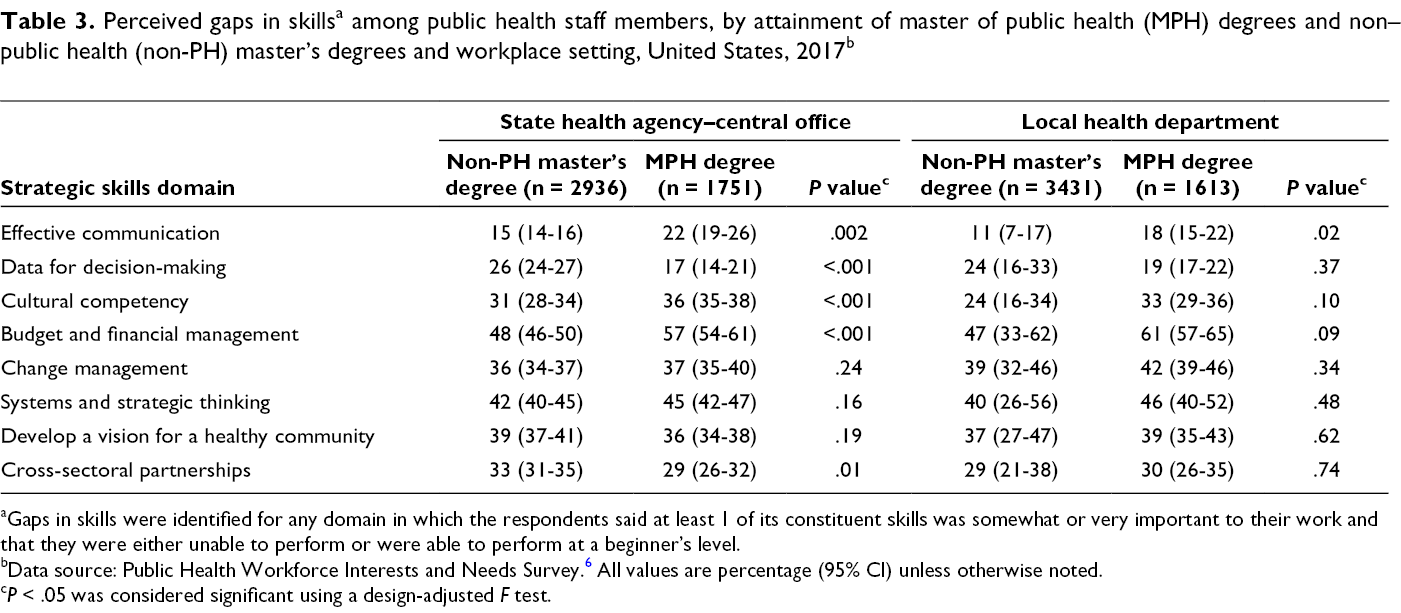
aGaps in skills were identified for any domain in which the respondents said at least 1 of its constituent skills was somewhat or very important to their work and that they were either unable to perform or were able to perform at a beginner’s level.
bData source: Public Health Workforce Interests and Needs Survey. 6 All values are percentage (95% CI) unless otherwise noted.
c P < .05 was considered significant using a design-adjusted F test.
Workplace Outcomes
We conducted a final set of analyses to assess the relative likelihood of career-related outcomes of interest (salary, supervisory status, and job and pay satisfaction) for staff members aged ≤40 (Table 4). Respondents aged ≤40 who had a terminal MPH degree were about as likely to be supervisors as their peers with a non-PH master’s degree. We found 1 significant difference between respondents who had a terminal non-PH master’s degree and respondents who had a terminal MPH degree: respondents aged ≤40 who had a terminal MPH degree were less likely to earn more than the national average salary than respondents aged ≤40 who had a terminal non-PH master’s degree (aOR = 0.67; 95% CI, 0.47-0.97; P = .03). We found no differences in job or pay satisfaction in either set of comparisons, except that staff members in LHDs who had a terminal MPH degree were more likely than staff members in LHDs who had a terminal non-PH master’s degree to be considering leaving their job in the next year (aOR = 2.8; 95% CI, 1.4-5.4; P = .01).
Career-related outcomes among public health staff members aged ≤40 with a terminal master of public health degree or a terminal non–public health master’s degree, United States, 2017 a
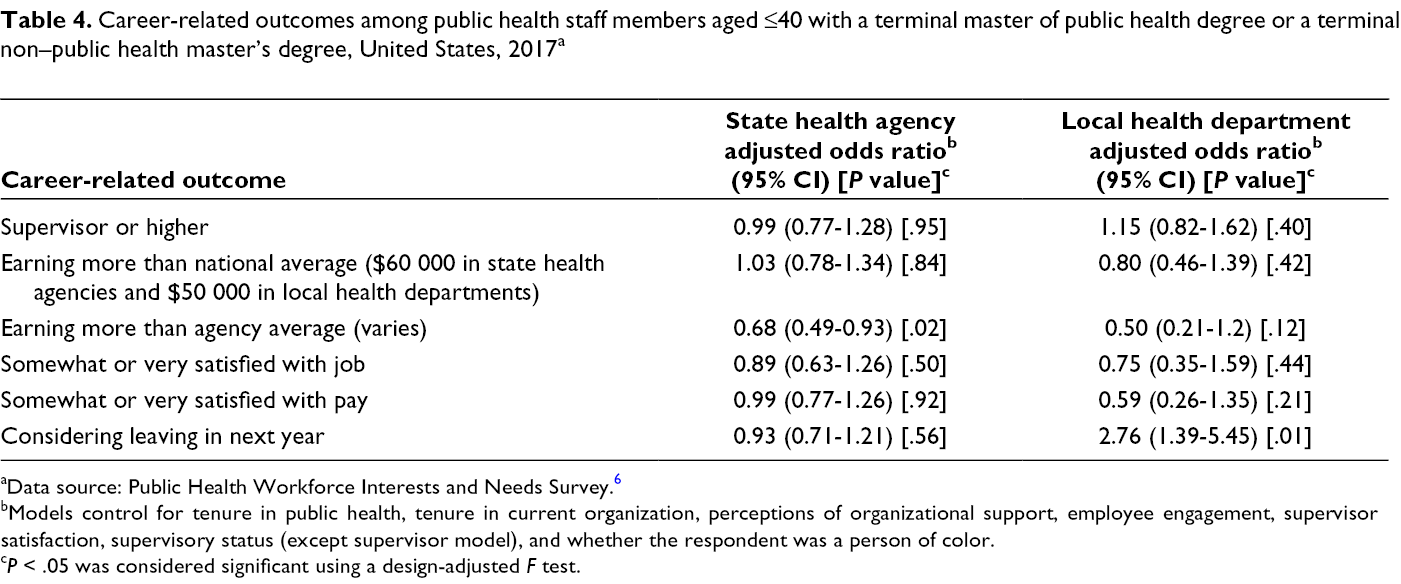
aData source: Public Health Workforce Interests and Needs Survey. 6
bModels control for tenure in public health, tenure in current organization, perceptions of organizational support, employee engagement, supervisor satisfaction, supervisory status (except supervisor model), and whether the respondent was a person of color.
c P < .05 was considered significant using a design-adjusted F test.
Discussion
Health department workforce development has long focused on recruiting people who have formal graduate training in public health. As a field, public health has targeted efforts with ASPPH members to improve competencies and strengthen associations between academia and governmental public health. However, evidence indicates that fewer than one-fifth of new graduates from ASPPH-member schools are opting for public sector jobs; longitudinal data from 1 school found that fewer graduates were opting for public sector jobs over time. 24,25 Although ASPPH-member schools have long been regarded as a primary entry point for the governmental public health workforce, in practice this may be true only for careers in public health science (eg, epidemiology, data analysis, health education, and related topics). However, our study found few practical differences between government employees with a terminal MPH degree and government employees with a terminal non-PH master’s degree, suggesting that a broader recruitment strategy inclusive of non-PH master’s degree programs may be necessary to make substantial gains in the employment of graduate-level trained public health practitioners.
Our study indicates that people who have a graduate degree in public health are likely to work in public health science, whereas people who have a non-PH master’s degree tend to work in administration and clinical and laboratory services. It is crucial to continue to recruit and retain public health graduates to maintain the core science of public health practice. However, in other positions, a more balanced approach that broadens recruitment from master’s degree programs outside of public health is prudent. People with a non-PH master’s degree bring skills in areas such as budget and finance (MBA), clinical services (MSN), and administration (MPP or MHA), which help optimize performance of governmental public health agencies. Although in our study, respondents with a non-PH master’s degree were less likely than respondents with an MPH degree to leave their positions in the next year, they were older than their MPH counterparts. Data from this study indicate that 3 in 5 workers with a non-PH master’s degree were aged >45, compared with 1 in 3 workers with an MPH degree.
Given the different education objectives of different degrees, it is not surprising that workers with an MPH degree and workers with a non-PH master’s degree identify different training needs. National training strategies should recognize the need for different trainings and prioritize new trainings to fill public health science gaps for people without formal public health training and management and related gaps for people without public policy or business training. Governmental public health agencies can leverage the strengths of their existing workforce to strengthen the entire workforce.
Limitations
This study had several limitations. First, PH WINS data are self-reported. As such, items in this analysis are largely related to perception and intent to leave, which are reasonably measured through self-report. Second, although PH WINS data are nationally representative of SHA-CO staff members and staff members at mid- and large-sized LHDs, staff members at small LHDs (ie, LHDs serving <25 000 people or LHDs that have <25 staff members) are not included. As such, PH WINS is not representative of staff members from small LHDs. However, analysis from available data on small LHDs shows that about 10% of these staff members have a terminal public health master’s degree (almost all MPH degrees). 26 As such, our findings are expected to be broadly generalizable to the state and local governmental public health workforce.
Conclusion
The genesis of education in public health has historically been at the master’s-degree level, although the number of undergraduate public health degrees awarded annually may soon eclipse the number of MPH degrees awarded. 2,3 Since the Welch–Rose report a century ago, 27 focus on the core sciences, as well as advancement in leadership capacity, has been a foundational recommendation for master’s degree students in the field of public health. In the early 2000s, the modern notion of public health education was formalized in the landmark Institute of Medicine report that laid out workforce development concerns for the 2 decades that would follow. 14 However, analysis of governmental public health workforce data has shown that a small percentage of the workforce has formal training in public health and that there are only marginal differences in career outcomes for people who have a terminal MPH degree compared with people who have other types of non-PH master’s degrees. People with terminal MPH degrees are more likely than people with non-PH master’s degrees to work in the public health sciences in a health department, but their earnings and advancement appear only marginally different. This observation does not necessitate a full reconsideration of the MPH degree as it relates to governmental public health practice, but a greater recognition that there are multiple paths into practice. This observation also suggests a need to continue support for robust on-the-job training and broader workforce development to ensure the workforce is ready for the challenges of the future.
Our findings also have implications for academic institutions, which could encourage further cross-disciplinary curriculum development and interprofessional education during degree programs. Although many dual-degree programs exist (eg, MBA-MPH, MSN-MPH), the extent to which a singular non-PH master’s degree program requires 1 or more public health courses, and vice versa, is not known. Given the multiple graduate-level pathways to employment in governmental public health, such connectivity during degree attainment could enhance workforce development efforts.
Footnotes
Acknowledgments
The authors thank Fatima Coronado, MD, MPH, and Sanjana Srinivasan, MPH, for their assistance on this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PH WINS was a joint effort of the Association of State and Territorial Health Officials and the de Beaumont Foundation. The de Beaumont Foundation funded the project. J.P.L. was funded by the de Beaumont Foundation for his time on this project.