
Abstract
Objectives
Correctional settings (prisons, jails, detention facilities) provide a unique opportunity to screen for sexually transmitted infections (STIs) among correctional populations with a high prevalence of infection. Immigrant detainees are a distinct and poorly described correctional population. The main objective of this study was to determine the feasibility of a national STI screening program for immigrant detainees.
Methods and Materials
We developed an opt-out STI testing program that included electronic health record integration, patient education, and staff member training. We piloted this program from June 22 through August 19, 2018, at 2 detention facilities with different operational requirements and detainee demographic characteristics. We assessed STI test positivity rates, treatment outcomes, estimated cost to conduct testing and counseling, and staff member perceptions of program value and challenges to implementation.
Results
Of 1041 immigrant detainees approached for testing, 526 (50.5%) declined. Of 494 detainees who were tested, 42 (8.5%) tested positive for at least 1 STI; the percentage positivity rates were 6.7% (n = 33) for chlamydia, 0.8% (n = 4) for syphilis, 0.8% (n = 4) for gonorrhea, 0.6% (n = 3) for hepatitis B, and 0.2% (n = 1) for HIV. The estimated cost to detect any STI ranged from $500 to $961; the estimated cost to identify 1 person infected with HIV ranged from $22 497 to $43 244. Forty of 42 persons who tested positive began treatment before release from custody. Medical staff members had positive views of the program but had concerns about workload.
Practice Implications
STIs are prevalent among immigrant detainees. A routine screening program is feasible if operational aspects are carefully considered and would provide counseling, education, and treatment for this vulnerable population.
Sexually transmitted infection (STI) screening programs in US correctional settings (eg, prisons, jails, detention facilities) provide an important opportunity to treat persons at high risk of being infected, 1,2 yet who may otherwise lack the resources to seek and/or obtain testing and appropriate management. 3,4 Reducing the prevalence of STIs among correctional populations benefits neighboring US communities by decreasing transmission among contacts and unborn children. 5 Rates of STIs among persons in US correctional settings are substantially higher than rates of STIs among the general public. 1 Immigrant detention is a unique setting that combines mobility, short stay, and diverse citizenship. Diagnosing and treating STIs in an immigration detention setting has the potential to reduce community transmission, both in the United States and abroad. However, STI test positivity rates and screening program assessment among Immigration and Customs Enforcement (ICE) detainees has not previously been described.
STI testing of correctional populations is supported by the Centers for Disease Control and Prevention guidelines. 6 The Centers for Disease Control and Prevention and the National Commission on Correctional Health Care recommend screening for HIV via an opt-out testing strategy in correctional settings 7,8 to reduce the stigma of being infected with an STI, thereby increasing testing program participation. 9 Universal STI screening has never been applied to a US immigration detention setting; its acceptability, which relies on factors such as health literacy and trust in the custody health care setting, 10 remains in question.
The 2011 ICE Performance-Based National Detention Standards 11 provide guidance on the minimum medical standards that facilities housing ICE detainees must meet, but it does not mandate STI testing. We explored the feasibility of implementing an opt-out STI screening program to inform future Performance-Based National Detention Standards guidance and practices in a subset of detention facilities in which we have direct visibility over patient care (ICE Health Service Corps [IHSC]–staffed facilities).
Materials and Methods
IHSC formed a multifacility, multidisciplinary workgroup to design an optimal opt-out STI screening pilot program that included electronic health record integration, patient education (pre- and posttesting), and staff member training. Tests conducted were HIV 1/2 fourth-generation assay (antigen and antibody), hepatitis B surface antigen test, rapid plasma reagin with reflex to Treponema pallidum antibodies, and nucleic acid testing (urine) for Neisseria gonorrhea and Chlamydia trachomatis.
We piloted this program at 2 IHSC-staffed detention facilities from June 22 through August 19, 2018. These facilities differed in their characteristics (eg, daily population, facility contract [ie, owned by private corporations or by ICE]) and detainee demographic characteristics. Facility A was located in Arizona, housed only male detainees, had an average daily population of 650 persons, and had an average length of stay of 37 days during fiscal year 2018. Facility B was located in Texas, housed both male and female detainees, had an average daily population of 1750 persons, and had an average length of stay of 32 days during fiscal year 2018. Participating facilities selected the optimal time to perform the screening visit. Given the restrictions in medical waiting room space, detainee turnover, and competing needs for clinic space, facility A elected to do the screening visit at day 30 of detention. Facility B combined the screening visit with the initial health assessment (the full physical examination generally performed within the first 7 days of detention at this facility).
At the initial appointment, health staff members provided detainees with pretesting counseling and education on STIs in their first language. They also detailed the tests that would be performed (unless detainees chose not to participate) and the potential health outcomes that would result from untreated infections. They further explained that participation was voluntary, testing and treatment were free, test results did not affect custody status, and all results would be confidential. We excluded detainees from the pilot program if they were symptomatic or pregnant (and therefore offered testing and treatment as part of clinical care before the program’s implementation); were known to be infected with any STIs, including HIV; or entered a facility on a day when screening was not available because of inadequate staffing. If a detainee was released from and reentered either of the 2 facilities during the pilot study, we included only the detainee’s first opt-out encounter.
We collected data on demographic characteristics, medical history, laboratory test results, and treatment provided via electronic health record review and entered in an Epi Info 12 collection form. Demographic variables were detainee gender (male, female, gender nonconforming), age (continuous), country of citizenship (El Salvador, Guatemala, Honduras, Mexico, other [ie, all other countries worldwide from which ICE has detainees]), and detention facility (facility A or facility B). Medical history variables were history of physical and/or sexual abuse (lifetime: any vs none), history of substance use (any vs none), behavioral health diagnoses (any vs none), and chronic medical diagnoses (eg, diabetes, hypertension, asthma, hypothyroidism, hyperlipidemia, and seizure disorder: any vs none). We conducted our analysis by comparing descriptive characteristics between our screened cohort and all detainees in IHSC-staffed facilities using simple logistic regression, as well as by examining bivariate associations, using logistic regression, between each covariate and STI results. We conducted all statistical analyses using SAS version 9.4. 13
We calculated the cost in 2018 dollars per patient screened and per diagnosis by using the average time to complete all encounter types and related procedures, laboratory specimen collection, average hourly billing rates for various disciplines (licensed vocational nurse, registered nurse, advanced practice provider, physician), and laboratory fees (for tests performed by the same contract laboratory and ordered under a single test code); we did not include the cost to treat a patient once an infection was confirmed or the opportunity cost (resources that could have been allotted to some other program). We presented cost per encounter by a range based on the various discipline types (eg, physician, advanced practice provider, registered nurse) eligible to conduct the encounter or procedure.
We surveyed staff members about their impressions of project challenges and successes, electronic health record encounter templates, training and preparation, and impact on general operations by using an online electronic survey consisting of 10 semiquantitative and open-ended questions.
This study was deemed nonresearch by the IHSC internal review process.
Results
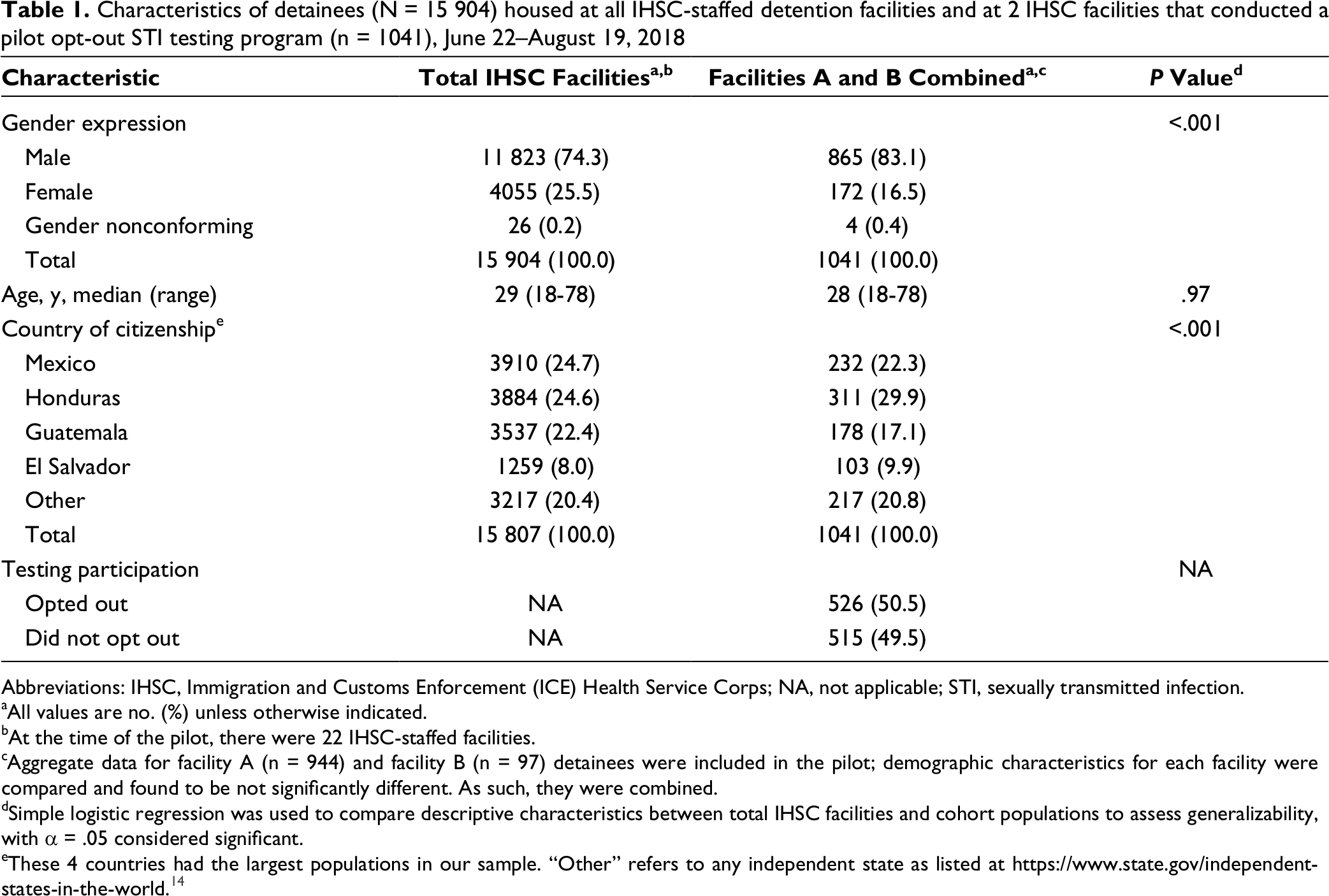
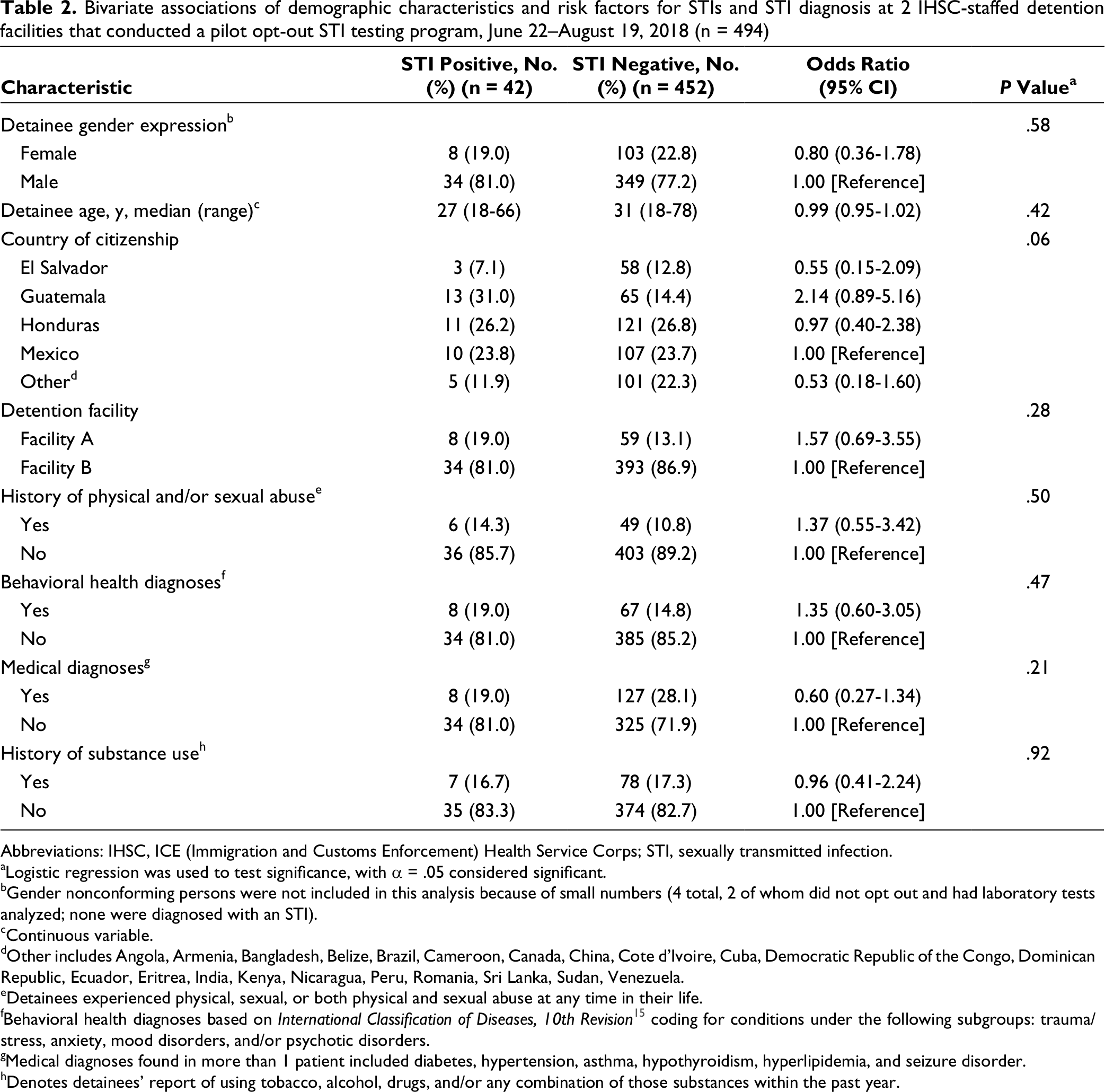
Staff members at the 2 pilot sites approached 1041 detainees (865 men, 172 women, 4 gender nonconforming) with a median age of 28 years; 526 (50.5%) opted out of STI testing (Table 1). We found no substantial differences in demographic characteristics between facility A and facility B; as such, the data are presented in aggregate. Facility A had a lower rate of opting out (27%) than facility B (53%). We collected laboratory specimens from 494 of the 515 detainees who did not opt out of STI testing. The 21 detainees who consented to testing but did not have specimens collected had either transferred from the facility (n = 6) before the testing appointment or declined testing at the time of the appointment (n = 15). Overall, of 497 detainees who were tested for STIs, 42 (8.5%) tested positive for any STI, 3 of whom tested positive for >1 STI. Thirty-three (6.7%) detainees tested positive for chlamydia, 4 (0.8%) for syphilis, 4 (0.8%) for gonorrhea, 3 (0.6%) for hepatitis B, and 1 (0.2%) for HIV. We considered all infections as newly diagnosed because no detainees had reported previous diagnosis or treatment. Forty of 42 (95.2%) detainees with STIs were treated before being released from custody. We found no substantial differences in demographic or risk factor variables between facility A and facility B and no significant bivariate association between these variables and having an STI diagnosed (Table 2). Gender nonconforming persons were not included in this analysis because of small numbers (4 total, 2 of whom did not opt out and had laboratory tests analyzed; none were diagnosed with an STI).
Characteristics of detainees (N = 15 904) housed at all IHSC-staffed detention facilities and at 2 IHSC facilities that conducted a pilot opt-out STI testing program (n = 1041), June 22–August 19, 2018
Abbreviations: IHSC, Immigration and Customs Enforcement (ICE) Health Service Corps; NA, not applicable; STI, sexually transmitted infection.
aAll values are no. (%) unless otherwise indicated.
bAt the time of the pilot, there were 22 IHSC-staffed facilities.
cAggregate data for facility A (n = 944) and facility B (n = 97) detainees were included in the pilot; demographic characteristics for each facility were compared and found to be not significantly different. As such, they were combined.
dSimple logistic regression was used to compare descriptive characteristics between total IHSC facilities and cohort populations to assess generalizability, with α = .05 considered significant.
eThese 4 countries had the largest populations in our sample. “Other” refers to any independent state as listed at https://www.state.gov/independent-states-in-the-world. 14
Bivariate associations of demographic characteristics and risk factors for STIs and STI diagnosis at 2 IHSC-staffed detention facilities that conducted a pilot opt-out STI testing program, June 22–August 19, 2018 (n = 494)
Abbreviations: IHSC, ICE (Immigration and Customs Enforcement) Health Service Corps; STI, sexually transmitted infection.
aLogistic regression was used to test significance, with α = .05 considered significant.
bGender nonconforming persons were not included in this analysis because of small numbers (4 total, 2 of whom did not opt out and had laboratory tests analyzed; none were diagnosed with an STI).
cContinuous variable.
dOther includes Angola, Armenia, Bangladesh, Belize, Brazil, Cameroon, Canada, China, Cote d’Ivoire, Cuba, Democratic Republic of the Congo, Dominican Republic, Ecuador, Eritrea, India, Kenya, Nicaragua, Peru, Romania, Sri Lanka, Sudan, Venezuela.
eDetainees experienced physical, sexual, or both physical and sexual abuse at any time in their life.
fBehavioral health diagnoses based on International Classification of Diseases, 10th Revision 15 coding for conditions under the following subgroups: trauma/stress, anxiety, mood disorders, and/or psychotic disorders.
gMedical diagnoses found in more than 1 patient included diabetes, hypertension, asthma, hypothyroidism, hyperlipidemia, and seizure disorder.
hDenotes detainees’ report of using tobacco, alcohol, drugs, and/or any combination of those substances within the past year.
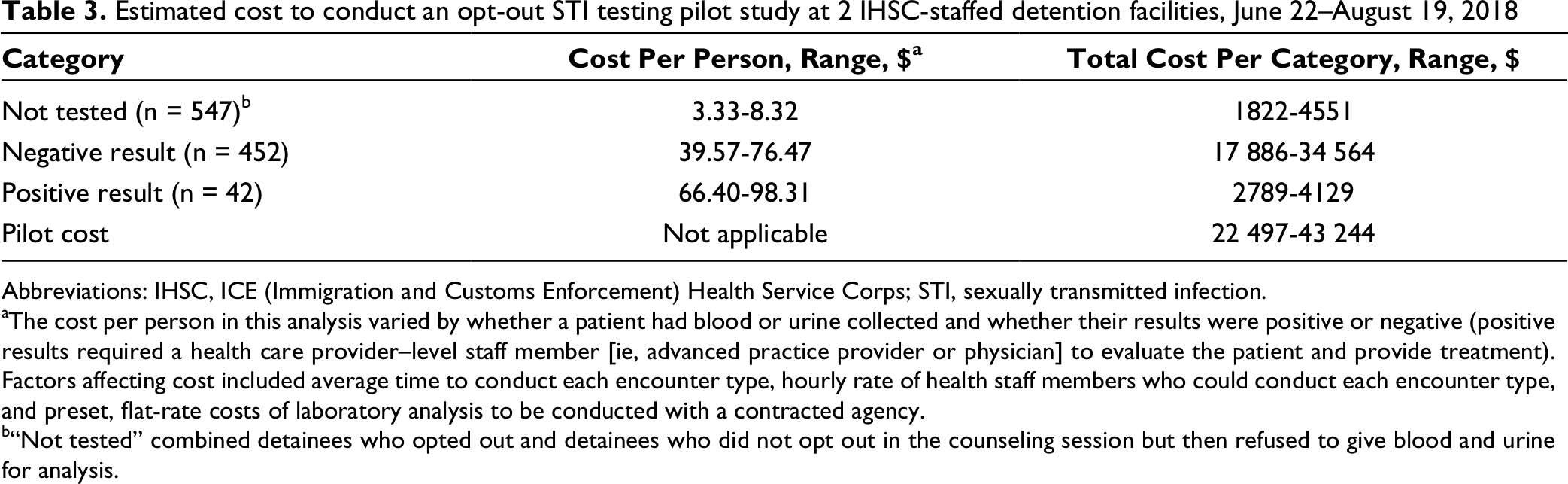
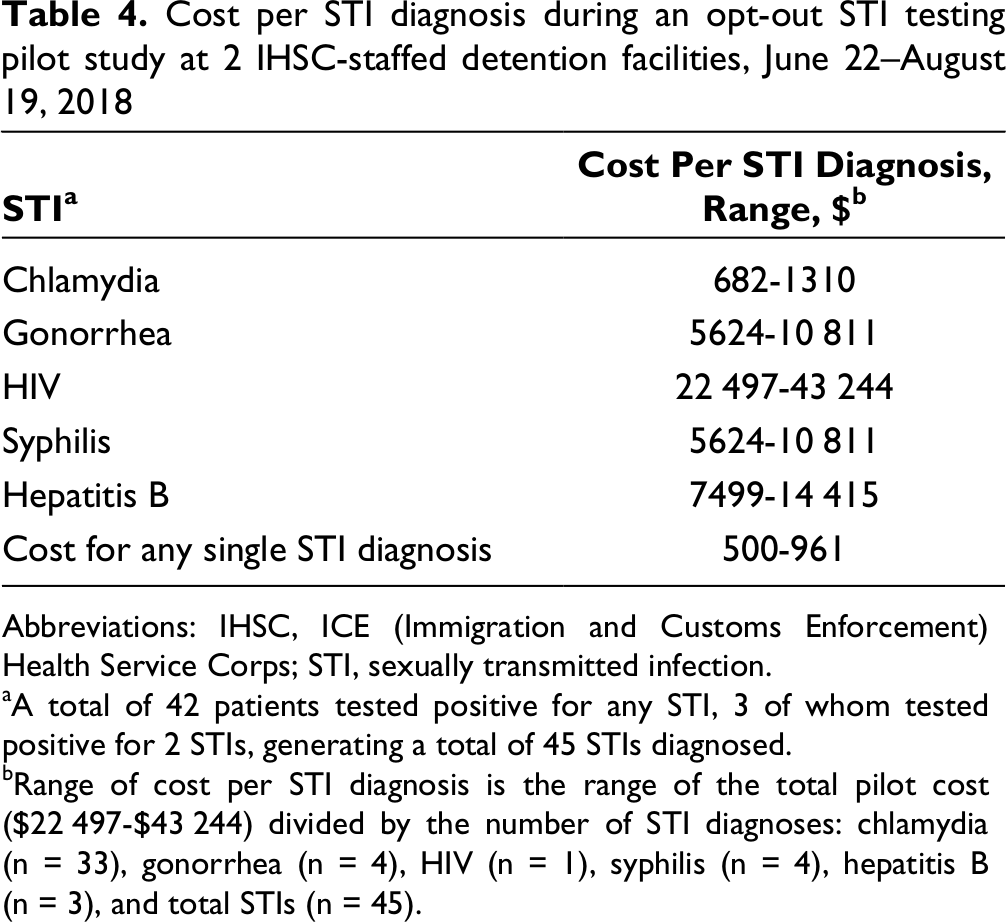
We analyzed costs for the initial opt-out STI counseling appointment (ie, staff member time), sample collection and offsite analysis by a commercial laboratory, and appointments (ie, staff member time) to review negative or positive STI results (Table 3). When including average encounter times, labor costs, and laboratory costs ($43.00/patient), the cost of our pilot program ranged from $22 497 to $43 244, with a per-patient average cost ranging from $22 to $42. We also estimated the cost to detect any STI, which ranged from $500 to $961; diagnosing a single case of HIV cost >$22 000 (Table 4).
Estimated cost to conduct an opt-out STI testing pilot study at 2 IHSC-staffed detention facilities, June 22–August 19, 2018
Abbreviations: IHSC, ICE (Immigration and Customs Enforcement) Health Service Corps; STI, sexually transmitted infection.
aThe cost per person in this analysis varied by whether a patient had blood or urine collected and whether their results were positive or negative (positive results required a health care provider–level staff member [ie, advanced practice provider or physician] to evaluate the patient and provide treatment). Factors affecting cost included average time to conduct each encounter type, hourly rate of health staff members who could conduct each encounter type, and preset, flat-rate costs of laboratory analysis to be conducted with a contracted agency.
b“Not tested” combined detainees who opted out and detainees who did not opt out in the counseling session but then refused to give blood and urine for analysis.
Cost per STI diagnosis during an opt-out STI testing pilot study at 2 IHSC-staffed detention facilities, June 22–August 19, 2018
Abbreviations: IHSC, ICE (Immigration and Customs Enforcement) Health Service Corps; STI, sexually transmitted infection.
aA total of 42 patients tested positive for any STI, 3 of whom tested positive for 2 STIs, generating a total of 45 STIs diagnosed.
bRange of cost per STI diagnosis is the range of the total pilot cost ($22 497-$43 244) divided by the number of STI diagnoses: chlamydia (n = 33), gonorrhea (n = 4), HIV (n = 1), syphilis (n = 4), hepatitis B (n = 3), and total STIs (n = 45).
Of 118 health staff members involved at any stage in the process, 24 (20.3%) completed an online survey on the overall design, processes, and outcomes of the pilot program. Of those who completed the survey, 15 (62.5%) reported that the electronic health record tools (note templates and laboratory order sets) were efficient, and 22 (91.7%) were satisfied with the program protocols and trainings provided. Staff members reported generally positive views of the program but expressed concern about workload and a need for more staffing if the program were implemented on a larger, more permanent scale.
Discussion
STI screening in nonimmigrant correctional settings has proven effective for reaching persons who have an increased risk for acquiring an STI but have decreased access to routine health care outside the correctional settings. 16,17 Immigrants who enter the United States through legal routes undergo some STI screening (syphilis and gonorrhea) 18 and are treated through panel physicians and their collaborating health departments. Although our population’s test positivity rates are lower than in other correctional settings in the United States, 16,19 our data suggest that implementing a comprehensive STI screening program for immigrant detainees, preferably opt-out testing, is likely to result in the identification of thousands of STIs annually and the opportunity to treat or initiate treatment of most detainees who are diagnosed with an STI. Approximately 1 in 12 detainees who underwent testing were found to have at least 1 asymptomatic STI; failure to identify and treat these persons is a missed opportunity to improve their health and to protect others residing in their postrelease community (in the United States or abroad).
Limiting testing to persons with clinical indications (symptoms of and/or risk factors for STIs) in an immigrant detention setting will fail to identify many persons who are infected, because of the asymptomatic nature of these infections. 20 From January 2014 through June 2018, we determined that 0.1% of detainees were diagnosed with syphilis through routine clinical practice and agency clinical guidelines (unpublished data, IHSC); during our pilot study, nearly 1% of incoming detainees were diagnosed with latent syphilis of unknown duration, which suggests that efforts made at immigrant detention facilities are missing most syphilis patients who could be successfully identified and treated. This finding has substantial public health implications in preventing syphilis transmission and complications in the United States and abroad.
Chlamydia, gonorrhea, and syphilis—STIs that can be cured by an antibiotic regimen (most with a single dose)—comprised most (91%) of the STIs we identified. Given the brief time detainees remain in our medical system (average detention stay in fiscal year 2018 for IHSC-staffed facilities ranged from 11 to 61 days), these STIs are ideal for successful identification and treatment. We initiated treatment of chronic infections (ie, HIV, hepatitis B) during custody, but continued treatment requires community investment in resources, whether a patient remains in the United States or repatriates. We treated 95% of persons before release from custody, which speaks to the feasibility of this program, as demonstrated by others in short-stay custody populations. 21 Close coordination with local health departments is necessary to ensure that detainees released in the United States before treatment are linked to care. Detainees who repatriate before treatment pose a challenge for linkage to care; fortunately, this outcome occurred in only 2 of the 42 patients. Therefore, we would expect release before treatment to occur infrequently during any future implementation.
This small pilot study did not uncover any risk factors associated with being diagnosed as having an STI, but this finding was limited by the available health record data and the unadjusted bivariate analysis. Therefore, a more inclusive testing approach, such as an opt-out method, is merited. In addition, most detainees did not report sexual abuse or sexual assault (92%) or tobacco use and/or drug or alcohol use (87%) in their initial health assessment. Therefore, we do not recommend using a risk-based strategy for screening but rather the most inclusive strategy feasible.
Of detainees approached, half opted out of STI testing, which is higher than the opt-out rate in studies of other correctional populations. 9,22,23 The opt-out rate differed significantly between facility A (27%) and facility B (53%). We postulate that this difference was because of the timing of the screening encounter; detainees who were at the facility longer (30 days at facility A vs ≤14 days at facility B) may have established rapport, gained trust in the health staff members, and been more certain that their remaining time in custody would allow for receipt of results and treatment. Further analysis is warranted to explore potential barriers of testing acceptance, including language and gender discordance, previous detention, STI knowledge, previous STIs, and the effect on testing acceptance, if any, of staff member discipline during the initial counseling visit (eg, nurse vs health care provider). Although not collected systematically, anecdotal reasons for opting out included denial of symptoms and/or risk factors and impending release.
This pilot study found that to diagnose a detainee with any STI would cost $500 to $961. Because detention stays are generally short, our ability to assess cost savings from complications averted as a function of early disease detection and management is limited. However, many other STI screening programs, especially those focusing on chlamydia, have been touted as cost effective. 21,24,25 Staff members’ time comprised 51% to 56% of our calculated cost, a portion attributed to pre- and posttesting counseling. We felt it was important to invest these resources to maximize participation in the program and to ensure detainees had sufficient information to make informed choices. Concerns about the ethics of mass screening have been voiced by other researchers, 26 and we felt compelled to provide clear, concise information to each detainee about the purpose of the testing, treatment, and confidentiality.
Given the heterogeneity and dynamic nature of our immigrant detention population, additional, more comprehensive assessment of this proposed program is needed. In the meantime, IHSC is committed to gradually expanding routine STI screening. As a result of this pilot study, presented to IHSC leadership as an executive summary (unpublished IHSC internal document), STI screening has been added to agency annual planning and budget; IHSC leadership has approved expansion of this screening program to sites with adequate staffing and an infection preventionist to act as the local champion and trainer (ie, 13% of current facilities, with a planned increase to at least 50% by fiscal year 2020). We have implemented this STI screening program at 2 facilities, and at least 2 more facilities will be added by the end of fiscal year 2020. Our leadership supports implementation but appreciates the high demands on facility staff members. As such, leadership has requested a slow and steady rollout. Unpredictable events such as border surges and communicable disease outbreaks (eg, mumps, coronavirus disease 2019) provide additional challenges. The success of a long-term, agency-wide program will ultimately hinge on integration with existing infrastructure (eg, electronic health records, routine laboratory collections) and adequate staffing to sustain additional workload.
Limitations
Our study had several limitations. First, the cross-sectional study design did not allow us to infer causality from statistical analyses. Second, these findings, although informative, may not be generalizable to all immigration detention facilities or other settings. Thus, a larger study evaluating this program is necessary before implementing nationwide policy changes, including a better understanding of factors contributing to a detainee’s decision to opt out of testing. These factors could include, but are not limited to, cultural, religious, and/or language barriers; perceived risk; health literacy; and/or anticipated length of stay in custody. Third, STI risk factor variables were self-reported, which could hinder the validity of the findings because of response bias. Although the use of a sexual history risk factor variable would be ideal, such a variable was not consistently provided in the health assessment; therefore, we could not analyze it retrospectively. Fourth, for this program, we limited STI screening to urine and blood testing; therefore, we underestimated the STI prevalence of both chlamydia and gonorrhea by not obtaining pharyngeal or rectal samples. Fifth, urine specimens for gonorrhea and chlamydia testing were collected with a first morning void when possible, but some were collected later in the day; failure to collect all specimens as first void may have led to an underestimation of the gonorrhea and chlamydia test positivity rate in our detainee population. Finally, because this study was retrospective, the reasons detainees chose to opt out of testing could only be inferred or provided anecdotally by staff members.
Practice Implications
STIs are prevalent among immigrant detainees, and a routine screening program is feasible if operational considerations and timing of testing are weighted carefully. When extrapolated to the IHSC-staffed facility population for fiscal year 2018 (approximately 115 000 adults), even with an opt-out rate of approximately 50%, we would expect to successfully treat nearly 5000 patients each year, significantly decreasing the prevalence of STIs among this vulnerable population and the populations they interact with after release from custody. Opt-out testing limited to HIV would not be as effective as STI testing for this population because of the low prevalence of the disease 27 ; broader testing will offset the cost of HIV testing and make inclusion of this less prevalent yet critical infection reasonable.
Footnotes
Acknowledgments
The authors acknowledge the substantial contributions by all health care staff members at participating sites and Stewart Smith, DHSc, Assistant Director, ICE Health Service Corps, for his leadership and unwavering support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.