
Abstract
In 2014, California passed Assembly Bill 966, which required condom access for persons incarcerated in all 35 California state prisons (33 men’s and 2 women’s prisons). The California Correctional Health Care Services and the Sexually Transmitted Disease Control Branch and the Office of AIDS of the California Department of Public Health collaborated in a prison administration–led multidisciplinary implementation workgroup. Our workgroup, representing public health, correctional health, legal and legislative affairs, labor relations, and prison staff members, participated in 4 planning meetings during May–September 2015. We surveyed prison staff members and incarcerated men to identify and address potential challenges; conceptualized a tamper-resistant condom dispenser; developed educational materials, frequently asked questions for staff members, and fact sheets for the public; and conducted forums for custody and medical staff members at each prison. Key lessons learned included the need for high-level custody support, engagement of labor unions early in the decision-making process, and flexibility within defined parameters for sites to determine best practices given their unique institutional population, culture, and physical layout. Condom access was initiated at 4 prisons in July 2015 and expanded incrementally to the remaining 29 men’s prisons through July 2016. A total of 243 563 condoms were accessed in the men’s prisons, for an average of 354 condoms per 1000 population per month. The start-up dispenser cost was $69 825 (735 dispensers at $95 each). We estimated an annual condom cost of $0.60 per person. Although staff members and incarcerated men expressed concern that this legislation would condone sex and provide repositories for contraband, no serious adverse incidents involving condoms were reported. California demonstrated that condom access is a safe, low-cost intervention with high uptake for a large correctional system and provided a replicable implementation model for other states. Prison condom programs have the potential to decrease transmission of sexually transmitted infections (STIs) among incarcerated persons and their communities, which are often disproportionately affected by STIs, HIV, and other chronic diseases.
In-custody transmission of HIV and outbreaks of syphilis, gonorrhea, and hepatitis B are well documented. 1 -9 One large outbreak of syphilis in a California men’s prison in 2007-2008 resulted in 30 cases of early syphilis; 22 patients (73%) acquired syphilis while incarcerated. 2
Access to condoms in correctional settings has long been recommended by public health and correctional organizations internationally and in the United States. 10 -13 The World Health Organization calls for HIV prevention measures that are responsive to documented in-custody risk behaviors, including sexual activity, even when prohibited by law. 10,11 The United States is party to several legal standards governing human rights, including prisoners’ right to health care and prevention comparable to the community. 14,15 The Eighth Amendment to the US Constitution protects incarcerated persons from “cruel and unusual punishment” and guarantees the right to health care. 16 Given the vulnerability of incarcerated persons who are entirely dependent on correctional authorities for health care, the higher prevalence of HIV/sexually transmitted infections (STIs) compared with the community, and risk behaviors (eg, unprotected sex) while incarcerated, denying access to harm-reduction measures such as condoms arguably constitutes “deliberate indifference.” 15
Evaluations of condom programs in correctional settings found (1) no increases in sexual activity 17,18 or serious incidents involving condoms 19 -22 ; (2) that, when available, condoms are used during sex 17,19,23 -25 ; and (3) that providing condoms is likely to reduce the transmission of HIV and STIs. 26
Despite the demonstrated need for condom access in correctional settings, recommendations, and evaluations finding no increased risk of unintended consequences, the only correctional systems in the United States that provide condoms are local jails in Los Angeles, San Francisco, New York City, Philadelphia, and Washington, DC; state prisons in Mississippi (conjugal visits only); and all men’s prisons in Vermont (upon request from medical staff members) and California. The California Department of Corrections and Rehabilitation (CDCR) is the first state prison system in the United States to provide access to condoms from discreetly located dispensers without being observed by staff members.
In California, legislation passed in 2007 (Assembly Bill 1334) required CDCR to allow health care agencies or community-based organizations to distribute condoms inside state prisons. 27 In his veto memorandum, then-Governor Arnold Schwarzenegger directed CDCR to conduct a pilot project, noting that although sex is illegal between persons who are incarcerated in California prisons (PWICP), 28,29 providing condoms is “consistent with the need to improve correctional healthcare and overall public health.” 30
CDCR conducted a 1-year pilot project in 2007-2008. An evaluation by the California Correctional Health Care Services (CCHCS; the state agency that provides medical care to PWICP) and the California Department of Public Health (CDPH) found providing condoms to be feasible, safe, and low cost. 21 This pilot study was the first published systematic investigation comparing pre- and postintervention rule violation rates to address concerns that condoms would result in increased contraband (prohibited items per policy or penal code), sexual misconduct, and assaults on staff members.
Based on these findings, in 2014, California passed the Prisoner Protections for Family and Community Health Act (Assembly Bill 966), requiring CDCR to develop a 5-year plan to expand condom access in all state prisons. 31 We represented CCHCS in a CDCR-led multidisciplinary workgroup to coordinate implementation of the new law.
The purpose of this case study is to describe our process in designing and implementing a statewide condom access program in prisons and share program outcomes and lessons learned (Table).
Summary of key implementation steps, challenges overcome, and outcomes achieved during implementation of a condom access program at 33 men’s prisons, California, 2015-2016 a
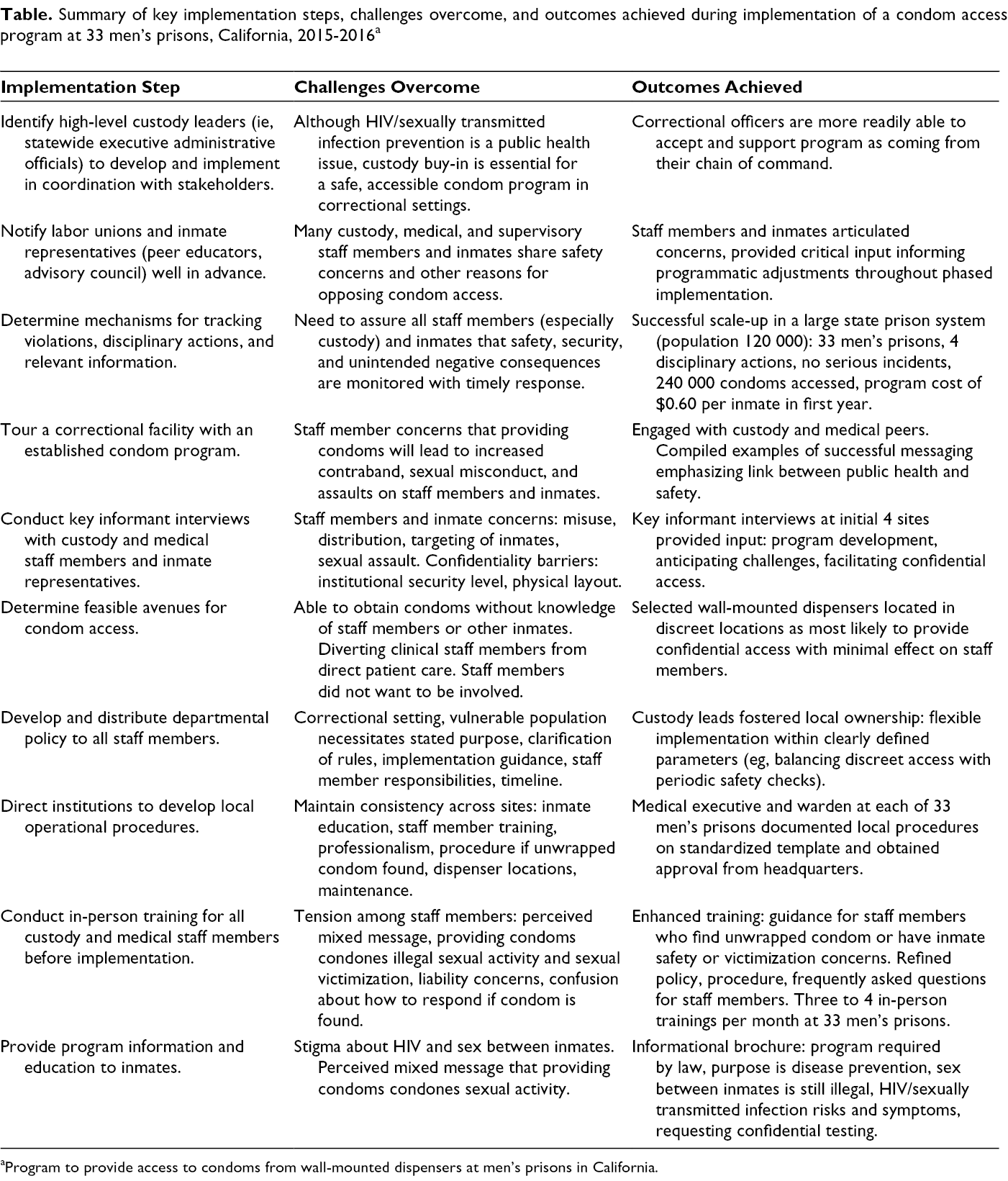
aProgram to provide access to condoms from wall-mounted dispensers at men’s prisons in California.
Methods
Two CDCR associate directors led the workgroup and program implementation in coordination with institutional custody and medical staff members representing 4 men’s prisons, 1 from each of the custodial missions: reception, general population, special populations (mental health, sensitive needs), and high security. CDCR preselected the 4 sites based on proximity to headquarters. Other workgroup members represented CDCR labor relations, regulations and policy, legal and legislative affairs, press office, CCHCS, and CDPH.
CDCR directed the workgroup to engage diverse stakeholders, determine avenues for accessing condoms, and standardize messaging for staff members and incarcerated persons. The condom program was to be implemented in phases, starting with the 4 preselected sites in July 2015 and expanding to the general population in all 33 men’s prisons by July 2016. Implementation would occur in restricted housing units (administrative, security, protective, psychiatric segregation, condemned) and women’s prisons at a later date. We engaged in 4 day-long workgroup meetings during May–September 2015. As each action item was completed (Table), workgroup leads sought feedback and CDCR approval to proceed.
We toured the San Francisco jail in May 2015 to learn about its condom access program, staff member training, and experiences. The custody and medical leads in the 4 preselected sites also conducted key informant interviews with custody (CDCR) and medical (CCHCS) staff members, union representatives, and PWICP, including the Men’s Advisory Council (MAC) and peer educators, for input on anticipated challenges and strategies for facilitating access. The MAC consists of PWICP at each prison who are elected by their peers to advise and communicate with the warden on matters that affect the incarcerated population. We determined guidelines for condom access after thoroughly considering the feasibility and confidentiality anticipated with a range of alternative avenues. We drafted a policy memorandum, institutional operational procedure (IOP) template, frequently asked questions (FAQs) for staff members, and an inmate educational brochure.
CDCR notified the unions (custody, medical, supervisory) and MAC in each prison of the plan to implement the program to make any necessary programmatic and training adjustments before implementing statewide. In the month before implementation in each prison, the workgroup leads and selected members conducted site visits and training for custody and medical staff members.
Each site reported the numbers of condoms accessed, rule violations, disciplinary actions, serious incidents, and other relevant information to the workgroup weekly through July 2016. We estimated the number of condoms dispensed per 1000 average daily inmate population per month across all 33 sites during the phased implementation from aggregate numbers reported to the workgroup. We estimated the start-up cost for the dispensers and the annual cost of condoms per inmate based on the population in the 33 men’s prisons as of December 2015.
Outcomes
Information Gathering
During our tour of the San Francisco jail, we observed condom dispensers in the gymnasium and housing units. From health department and custody staff members, we learned that successful messaging (Table) emphasizes the link between public health and safety, that preventing disease protects all staff members and incarcerated persons who may be exposed to infectious agents, that contraband is just as easily stored and transported in materials other than condoms (eg, latex gloves, plastic wrap), and that rule violations should be issued only for sexual activity or other misconduct but not for mere possession of a condom.
We received a wide range of input from key informant interviews with PWICP and staff members in the 4 preselected prisons (Table). PWICP and staff members were generally accepting in the reception center setting, where turnover of incarcerated persons is high. In higher security–level settings, PWICP and staff members were concerned about misuse of condoms, PWICP being targeted for accessing condoms, and sexual assault. PWICP commented that providing condoms is “safer than not” but should be “out of sight and out of mind.” In the general and special population settings, PWICP acknowledged sexual activity occurs and were mainly concerned about how condoms would be distributed, noting, “Don’t put it where everyone sees it, but put it out there.” Staff members who preferred condom access through dispensers cited confidentiality and not wanting to be involved. Some staff members were interested in considering access through medical and mental health appointments but expressed concern that this process could interfere with delivering health care.
Condom Access
We weighed the potential benefits and risks of condom distribution alternatives, including providing condoms in new-arrival toiletry kits, in the canteen, through medication-dispensing windows, by request during medical appointments, from PWICP peer educators, and ordering from the approved supplies catalogue. Our main concerns were that adding condoms to the toiletry kits would be a difficult message at intake, allowing or requiring PWICP to obtain condoms through the sick-call process could divert clinical staff members unnecessarily from direct patient care activities, and the lack of confidentiality or inability to access condoms without the knowledge of staff members or other PWICP with most of these methods. We settled on dispensers as providing the most confidential access with the least involvement of staff members (Table).
To avoid the frequent vandalism of dispensing machines that occurred in the pilot program, we conceptualized a tamper-resistant dispenser made from a single piece of polythermoplastic, evaluated prototypes from a contracted vendor, and selected a model for mass production (Figure). Our dispenser is shatterproof; has no moving or metal parts that can be damaged or used as weapons; is transparent, making it difficult to hide contraband in it; and does not require any particular brand or packaging for the condoms.

Examples of discreet locations for wall-mounted condom dispensers during implementation of a condom access program in 33 men’s state prisons, California, 2015-2016.
Policy and Procedure
Before implementing the condom access program, the CDCR secretary issued a policy memorandum to the custody and medical executives in all prisons (1) to provide the public health and safety rationale for providing condoms; (2) to reiterate that by providing condoms, CDCR is not condoning illegal sexual behavior between PWICP; (3) to provide guidance for selecting dispenser locations; and (4) to set the timeline for program expansion (Table). Custody administrators were directed to install the dispensers in various areas in inconspicuous locations whenever possible to enable discreet access while allowing staff members to conduct periodic checks to maintain safety and security.
The chief executive officer for clinical services and the warden in each prison were required to document their plan for PWICP access to condoms in the IOP template and submit it to headquarters for approval before implementation (Table). The template provided consistency across sites in describing the purpose of the program, population-wide awareness through brochures and posters, staff training and expectation of professionalism, and procedures to follow if a condom is found outside of its wrapper. Each site included a list of dispenser locations and responsibility for refilling them.
Training and Education
The all-staff trainings (Table) at each prison in the month before implementation and FAQs addressed the inherent tension around the perceived mixed message: that by providing condoms, CDCR is condoning sexual activity, including sexual victimization, which is reportable under the Prison Rape Elimination Act. 32 Clarification was provided to staff members that allowing PWICP access to condoms is not in conflict with the Prison Rape Elimination Act because the purpose of providing access to condoms is to prevent the spread of disease while continuing to investigate and report sexual contact between inmates according to existing regulations. The other main issue addressed was how staff members should respond if they find a condom outside its packaging. Emphasis was placed on continuing to follow existing protocols, including supervisor notification and confidential interviews to assess if PWICP in the area have any safety concerns or may have been victimized, and that the presence of a condom alone is not evidence of an assault or any other violation.
The education for PWICP was designed for use as a brochure or poster to display next to the dispensers (Table). Information listed provides a brief statement about the public health and safety purpose of the state law requiring CDCR to provide condoms; that providing condoms does not change the fact that sexual activity between PWICP is illegal; descriptions of the symptoms and risk factors for HIV, STIs, and viral hepatitis; that inmates may request confidential screening at any time; and to dispose of used or expired condoms by flushing them down the toilet or discarding them in the trash.
Implementation and Costs
The condom program was implemented at all 33 men’s prisons starting with the 4 preselected prisons in July 2015 and adding 3 to 4 prisons each month from November 2015 through July 2016. A wide variety of dispenser locations were reported: gymnasiums, housing units, clinic waiting rooms, educational and library facilities, hallways and stairwells, and next to telephone booths and institutional mailboxes.
A total of 243 563 condoms were dispensed during 1 year of the phased implementation. Overall, 354 condoms were dispensed per 1000 average daily prison population per month. Only 4 disciplinary actions for use of a condom to store controlled substances or contraband were reported from the 33 sites, and no serious incidents involving a condom were reported.
Start-up and maintenance costs were minimal. CDCR ordered 735 dispensers at $95 each from the manufacturer, making available 21 dispensers per prison (33 men’s and 2 women’s). Assuming installation of at least 4 dispensers in a typical 4-yard prison, we estimated a cost per site ranging from $380 for 4 dispensers to $1995 if all 21 dispensers were used. We estimated the cost of condoms (14 cents each) at $49.60 per 1000 inmates per month, or about 60 cents per inmate annually. For CDCR’s large prison population (about 120 000), the estimated annual cost for condoms is about $70 000. Given the treatment cost of $253 000 to $402 000 (in 2011 dollars; $289 450 to $459 916 in 2019 dollars), 33 few HIV infections need to be averted for the program to be cost neutral.
Lessons Learned
Our workgroup benefited from lessons learned from the pilot project. These lessons included (1) the importance of engaging influential and respected PWICP (eg, MAC and peer educators), (2) the use of consistent and clear messaging that avoids stigma, and (3) the discreet placement of dispensers for confidentiality and to prevent disruptions to daily activities because of vandalism or PWICP being targeted by others, including staff members, for accessing condoms. During the pilot project, we also learned not to assume that all health care staff members will agree that PWICP should have access to condoms, for many of the same reasons as custody staff members (eg, concern about misuse of condoms, PWICP being targeted for accessing condoms, sexual assault).
High-level executive support was critical for success both during the condom pilot project (which was governor ordered) and during statewide program implementation (from the CDCR secretary and director). Translating this lesson learned (about the importance of high-level executive support) to the workgroup and the institutional level, we felt that having associate directors and wardens take the lead, in consultation with medical and public health staff members, helped correctional officers support the program as coming from the custody chain of command (Table).
California has a large prison system with 35 institutions dispersed across 950 miles from the Oregon border to the Mexico border; therefore, it is not amenable to the model of relying on health care agencies or community-based organizations to distribute condoms. Although this model worked well during the pilot project, we felt that it would be challenging to scale up. To ensure consistency and sustainability, CDCR implemented a state-run, state-funded condom program.
To ensure that all concerns about safety, procedures, investigations, and inmate discipline are addressed, it was essential to include the custody and medical labor unions early in the decision-making process (Table). Custody union representatives in particular felt that comprehensive and mandatory training was needed, including discussion of scenarios and expectations for correctional officers who find an unwrapped condom and clarification about complaints of sexual assault in an environment where condoms are allowed. CDCR’s legal team conducted an analysis in 2015 and concluded that the presence of a condom alone is not evidence of misconduct or assault and that existing procedures should be followed in consultation with supervisors to ascertain, through confidential interviews, whether inmates in the vicinity have any safety or victimization concerns. We used these findings to inform the policy memorandum, FAQs, and all-staff training to support correctional officers’ confidence that they are using best practices to maintain safety and security while adhering to policy and the law.
California developed a prison condom access program that can be replicated in other states and correctional settings that range in size, security level, and population characteristics. High-level custody support and flexibility within defined parameters (eg, providing the most discreet or confidential access possible) facilitated program implementation across sites. Program ownership was enabled at the local level by determining best practices given their institution’s unique population, culture, and physical layout.
Footnotes
Acknowledgments
The authors acknowledge our custody partners at CDCR headquarters and the initial prison sites for their effective leadership; peer mentorship; engaging diverse stakeholders including workgroup members with public health, communications, legal, and legislative expertise; and overall dedication to ensure successful program implementation. The authors also thank Anna Steiner and Valorie Eckert, formerly with the California Department of Public Health, Sexually Transmitted Diseases Control Branch and Office of AIDS, respectively, for their invaluable contributions to the workgroup, including developing educational materials for incarcerated persons and messaging for staff members and the public.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support with respect to the research, authorship, and/or publication of this article.