
Abstract
Objectives:
Screening tools in which participants self-report sexual behaviors can identify people at risk of HIV acquisition for enrollment in preexposure prophylaxis (PrEP). We compared enrollment outcomes (ie, receiving PrEP vs being excluded by a counselor or declining PrEP) in Mexico’s PrEP demonstration project and evaluated the validity of a 4-criteria PrEP eligibility tool in which participants self-reported risk behavior—having condomless anal sex, transactional sex, a partner living with HIV, or a sexually transmitted infection—as compared with PrEP eligibility assessed by a counselor.
Methods:
We recruited men who have sex with men and transwomen who were offered PrEP services in Mexico. We characterized participants according to enrollment outcome and identified underlying factors through logistic regression analyses. We calculated the sensitivity and specificity of the self-reported risk criteria, using the counselor’s risk assessment as the point of reference.
Results:
Of 2460 participants, 2323 (94%) had risk criteria of HIV acquisition according to the 4-criteria tool; 1701 (73%) received PrEP, 247 (11%) were excluded by a counselor, and 351 (15%) declined PrEP despite being considered eligible by the counselor. Participants who were excluded or who declined PrEP were less likely to report HIV risk behaviors than those who received PrEP, and participants who declined PrEP were more likely to be transwomen (vs men who have sex with men) and aged ≤25 years (vs >25 y). The 4-criteria risk tool had high sensitivity (98.6%) and low specificity (29.8%).
Conclusion:
The screening tool identified most participants at risk of HIV acquisition, but counselors’ assessment helped refine the decision for enrollment in PrEP by excluding those with low risk. Public health strategies are needed to enhance enrollment in PrEP among some groups.
Keywords
An estimated 100 000 new HIV infections occurred in 2020 in Latin America, of which 92% were among key populations (men who have sex with men [MSM], transgender women, sex workers, and people who inject drugs) and their partners. Countries in Latin America thus need to fortify prevention programs to target key populations. 1 Preexposure prophylaxis (PrEP)—antiretroviral drugs to prevent HIV infection—is highly effective 2 and recommended as an additional tool in a comprehensive prevention package for people at high risk of HIV acquisition.3,4
Delivering PrEP to key populations at high risk of HIV is a highly cost-effective strategy. 5 Thus, correctly identifying eligible people is essential and is particularly relevant where PrEP programs have limited capacity. 6 However, identifying people at high risk of HIV is challenging; furthermore, definitions of “high risk” vary and often lack a solid evidence base. 7 In addition, not all people in key populations may be at risk of HIV acquisition, so programs must differentiate among them.
One approach for identifying eligible people for PrEP is to screen potential users by applying a tool developed and evaluated for specific contexts and populations. 8 Simple screening tools are needed because the rapid identification of eligible people and the prompt delivery of PrEP could increase uptake. 9 For example, HIV risk–screening tools to identify potential PrEP users among MSM include behaviors such as receptive condomless anal sex (CAS), multiple sexual partners, sexual partner living with HIV (PLWH), and a history of sexually transmitted infections (STIs).10-12 Nevertheless, in 2019, the US Preventive Services Task Force found no well-validated accurate tools to assess HIV risk. 13
From 2018 through 2021, an international demonstration project, ImPrEP, implemented PrEP services in Mexico. The project focused on MSM and transgender women, 14 2 key populations with a high prevalence of HIV.15,16 Candidates were preliminarily considered at risk of HIV if they met at least 1 of 4 risk criteria: CAS, transactional sex, a PLWH, or an STI. A counselor then complemented the initial risk screening through an in-depth discussion with the candidate regarding the candidate’s risk of HIV acquisition. ImPrEP’s service provision, which centered on counseling, aligned with a community-based organization (CBO) model that provided much of Mexico’s HIV response from 2006 through 2018; this model was created to better reach key populations through community-based services led by peers. 17
In this study, we aimed to identify factors among MSM and transgender women that were associated with either receiving PrEP or being excluded by a counselor or declining PrEP within ImPrEP. We also studied the validity of a self-reported PrEP eligibility assessment based on 4 criteria for HIV risk as compared with a counselor’s assessment of PrEP eligibility.
Methods
ImPrEP–Mexico
ImPrEP offered PrEP services at no cost to MSM and transgender women in Mexico through 4 study sites: a public HIV clinic and 3 CBOs in Mexico City, Guadalajara, and Puerto Vallarta. The study sites promoted PrEP services through sexual health services, social media campaigns, and informative talks.
Study Questionnaire
Members of the research team and counselors asked adult MSM and transgender women attending the study sites to complete a questionnaire, regardless of whether they were seeking PrEP. Research teams and counselors approached most candidates during service hours; however, research teams and counselors approached some candidates during informative talks after hours when no HIV testing or PrEP services were available.
Participants answered questions about the 4 risk criteria and additional risk factors, as well as sociodemographic information, screening site, and main reason for attending the study site.
Screening and Enrollment
Project counselors preliminarily considered participants at risk of HIV when they self-reported any of the 4 risk criteria in the screening tool. The counselors further discussed risk with the participants to confirm or reject the screening tool’s determination of risk. Counselors then invited eligible participants to see a medical provider to identify any preexisting health conditions to contraindicate PrEP; participants without contraindications were offered PrEP.
To determine factors associated with enrollment in PrEP, we defined 3 possible outcomes among participants who self-reported risk according to the 4 criteria: received PrEP, excluded by a counselor, and declined PrEP. We determined participants as “received PrEP” if those who were confirmed to be at risk of HIV acquisition by the counselor (ie, eligible for PrEP) accepted PrEP. We determined participants as “excluded by counselor” if they were considered by the counselor to be without risk of HIV acquisition based on behaviors (ie, ineligible for PrEP) and were not enrolled in the program. We determined participants as “declined PrEP” if they were eligible (ie, considered at risk by the counselor) and did not receive PrEP, either because they did not want to or because there were no HIV testing services available when they were screened and, despite being invited, did not return to receive PrEP.
Counselors aimed to perform the entire screening process, including HIV testing, on the same day. If HIV testing could not be offered on the same day (eg, when the screening process started during informative talks after hours), counselors scheduled participants for other days and reminded them of their appointments by calling and rescheduling if necessary. Counselors also evaluated participants who were considered not at risk of HIV acquisition according to the screening tool. Participants discussed their answers with a counselor to verify whether they were truly ineligible.
Counselors offered participants deemed ineligible at any point other prevention options and referred those with a positive HIV test result to treatment. We did not include participants with a positive HIV test result in our analyses. All participants provided informed consent verbally and in writing. The institutional review board of the National Institute of Public Health of Mexico approved this study (CI-241-2020, CI:1515 09-01-2018).
Statistical Analysis
We used a flowchart to describe the screening and enrollment process, which included the following steps: (1) availability of a negative HIV test result, (2) result of risk assessment based on the 4 self-reported HIV risk criteria, (3) counselor’s eligibility decision based on identified risk (and the medical provider’s identification of medical contraindications), and (4) enrollment outcomes (received PrEP, excluded by counselor, and declined PrEP). For the validity assessment, we calculated the sensitivity and specificity of the results of the 4 self-reported risk criteria (at risk or not at risk), taking the counselor’s eligibility decision based on identified risk (eligible or ineligible) as the point of reference.
We described the sociodemographic and HIV risk characteristics of all participants and compared those who received PrEP with those who were excluded by a counselor and with those who declined PrEP. We used the Pearson χ2 test to identify differences between group bivariable comparisons, with P < .05 considered significant. We used multivariable logistic regression analyses to identify variables with significant differences associated with being excluded by a counselor or declining PrEP versus receiving PrEP. Finally, we discussed screening and enrollment results with the project’s counselors to obtain feedback.
Results
From November 2018 through October 2020, 2460 participants completed the questionnaire (some did not answer certain questions). Most participants were aged >25 years (70%, 1719/2460), MSM (96%, 2357/2457), highly educated (60% had a bachelor’s degree or more, 1465/2460), and screened in the public HIV clinic (67%, 1655/2460), and most attended a study site to seek PrEP (74%, 1830/2458) (Table 1).
Characteristics of participants screened in ImPrEP–Mexico, by enrollment outcome, 2018-2020 a
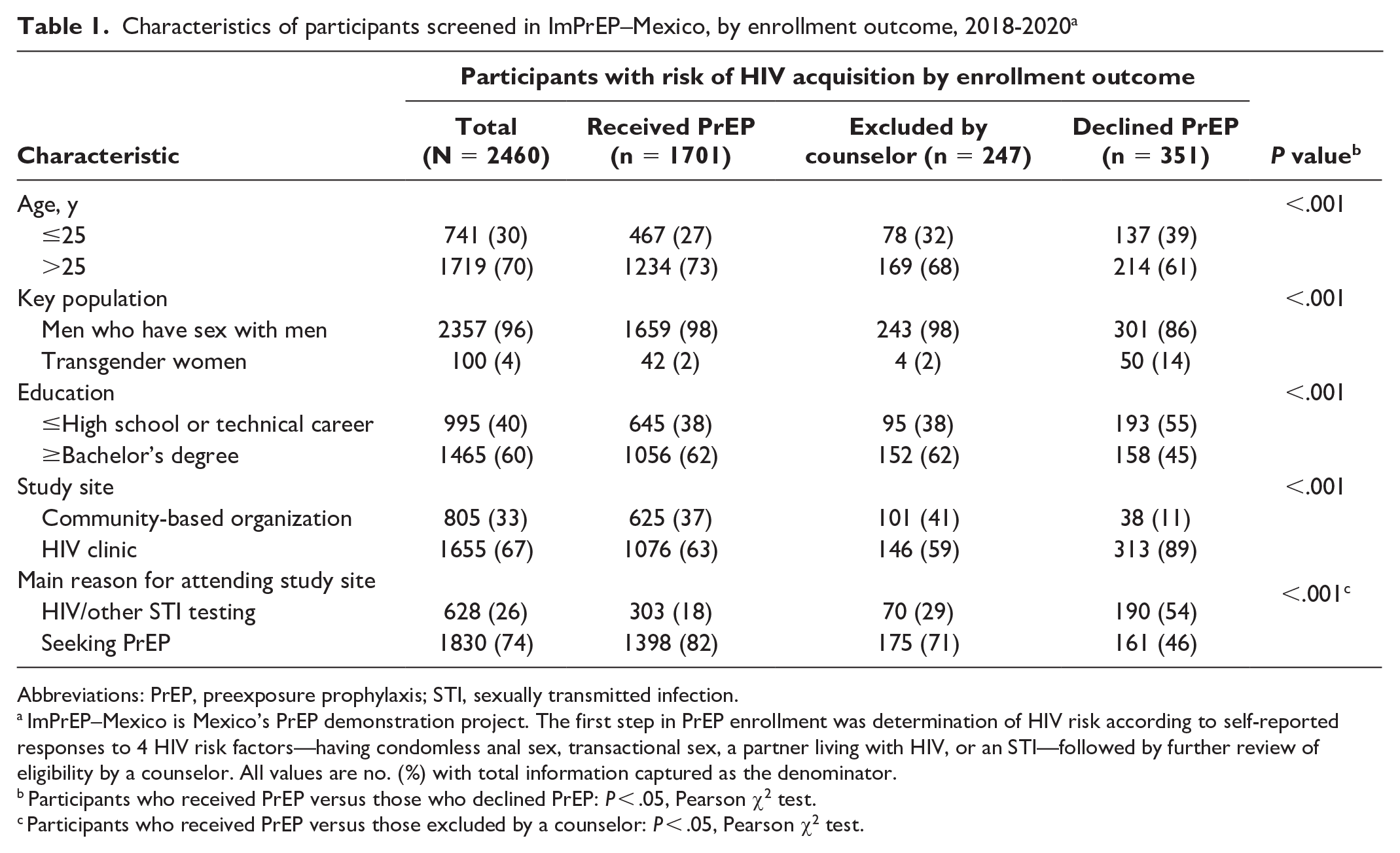
Abbreviations: PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
ImPrEP–Mexico is Mexico’s PrEP demonstration project. The first step in PrEP enrollment was determination of HIV risk according to self-reported responses to 4 HIV risk factors—having condomless anal sex, transactional sex, a partner living with HIV, or an STI—followed by further review of eligibility by a counselor. All values are no. (%) with total information captured as the denominator.
Participants who received PrEP versus those who declined PrEP: P < .05, Pearson χ2 test.
Participants who received PrEP versus those excluded by a counselor: P < .05, Pearson χ2 test.
Of the 2460 participants, CAS in the past 6 months was the most frequent HIV risk behavior (82%, 2006/2459). More than one-quarter of participants reported anal sex with a PLWH (28%, 698/2452), but even more did not know the HIV status of their past partners (41%, 1003/2452). Fewer participants indicated having transactional sex (22%, 548/2442) or having an STI (17%, 413/2452) in the past 6 months. Other risk factors included having >5 male sexual partners (65%, 1583/2442) and using a noninjectable drug (58%, 1407/2446). Only 13% (316/2454) had used postexposure prophylaxis in the past 12 months, and 44% (1075/2442) had ever considered stopping condom use (Table 2).
HIV risk factors among participants enrolled in ImPrEP–Mexico, by enrollment outcome, 2018-2020 a
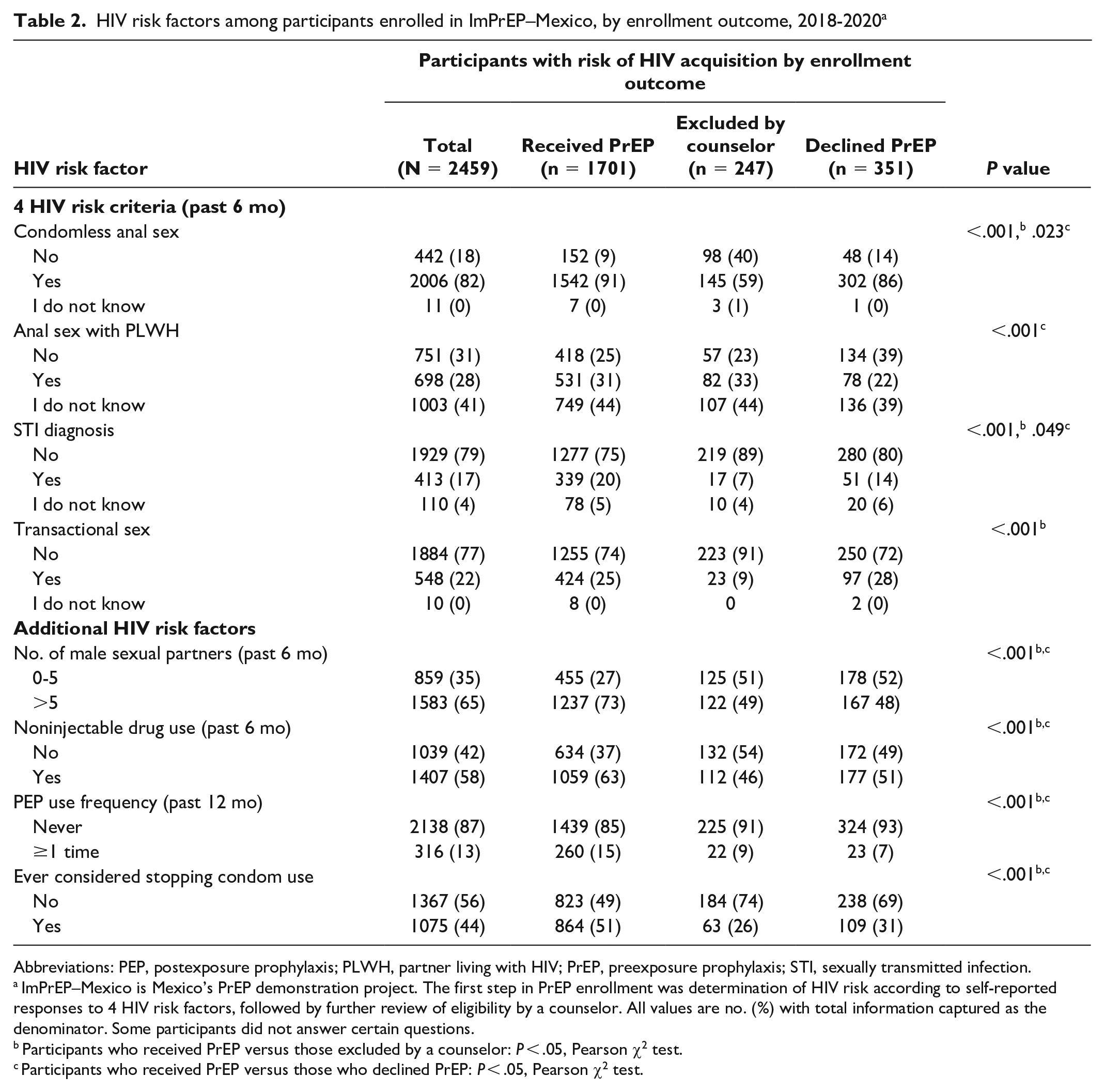
Abbreviations: PEP, postexposure prophylaxis; PLWH, partner living with HIV; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
ImPrEP–Mexico is Mexico’s PrEP demonstration project. The first step in PrEP enrollment was determination of HIV risk according to self-reported responses to 4 HIV risk factors, followed by further review of eligibility by a counselor. All values are no. (%) with total information captured as the denominator. Some participants did not answer certain questions.
Participants who received PrEP versus those excluded by a counselor: P < .05, Pearson χ2 test.
Participants who received PrEP versus those who declined PrEP: P < .05, Pearson χ2 test.
Of 2460 participants, 2072 (84%) had a negative HIV test result; the remaining were not tested for HIV (Figure). Of 137 (6%) who did not report any of the 4 risk criteria, 64% (n = 87) had a negative HIV test result and 36% (n = 50) were not tested. Of 137 participants not at risk per the screening tool, 21% (n = 29) were afterward deemed eligible for PrEP by the counselors based on risk, and 79% (n = 108) were deemed to have a lack of risk by the counselors. Of 137 who did not report any of the 4 risk criteria, 20% (n = 27) eventually received PrEP. The counselors explained that they enrolled a few participants in PrEP without past HIV risk per the 4 criteria because they reported planning to engage in risky behavior in the following weeks (eg, starting sex work). Also, the counselors identified some eligible participants who had answered the screening tool incorrectly.
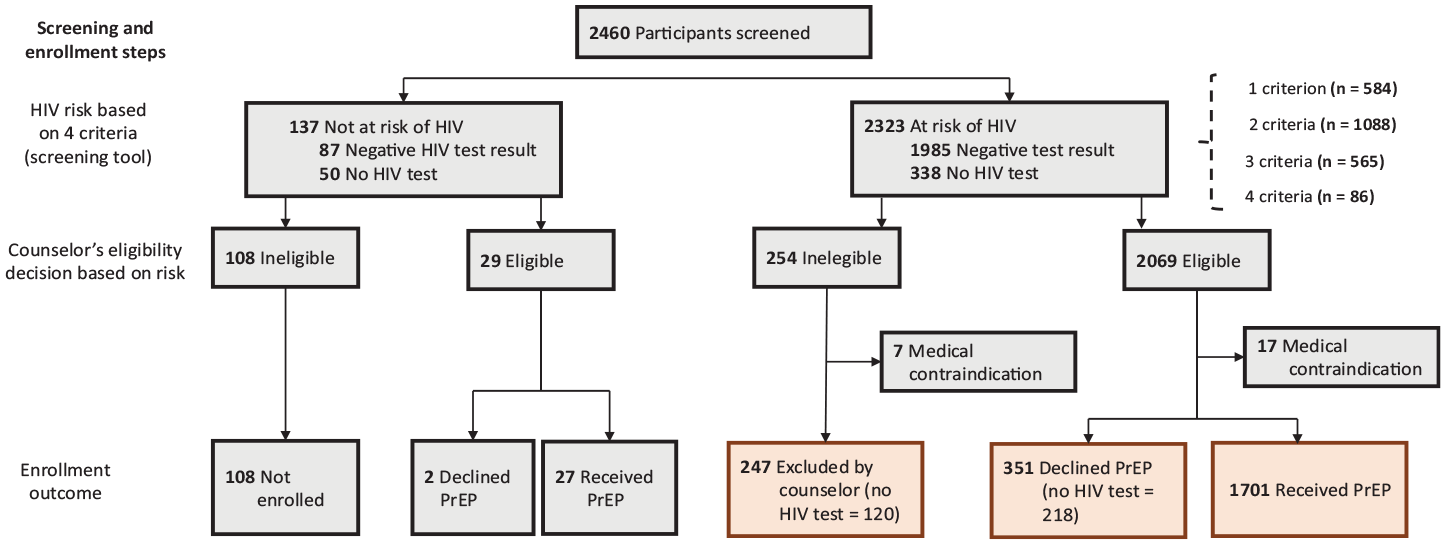
Screening and enrollment steps in Mexico’s preexposure prophylaxis (PrEP) demonstration project (ImPrEP–Mexico), 2018-2020. The first step in PrEP enrollment was determination of HIV risk according to self-reported responses to 4 HIV risk factors—having condomless anal sex, transactional sex, a partner living with HIV, or a sexually transmitted infection—with eligibility for PrEP further reviewed by a counselor.
According to the 4 criteria, 94% of participants (2323/2460) were at risk for HIV. Of these, 584 (25%), 1088 (47%), 565 (24%), and 86 (4%) fulfilled 1, 2, 3, and all 4 risk criteria, respectively (106 were considered at risk because they answered a combination of “I do not know” and “no”). Among 2323 participants who were at risk of HIV according to the 4 criteria, 1985 (85%) tested negative for HIV and 338 (14%) did not get tested (Figure).
Of the 2323 participants at risk of HIV, 11% (n = 254) were considered ineligible for PrEP by counselors per the screening tool, of which 47% (120/254) were not tested for HIV. Of the 254 considered ineligible for PrEP, 3% (n = 7) were excluded because of medical contraindications, resulting in the exclusion of 247 of 2323 participants (11%) who were assessed by counselors to be at risk based on the 4 criteria (Figure). When asked about these data, the counselors explained that some participants had answered “no” and “I do not know” to all 4 questions, making them eligible in theory, but they did not identify a recent risk factor during counseling. The counselors stated that other participants reported always using a condom with a PLWH or having condomless sex with a PLWH who had an undetectable viral load. Although the protocol required enrolling people who had anal sex with a PLWH, the counselors considered that not all participants who met this requirement were at risk.
Of 2323 participants considered at risk according to the screening tool, the counselors confirmed 89% (n = 2069) as eligible, of which 11% (n = 218) lacked an HIV test and 1% (n = 17) presented with medical contraindications. Of 2323 participants considered at risk according to the screening tool, 15% (n = 351) declined PrEP and 73% (n = 1701) received PrEP (Figure). Counselors noted that many participants filled in the questionnaire during the informative sessions, which took place when no HIV testing was offered (after service hours); these participants were asked to come back for an HIV test and to finish enrollment. Many never showed up—some because of lack of interest and others because the project and service hours were not compatible with their lifestyles.
When we compared results from participants’ 4 risk criteria with the counselors’ eligibility decisions based on risk, sensitivity of the results of the 4 risk criteria was 98.6% (95% CI, 98.2%-99.1%) and specificity was 29.8% (95% CI, 28.0%-31.6%) (Table 3). The positive and negative predictive values were 89.1% (95% CI, 88.0%-90.3%) and 78.8% (95% CI, 77.2%-80.5%), respectively.
Sensitivity and specificity for HIV risk according to the 4-criteria tool as compared with the counselor’s eligibility decision (ie, final risk assessment) as a point of reference in ImPrEP–Mexico, 2018-2020 a
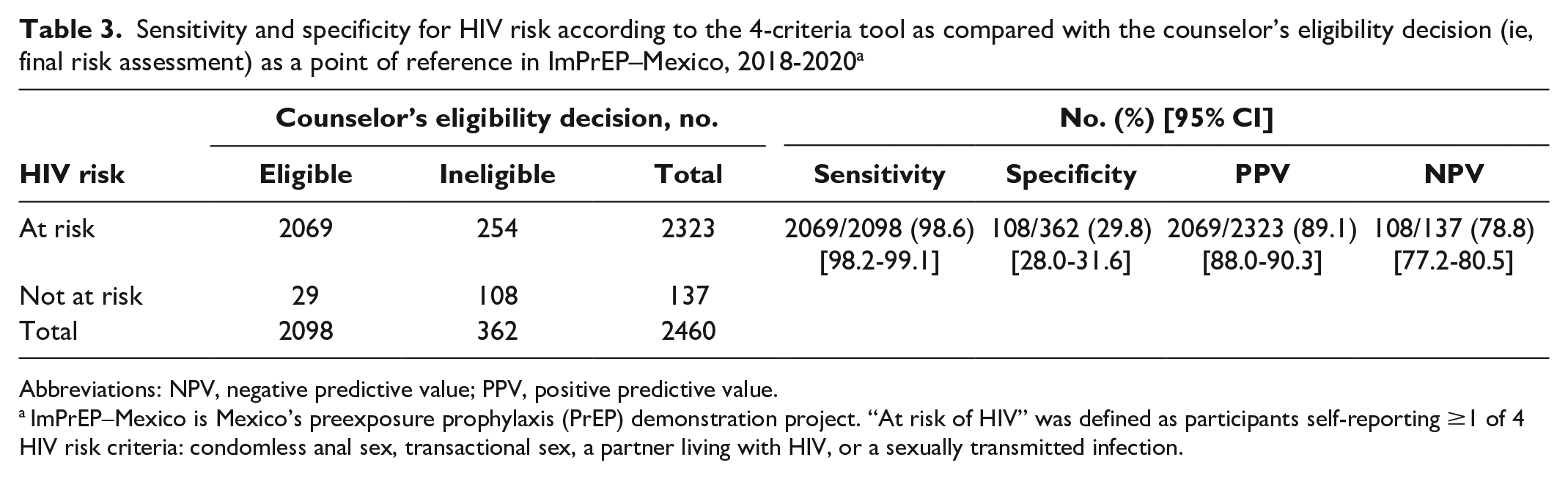
Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
ImPrEP–Mexico is Mexico’s preexposure prophylaxis (PrEP) demonstration project. “At risk of HIV” was defined as participants self-reporting ≥1 of 4 HIV risk criteria: condomless anal sex, transactional sex, a partner living with HIV, or a sexually transmitted infection.
Among differences identified through logistic regression between participants who were excluded by counselors and participants who received PrEP, the odds of being excluded were lower among those who visited the study site seeking PrEP than among those seeking testing (adjusted odds ratio [AOR] = 0.70). In addition, participants who indicated the following risk factors were less likely to be excluded than those who did not present the risk factors: CAS (AOR = 0.17), an STI diagnosis (AOR = 0.38), transactional sex (AOR = 0.29), >5 male sexual partners (AOR = 0.64), postexposure prophylaxis use (AOR = 0.63), and considering stopping condom use (AOR = 0.40) (Table 4).
Multivariable logistic regression analysis of factors associated with being excluded by a counselor for PrEP and declining PrEP as compared with receiving PrEP among participants with HIV risk in ImPrEP–Mexico, 2018-2020 a
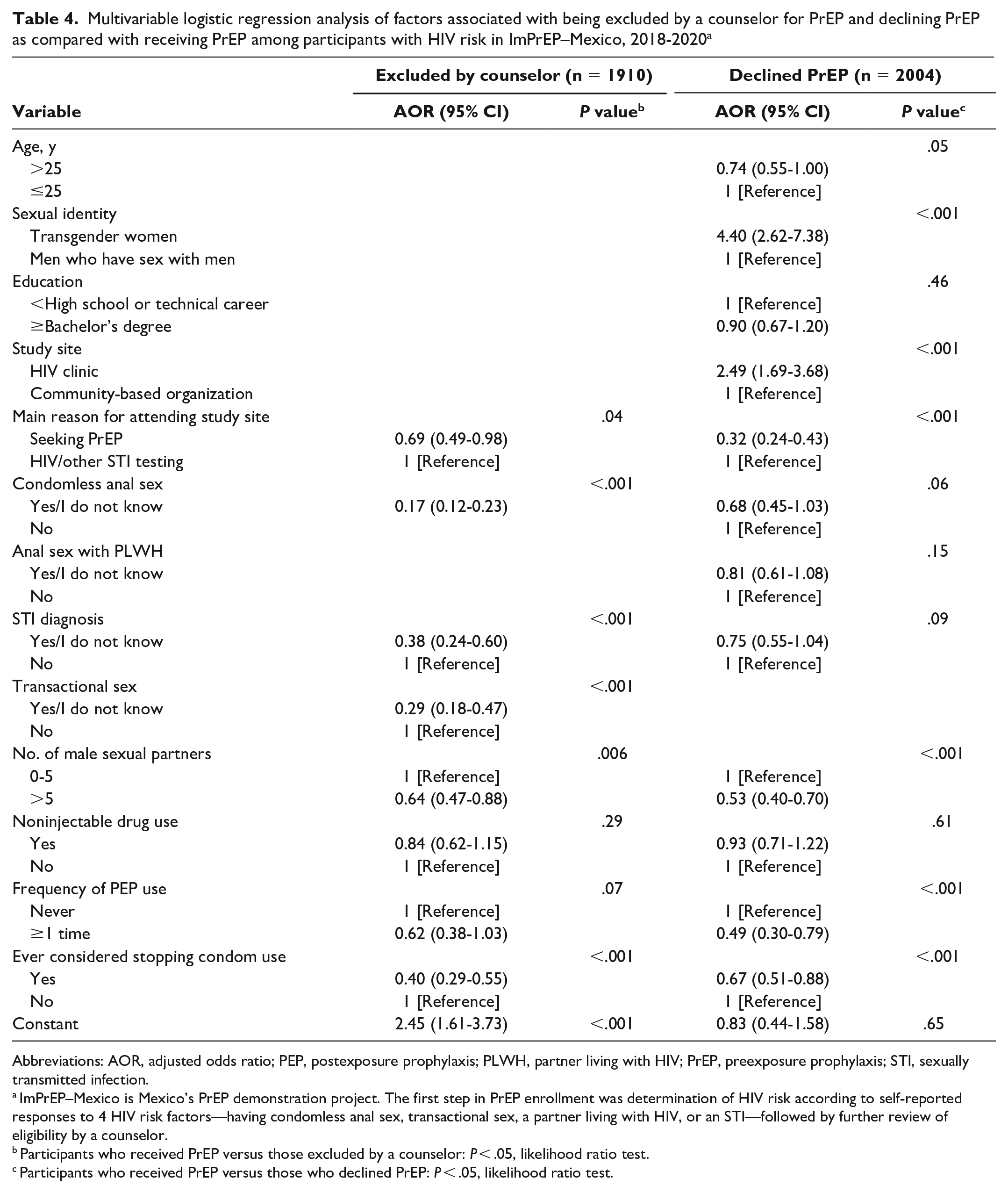
Abbreviations: AOR, adjusted odds ratio; PEP, postexposure prophylaxis; PLWH, partner living with HIV; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
ImPrEP–Mexico is Mexico’s PrEP demonstration project. The first step in PrEP enrollment was determination of HIV risk according to self-reported responses to 4 HIV risk factors—having condomless anal sex, transactional sex, a partner living with HIV, or an STI—followed by further review of eligibility by a counselor.
Participants who received PrEP versus those excluded by a counselor: P < .05, likelihood ratio test.
Participants who received PrEP versus those who declined PrEP: P < .05, likelihood ratio test.
Among differences identified through logistic regression between participants who declined PrEP and those who received PrEP, the odds of declining PrEP were lower among those aged >25 years (AOR = 0.74) versus ≤25 years. Participants who visited the study site seeking PrEP (AOR = 0.32) had lower odds of declining PrEP when compared with those seeking testing. However, being a transgender woman versus a man who has sex with men (AOR = 4.40) and attending the public HIV clinic versus a CBO (AOR = 2.49) were positively associated with declining PrEP. Participants who reported the following risk factors also had low odds of declining PrEP: CAS (AOR = 0.68), an STI diagnosis (AOR = 0.75), >5 male sexual partners (AOR = 0.53), past postexposure prophylaxis use (AOR = 0.49), and considering stopping condom use (AOR = 0.67) (Table 4).
Discussion
During the ImPrEP project, a screening tool was coupled to counseling sessions to identify and enroll MSM and transgender women with a risk of HIV in PrEP. This screening process was successful in enrolling most but not all participants who were deemed eligible. Among participants considered eligible for PrEP by a counselor, 15% declined it. Although these participants reported fewer risk factors than eligible participants who accepted PrEP, they met ≥1 of 4 risk criteria and were confirmed by counselors to be at risk of HIV. These participants tended to be younger (aged ≤25 vs >25 y) and transgender women (vs MSM), indicating potential disparities in program engagement. Counselors in our study noted that some participants declined the PrEP program because of the high level of commitment required. Studies conducted in the United States have identified transportation barriers, sexual minority status, and HIV-related stigma as impediments to PrEP uptake. 18 Thus, programs must identify strategies to reduce these barriers (eg, by adopting more flexible PrEP schemes and appointments).
The participants who declined PrEP were more likely to have been screened at the public HIV clinic than at CBOs. The public HIV clinic screened more than half of participants and arranged PrEP information sessions. The large number of people who attended this study site challenged the ability of counselors to provide personalized follow-up. According to the counselors, participants who were screened and required to return on a separate day for testing and enrollment frequently failed to return. Therefore, not only are same-day screening and enrollment critical to reducing the number of participants who decline PrEP, 19 but so is directly linking PrEP information sessions with the screening and enrollment process.
The counselors used their professional judgment to exclude candidates who were deemed ineligible despite fulfilling the initial screening criteria. Thus, the screening assessment with the 4 self-reported HIV risk criteria had low specificity when compared with the counselors’ assessment of HIV risk. The counselors explored additional risk factors and requested further information from participants; they decided to exclude those who had a PLWH but were not necessarily exposed to risk. They also enrolled a few participants in PrEP who did not initially meet the 4 HIV risk criteria but anticipated future risks or misunderstood the questions. Similarly, Australia’s PrEP demonstration project, PRELUDE, concluded that allowing clinicians to exercise their discretion when prescribing PrEP was warranted after participants used a risk assessment tool. 20
Screening of HIV risk in PrEP programs needs to be short and effective. 9 Screening tools can help identify people at risk, but they will have limitations. In addition, revalidating an existing screening tool in a new context requires human and economic resources. Counselor assessments were added to screening in ImPrEP, which corresponded with Mexico’s history of a CBO-led HIV response 17 and a lack of a validated tool. The counseling approach sought to reduce the limitations inherent in any instrument while promoting shared decision-making for PrEP, which can improve health outcomes by considering the client’s preferences and the counselor’s recommendations. 21 Nevertheless, assessments that do not systematically follow a set of criteria can be prone to the counselor’s potential biases, such as differing interview depths, misconceptions about HIV risk, and even stigma. As such, counselors who screen for HIV risk should be trained to increase their objectivity.
Only a small number of participants did not meet any of the 4 self-reported risk criteria. The 4 risk criteria used in this study were not sufficiently specific to identify people who were not at substantial risk in this setting (ie, study sites offering sexual health services). To better identify those not at risk of HIV, adding more detailed questions to ascertain risk or increasing the cutoff to require at least 2 risk criteria instead of 1 may be beneficial (although at the cost of sensitivity).
Most participants who were enrolled in this study were at substantial risk of HIV based on the CAS criteria; however, they also indicated the other 3 criteria. Previous screening tools for HIV risk included CAS and STI diagnosis10-12 and anal sex with PLWH 10 but not transactional sex. These tools considered factors such as multiple sexual partners10-12 and drug use,11,12 which were included in this study as additional HIV risk factors (but not in the 4-criteria screening tool).
The 4 risk criteria used to identify HIV risk showed higher sensitivity (98.6%) but lower or similar specificity (29.8%) than the HIV risk–screening tools used in other studies.10,12,22,23 However, these studies compared self-reported HIV risk with subsequent seroconversions in retrospective cohorts. 11 In our study, the counselor’s assessment was helpful as a separate predictor of HIV risk, although it was a substitute for the unknown condition of actual HIV acquisition.
Limitations
This study had several limitations. First, the study population was limited to MSM and transgender women; additional research is necessary to examine obstacles among, for example, female sex workers or drug users. Second, we did not distinguish whether participants sought an HIV test or an STI test or whether they visited the site to request PrEP or attend a PrEP information session; these motivations could be differently related to a participant receiving or declining PrEP. Other unrecorded information included reasons for participants declining to participate despite meeting the eligibility criteria (ie, were they not willing to take PrEP or not able to visit the study site again to receive PrEP?), so reasons for not participating remain unclear. Third, we did not include people with an HIV diagnosis in the analysis because most did not fill in the screening tool, so the HIV prevalence among the study sites’ users could not be analyzed.
Conclusions
Screening and enrolling key populations at high risk of HIV in Mexico’s inaugural PrEP service was feasible. Furthermore, participants who were excluded by counselors and who declined PrEP had lower rates of various risk factors than those who received PrEP. Of note, some people who declined PrEP may still be at risk of HIV. Providing PrEP to people with a high risk of HIV is critical to optimizing the public health effects of a PrEP program and to addressing barriers to access PrEP among people with higher levels of vulnerability than the general population.
Further research is needed to validate concise HIV risk assessment tools that can effectively prioritize PrEP for key populations. The screening tool was useful in identifying almost all people at risk of HIV. Still, the additional counseling evaluation helped reduce the tool’s limited capacity for identifying people with low risk of HIV. Programs could implement screening tools in conjunction with counselor assessments to refine eligibility decisions.
Footnotes
Acknowledgements
The ImPrEP Study was implemented in Brazil, Peru, and Mexico with the leadership of Brazil’s principal investigator, Valdiléa G. Veloso, MD, PhD, MSc. We thank staff members at ImPrEP–Mexico’s study sites: CHECCOS, México Vivo, SETAC, and Clínica Condesa. Finally, we thank the participants for providing information to generate scientific evidence.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the United Nations Population Fund and UNITAID (grant MEX07SRH), with additional funding in Mexico by the National Institute of Public Health.