
Abstract
Objective
The opioid epidemic in the United States increasingly affects women of reproductive age and has resulted in a rise in concurrent polydrug use. The objective of this study was to investigate the effect of this polydrug use on preterm birth in a multiethnic birth cohort.
Methods
We analyzed data from 8261 mothers enrolled in the Boston Birth Cohort from 1998 to 2018 in Boston, Massachusetts. We grouped substances used during pregnancy based on their primary effects (stimulant or depressant) and assessed independent and combined associations with smoking on preterm birth.
Results
Of 8261 mothers, 131 used stimulant drugs and 193 used depressant drugs during pregnancy. The preterm birth rate was 27.5% (2271 of 8261) in the sample. Mothers who smoked had 35% increased odds of preterm birth across adjusted models. Mothers who used stimulant drugs without smoking were not at increased risk of preterm delivery compared with mothers who used neither (odds ratio [OR] = 0.69; 95% confidence interval [CI], 0.19-1.98), whereas mothers who used depressant drugs without smoking had more than twice the odds of having preterm delivery (OR = 2.31; 95% CI, 1.19-4.44), and infants were at risk of a 1-week reduction in gestational age (OR = −1.05; 95% CI, −2.07 to −0.03). Concurrently smoking and using depressant drugs was associated with increased odds of preterm birth (OR = 1.83; 95% CI, 1.28-2.61), as was concurrently smoking and using stimulant drugs (OR = 1.73; 95% CI, 1.14-2.59).
Conclusions
Using stimulant drugs and depressant drugs during pregnancy is a risk factor for preterm birth. The individual and combined effects of using these drugs with smoking must be considered together to reduce the risk of preterm birth in the United States.
The opioid epidemic in the United States is increasingly affecting women of reproductive age. 1 Of women aged ≥18 years in the United States, 19.5 million reported using illicit substances in 2016 alone, and the number of women with opioid use disorder who gave birth quadrupled from 1.5 per 1000 deliveries in 1999 to 6.5 per 1000 deliveries in 2014. 2 Stimulant drugs also contribute to the high prevalence of substance use, reported to be 10 times more common than heroin among young adults in 2015. 3 Among women of reproductive age (15-49 years), using both depressant drugs and stimulant drugs during pregnancy is associated with adverse birth outcomes, including prematurity, decreased birth weight and length, and small for gestational age. 4
One such adverse outcome, preterm birth, affects nearly 10% of all US births 5 and cost $26.2 billion in 2005 alone. 6 Preterm birth, defined as gestational age <37 weeks, is a major clinical and public health problem, resulting in many negative sequelae for affected children. 7 Consequences include a higher risk of respiratory disorders such as asthma, 8 cardiometabolic disorders, 9 and reduced cognitive performance, which increases the risk for behavioral disorders by school age. 10 -12
Both stimulant drugs and depressant drugs have been well-described risk factors for preterm birth. 4,13,14 For example, a large meta-analysis showed cocaine (a stimulant) to be associated with a nearly 3-fold unadjusted risk of preterm birth. 13 Although multiple studies on stimulant drugs and preterm birth have controlled for smoking through either multivariate regression or stratified analyses, 15 -20 these studies had small sample sizes, in part because substance users are difficult to reach. 13 Depressant drugs, including opioids, are also associated with preterm birth and are of growing importance given the recent surge of opioid use in the United States. 1 However, several recent studies of this relationship have focused on buprenorphine 21,22 or methadone 23 without accounting for switching between other opioids and medication-assisted therapy. These studies have similarly been limited by small samples 22 or relatively homogeneous samples. 14 Among larger studies, most research on preterm birth used cohorts from the 1980s and the 1990s 13,24,25 and do not reflect substance use trends in the past 20 years. 26 Although polydrug use is the most common type of drug use among pregnant women, 27 few studies have simultaneously examined the role of polydrug use in preterm birth.
Tobacco is the most common concurrent substance among opioid-exposed pregnant women, reported among 88% to 95% of pregnant women who use buprenorphine and methadone. 28 Similarly, 75% of pregnant women who report cocaine use also smoke. 29 The effects of both active and passive smoking on gestation and risk of preterm birth are well-characterized in previous studies, including in multiethnic US cohorts. 30 -33 However, only 1 study controlled for confounding of other drug use during pregnancy. 32 Although this gap in research may be due to low overall prevalence of substance use in a given population, the well-described effect of substance use on birth outcomes 34 is integral to understanding the risk of adverse pregnancy outcomes in today’s substance use crisis.
The objectives of our study were to (1) estimate the separate and combined effects of stimulant drug and depressant drug use in pregnancy on preterm birth and (2) investigate the effect of smoking on these associations.
Methods
Study Population
This study is a secondary analysis of a large birth cohort, using data from 8494 mother–infant pairs recruited in the Boston Birth Cohort at Boston Medical Center from 1998 through 2018 with a final sample size of 8261. We excluded 233 participants because data on the outcome of interest (gestational age) or exposure (smoking or substance use) were missing. Recruitment and data collection methods are described elsewhere. 35 In brief, mothers were recruited 24 to 72 hours after birth. Maternal and newborn clinical information was collected from electronic medical records. Participants completed staff-administered, retrospective questionnaires on sociodemographic characteristics and substance use. Infants resulting from multiple births and with major birth defects were excluded from the parent study.
This research was approved by the institutional review boards of Boston University Medical Center and the Johns Hopkins University Bloomberg School of Public Health. All participants provided written informed consent.
Exposures
Substance use
Questionnaires were administered with a National Institutes of Health Certificate of Confidentiality to increase the validity of responses. Participants reported using any drugs in their lifetime, during the first trimester (1-90 days of pregnancy), during the second trimester (91-180 days of pregnancy), and during the third trimester (181 days of pregnancy to delivery). Substance use during pregnancy was defined as use during any trimester. The substances reported included stimulant drugs (cocaine, crack cocaine, and amphetamines) and depressant drugs (heroin, methadone, and barbiturates). For example, although methadone is prescribed for opioid dependence, evidence suggests that it may elevate the risk of preterm birth 23,36 ; therefore, mothers who were prescribed these substances were included in the sample. Doses for substances were self-reported as regular or occasional use; however, the number of participants was insufficient for more detailed dose analyses.
Smoking
We grouped women into 3 categories of smokers: never smokers, intermittent smokers (women who smoked previously but ceased before the second trimester), and continuous smokers (women who smoked through the second and third trimesters). 37 Smoking late in pregnancy affects preterm birth more than smoking early in pregnancy 38,39 ; women who are pregnant but do not realize it in the first trimester may stop smoking when they learn they are pregnant. As such, tobacco use during pregnancy was defined as smoking continuously into the second and third trimesters.
Outcomes
Gestational age was estimated via early ultrasound and last date of menstrual period as documented in the medical records using established methods 35 ; preterm birth was defined as gestation of <37 weeks at delivery.
Covariates
Sociodemographic factors such as maternal age (in years), education, race/ethnicity, annual household income, marital status, and parity were based on self-report through questionnaires administered in-person. Education categories were completion of elementary school, some secondary school, high school, some college, and college. Body mass index (BMI) was defined continuously as self-reported pre-pregnancy weight (kilograms) divided by height (meters squared). Annual household income was categorized as above or below the sample’s median annual household income. Marital status was a categorical variable for single, currently married, divorced, or widowed. Self-reported race/ethnicity was categorized as non-Hispanic black, non-Hispanic white, Hispanic, and other (Asian, Native American, and multiracial); other responses were grouped because of small sample size. Parity was defined continuously as the number of previous pregnancies. Alcohol use during pregnancy was dichotomized as drinking during any trimester vs no drinking. Variables missing ≥10% of the sample were classified as “missing”; annual household income met this threshold. Multiple imputation with chained equations was conducted for covariates with <10% missingness, using 50 imputations and 30 iterations each. The number of prenatal care visits was included only as a supplementary analysis because of ≥30% missingness, which may have biased the results.
Analysis
The outcomes of interest were preterm birth and gestational age (in weeks). Exploratory analyses included using the Student t test for continuous variables and the Pearson χ2 test for categorical variables and preterm birth, with P < .05 considered significant.
Using regression, we assessed the total effect (direct and indirect) of depressant drugs and stimulant drugs on preterm birth and depressant drugs on gestational age. We used logistic regression to assess the association of substances with preterm birth, and we used linear regression analysis to assess gestational age in weeks as a continuous outcome. We generated 5 types of models for stimulant drugs and depressant drugs. First, we estimated a crude model (model 1). Then, we used a second adjusted model to control for maternal age, education, race/ethnicity, sex of child, annual household income, marital status, parity, BMI, and alcohol use (model 2). We used a third fully adjusted model that included characteristics from the adjusted model and smoking during pregnancy to show independent effects of substances and tobacco (model 3). A fourth model included an interaction term between substances and smoking to discern significant differences between using a single substance and the combined effect of using multiple substances (model 4). The last models examined combined risk categories between drug use and current smoking. These mutually exclusive categories consisted of using neither, smoking only, using stimulant drugs only, and both smoking and using stimulant drugs. We also created similar categories for smoking and depressant drugs.
Supplementary analyses examined the combined use of stimulant drugs and depressant drugs (using neither, using only 1 substance, or using both), controlling for all covariates. We conducted sensitivity analyses with potential confounders, using the number of prenatal care visits, preeclampsia, being obese or overweight, and stratified as delivering before or after 2006. We also generated E values 40 for significant primary findings in order to characterize residual confounding. E values describe the minimum level of association an unmeasured confounder would have to have with both the outcome and exposure to negate an estimated result (controlling for identified covariates). All models used complete-case analysis. We also generated 95% confidence intervals (CIs) and considered P < .05 to be significant. We performed all analyses by using R version 3.5.0. 41
Results
In our sample of 8261 mother–newborn pairs, 131 participating mothers reported using stimulant drugs during pregnancy and 193 participating mothers reported using depressant drugs during pregnancy (Table 1). Of 8261 mothers in the overall sample, 3900 (47.2%) were non-Hispanic black; of 193 mothers who used depressant drugs, 136 (70.5%) were non-Hispanic black. The median annual household income in the overall sample was $35 000.
Demographic characteristics of mothers, by use of stimulant drugs or depressant drugs during pregnancy, Boston Birth Cohort, 1998-2018 a
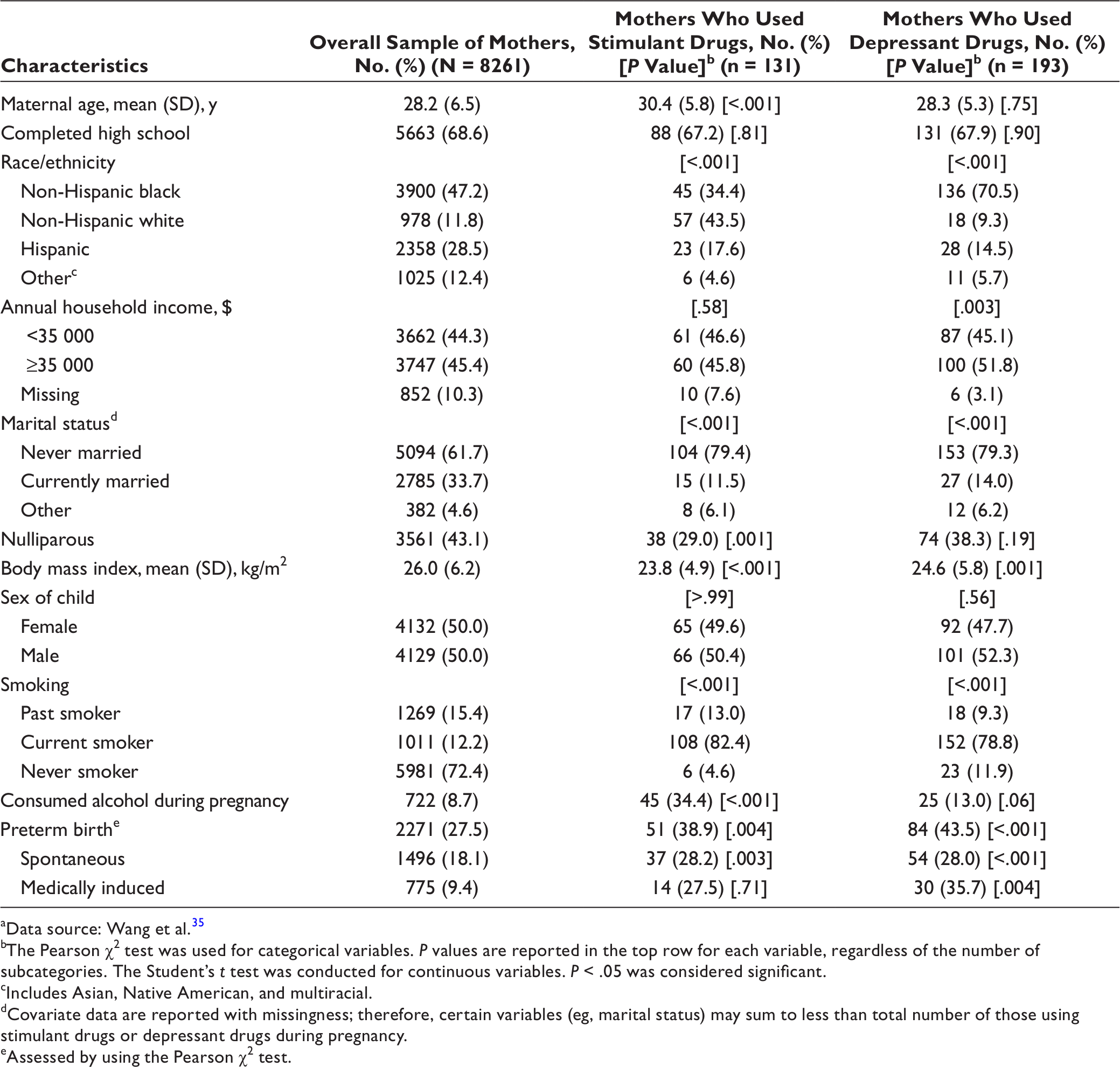
aData source: Wang et al. 35
bThe Pearson χ2 test was used for categorical variables. P values are reported in the top row for each variable, regardless of the number of subcategories. The Student’s t test was conducted for continuous variables. P < .05 was considered significant.
cIncludes Asian, Native American, and multiracial.
dCovariate data are reported with missingness; therefore, certain variables (eg, marital status) may sum to less than total number of those using stimulant drugs or depressant drugs during pregnancy.
eAssessed by using the Pearson χ2 test.
Participants who used stimulant drugs and depressant drugs were significantly more likely than the overall sample to smoke and use alcohol (Table 1). Of 131 participants who used stimulant drugs, 108 (82.4%) were current smokers, whereas among the overall sample, 1011 (12.2%) were current smokers. Alcohol use was also more common among participants who used stimulant drugs (34.4%, n = 45) than among the overall sample (8.7%, n = 722). Cocaine was the most commonly reported stimulant drug, and most stimulant drug-using participants reported occasional use (n = 113, 86.3%). Of women who reported using stimulant drugs, 97.7% (n = 128) reported using cocaine or crack cocaine.
Most participants who used depressant drugs were also current smokers (78.8%, n = 152) (Table 1). Although alcohol use was less common among participants who used depressant drugs (13.0%) than among participants who used stimulant drugs (34.4%), the percentage of women who used alcohol was higher among both groups of women than in the overall sample (8.7%). Most participants who used depressant drugs used methadone (n = 142, 73.6%) or heroin (n = 107, 55.4%), but most participants reported occasional use. The percentage of preterm births was lower in the overall sample (27.5%) than among participants who used stimulant drugs (38.9%) or depressant drugs (43.5%). Most preterm births in the overall sample were spontaneous preterm deliveries (n = 1496) rather than medically induced deliveries (n = 775).
Independent Association of Stimulant Drugs With Preterm Birth and Gestational Age
In bivariate analyses, women who used stimulant drugs during pregnancy had 70% higher odds of preterm birth (95% confidence interval [CI], 1.18-2.41) and 0.78 fewer weeks of gestation (95% CI, −1.33 to −0.23) compared with women who did not use stimulant drugs or tobacco during pregnancy (Table 2). However, after adjusting for smoking, the odds of preterm birth increased by only 19% (95% CI, 0.80-1.75). Current smoking alone was associated with a 35% increase in preterm birth (95% CI, 1.14-1.60) and a half-week reduction (β coefficient = 0.52 weeks; 95% CI, −0.77 to −0.27) in gestation after adjustment in the linear model.
Associations of stimulant drug use in pregnancy with preterm birth and gestational age (in weeks), comparing the unadjusted, semi-adjusted, fully adjusted, and combined risk with smoking models, Boston Birth Cohort, 1998-2018 (N = 8261) a
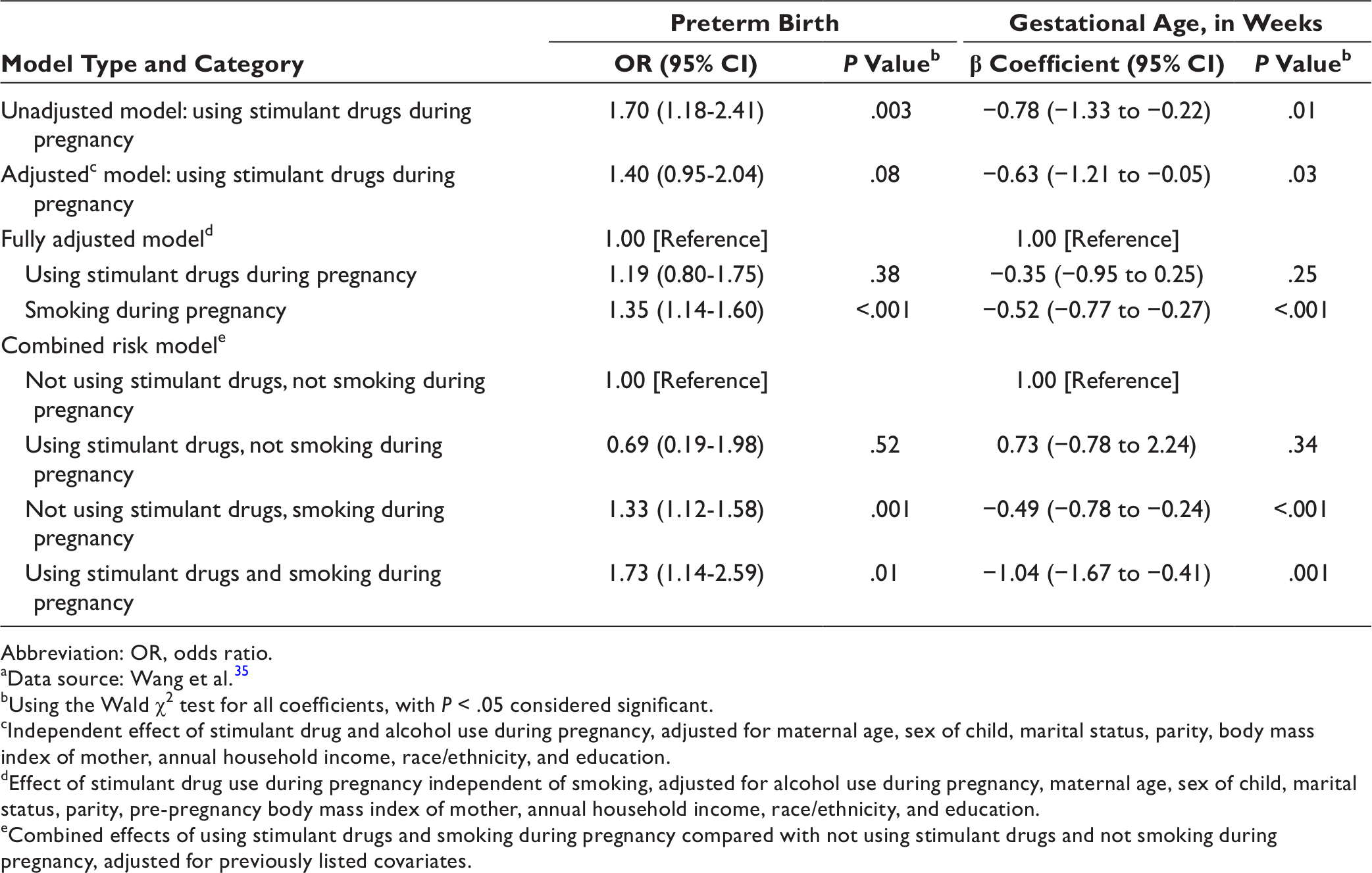
Abbreviation: OR, odds ratio.
aData source: Wang et al. 35
bUsing the Wald χ2 test for all coefficients, with P < .05 considered significant.
cIndependent effect of stimulant drug and alcohol use during pregnancy, adjusted for maternal age, sex of child, marital status, parity, body mass index of mother, annual household income, race/ethnicity, and education.
dEffect of stimulant drug use during pregnancy independent of smoking, adjusted for alcohol use during pregnancy, maternal age, sex of child, marital status, parity, pre-pregnancy body mass index of mother, annual household income, race/ethnicity, and education.
eCombined effects of using stimulant drugs and smoking during pregnancy compared with not using stimulant drugs and not smoking during pregnancy, adjusted for previously listed covariates.
Combined Associations of Stimulant Drugs and Smoking With Preterm Birth and Gestational Age
In modeling the interaction between smoking and stimulant drugs during pregnancy, the interaction term of the 2 was not significant for either preterm birth or gestational age. This association was similar in the model for gestational age; neither stimulant drug alone nor the interaction term was significant.
In the examination of concurrent substance use, 23 mothers used stimulant drugs alone without smoking. Compared with no use of stimulant drugs or smoking, use of stimulant drugs alone was not significantly associated with preterm birth or gestational age (Table 2). Smoking alone during pregnancy was associated with 33% increased odds of preterm birth (95% CI, 1.12-1.58) and a half-week reduction in gestation (β coefficient = −0.49 weeks; 95% CI, −0.78 to −0.24). Among participants who smoked and used stimulant drugs, the odds of preterm birth increased by 73% (95% CI, 1.14-2.59) and gestation decreased by nearly 1 week (β coefficient = −1.04 weeks; 95% CI, −1.67 to −0.41), controlling for all covariates. The sensitivity analyses confirmed these findings with CIs overlapping with those in the primary findings.
Independent Association of Depressant Drugs With Preterm Birth and Gestational Age
Use of depressant drugs was significantly associated with preterm birth and gestational age in the bivariate regression analysis and in the models adjusted for sociodemographic variables (Table 3). In the unadjusted model, this association reflected a 2-fold increase in the odds of preterm birth (OR = 2.07; 95% CI, 1.55-2.76) and a nearly 1-week reduction in gestational age (β coefficient = −0.94 weeks; 95% CI, −1.40 to −0.49). After adjustment, smoking increased the odds of preterm birth by 31% (95% CI, 1.11-1.55) and reduced gestation by half a week (β coefficient = 0.48 weeks; 95% CI, −0.72 to −0.23). Using depressant drugs increased the odds of preterm birth by 54% (95% CI, 1.11-2.12) and reduced gestation by 0.68 weeks (95% CI, −1.17 to −0.18).
Associations of depressant drug use in pregnancy with preterm birth and gestational age (in weeks), comparing the unadjusted, semi-adjusted, fully adjusted, and combined risk with smoking models, Boston Birth Cohort, 1998-2018 (N = 8261) a
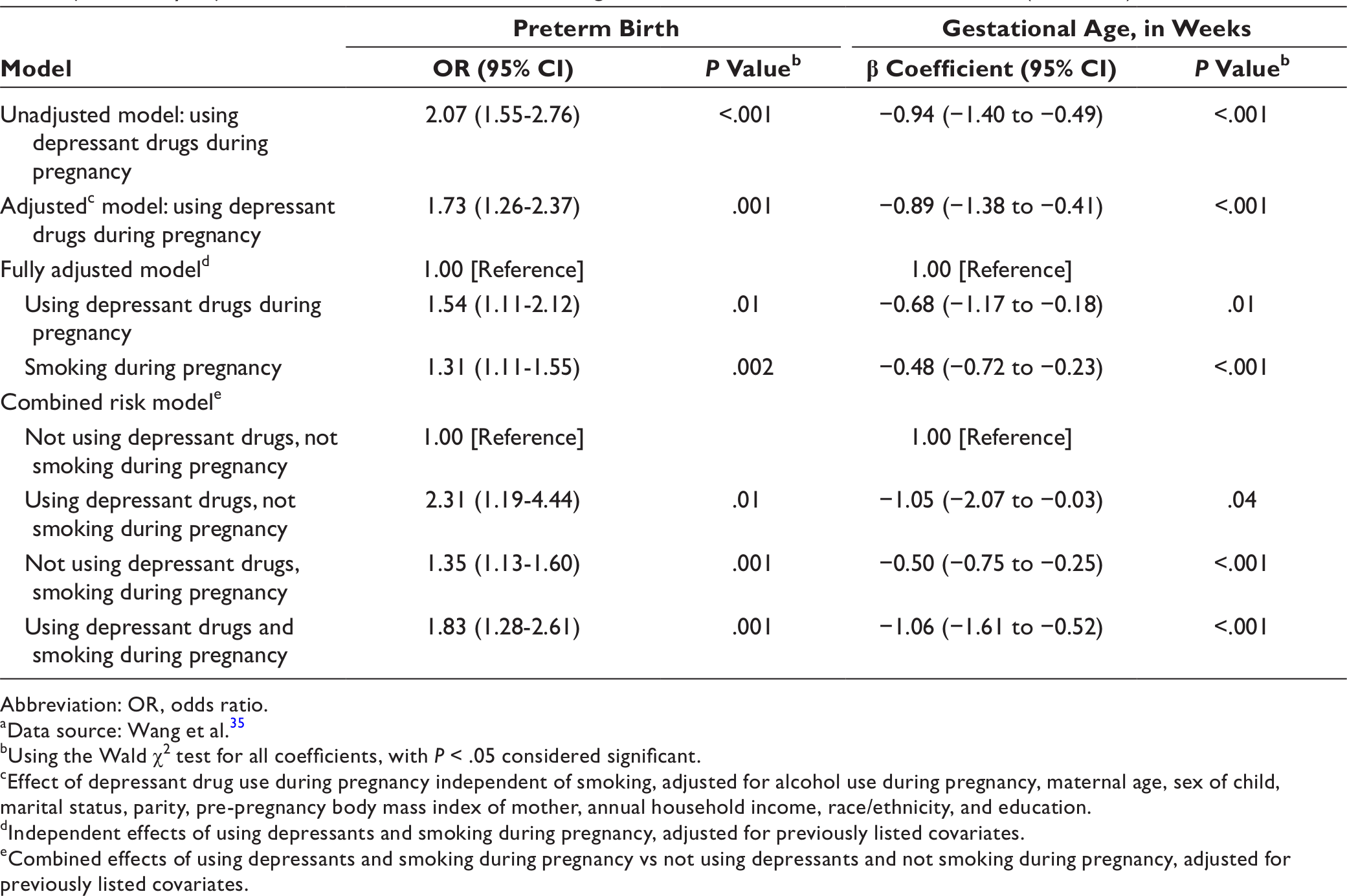
Abbreviation: OR, odds ratio.
aData source: Wang et al. 35
bUsing the Wald χ2 test for all coefficients, with P < .05 considered significant.
cEffect of depressant drug use during pregnancy independent of smoking, adjusted for alcohol use during pregnancy, maternal age, sex of child, marital status, parity, pre-pregnancy body mass index of mother, annual household income, race/ethnicity, and education.
dIndependent effects of using depressants and smoking during pregnancy, adjusted for previously listed covariates.
eCombined effects of using depressants and smoking during pregnancy vs not using depressants and not smoking during pregnancy, adjusted for previously listed covariates.
Combined Associations of Depressant Drugs and Smoking With Preterm Birth and Gestational Age
In the interaction model, using depressant drugs alone during pregnancy was associated with significantly increased odds of preterm birth (OR = 2.31; 95% CI, 1.19-4.44), but the interaction between smoking and using depressant drugs was not significant. Use of depressant drugs alone decreased gestational age by 1.05 weeks (95% CI, −2.07 to −0.03), but the interaction term was not significant (P = .41).
After adjustment, participants who used only depressant drugs during pregnancy (n = 41) had 2.31 times higher odds of preterm birth (95% CI, 1.19-4.44) than participants who used neither depressant drugs nor tobacco (Table 3). Using depressant drugs without smoking corresponded to slightly more than a 1-week reduction in gestational age (95% CI, −2.07 to −0.03). Women who used depressant drugs and smoked had 83% higher odds of preterm birth (95% CI, 1.28-2.61) and a 1.06-week reduction in gestational age (95% CI, −1.61 to −0.52) compared with women who did not use depressant drugs or tobacco during pregnancy. The sensitivity analyses confirmed these results, with CIs that overlapped with those in the primary findings.
Combined Association of Stimulant Drugs and Depressant Drugs With Preterm Birth and Gestational Age
When we examined the use of stimulant drugs and depressant drugs categorically (Table 4), the use of stimulant drugs but not depressant drugs (n = 82) was not significantly associated with risk of preterm birth (95% CI, 0.71-1.91) or gestational age (95% CI, −0.87 to 0.63). However, participants who used only depressant drugs (n = 144) had 60% higher odds of preterm birth (95% CI, 1.11-2.31) and a 0.61-week reduction in gestational age (95% CI, −1.17 to −0.05) compared with women who did not use depressant drugs or stimulant drugs during pregnancy. Compared with women who did not use stimulant drugs or depressant drugs during pregnancy, women who used stimulant drugs and depressant drugs during pregnancy (n = 49) had a non-significant 0.89-week reduction in gestational age (95% CI, −1.81 to 0.04) (P = .06).
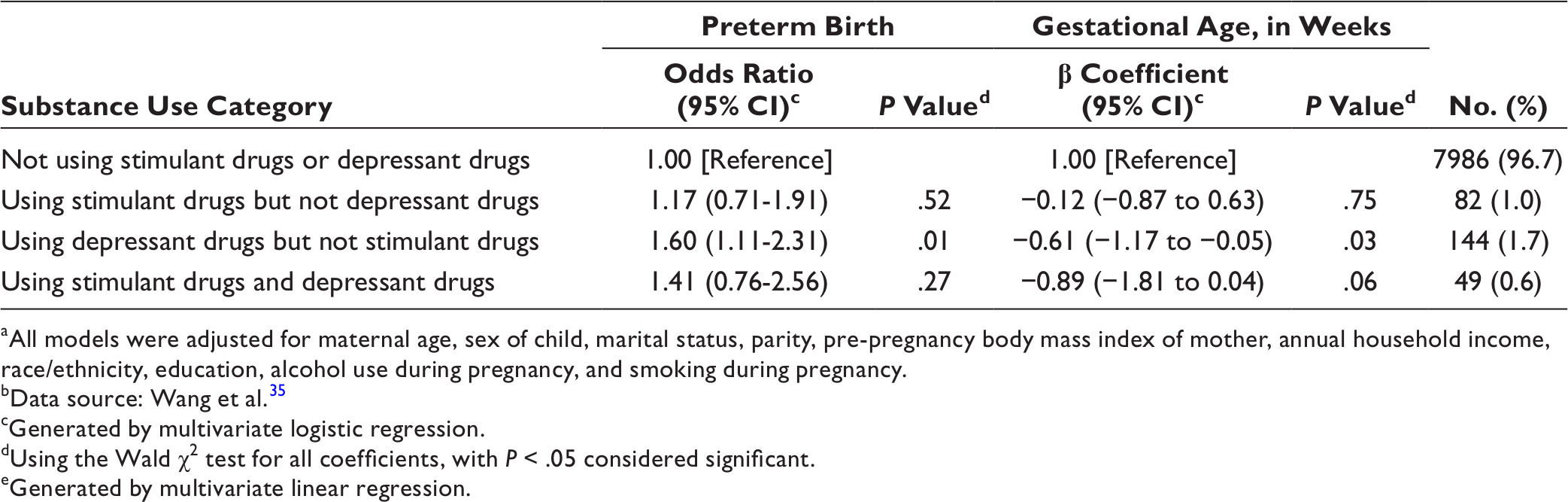
aAll models were adjusted for maternal age, sex of child, marital status, parity, pre-pregnancy body mass index of mother, annual household income, race/ethnicity, education, alcohol use during pregnancy, and smoking during pregnancy.
bData source: Wang et al. 35
cGenerated by multivariate logistic regression.
dUsing the Wald χ2 test for all coefficients, with P < .05 considered significant.
eGenerated by multivariate linear regression.
Discussion
In the midst of an opioid epidemic in the United States, our data and other reports 42 show that using depressant drugs greatly increases the risk of preterm birth, even after controlling for concurrent substance use, including tobacco and stimulant drugs. To our knowledge, our study is the first to simultaneously examine the independent and combined effect of stimulant drugs, depressant drugs, and smoking on preterm birth in a US population at high risk for preterm birth. We found evidence for more than a 2-fold increase in odds of preterm birth among women who used depressant drugs but did not smoke. Furthermore, we found that using depressant drugs alone with no reported smoking reduced gestational age by an estimated 1 week compared with women who did not use depressant drugs or smoke during pregnancy. However, stimulant drugs did not show consistent significant associations with preterm birth, either as a predictor alone or after controlling for smoking, although evidence suggests that using stimulant drugs and tobacco together during pregnancy increased the odds of having a preterm birth more than using tobacco alone.
Smoking, which is prevalent among substance users, is a major effect modifier for any individual drug effect. Our findings demonstrated that use of depressant drugs during pregnancy was independently associated with an elevated risk of preterm birth, even when we restricted the analysis to nonsmokers. Our estimates, which suggest approximately double the risk of preterm birth, are similar in magnitude to previously reported estimates for preterm birth among offspring of women who used methadone or buprenorphine during pregnancy. 14,43 However, unlike our study, those studies did not attempt to directly compare the independent and joint effects of depressant drugs and tobacco.
When women reported using depressant drugs and smoking, we found a reduced effect in the point estimates for preterm birth and gestational age compared with using depressant drugs alone, although the CIs overlapped. This finding was counter to our expectations given that depressant drugs alone and smoking alone have been related to preterm birth in previous research. 23,33 Nonetheless, a similar pattern of reduced risk was reported in at least 1 other study. 14 Our data showed that the magnitude of association between use of depressant drugs alone and preterm birth (odds ratio = 2.3) was stronger than the association between smoking alone and preterm birth (odds ratio = 1.4).
One reason for lower odds of preterm birth among dual users may be a lower frequency of depressant drug use during pregnancy. In other words, women who smoke and use depressant drugs may reduce their depressant drug use during pregnancy but continue to smoke. In a qualitative study of experiences of using methadone during pregnancy, women described difficulties in taking the drug because of nausea/vomiting and a lack of support services. 44 Other qualitative work found that women from a similar largely low-income, multiethnic population rationalized moderate levels of smoking during pregnancy. 45 Furthermore, research has shown that persons were often skeptical of the need to refrain from smoking and the full extent of the risks. 45 These studies support the idea that pregnant women may be more likely to discontinue using depressant drugs than to discontinue smoking. Women with dual dependencies may be overwhelmed by reducing both dependencies at once and choose to address what they perceive to be the riskier exposure first; in this case, depressant drugs.
In our results, smoking alone, compared with not smoking, consistently increased the odds of preterm birth by about 34%. This finding is consistent with the findings of a systematic review estimating that smoking was associated with 1.27 higher odds of preterm birth across 20 studies. 32 In addition, our estimated effect of using stimulant drugs and smoking showed reductions in gestational age similar to the meta-analytic estimate for using cocaine with overlapping CIs. Other drugs in the stimulant drug group, such as methamphetamines, have been associated with a similar gestational age reduction of 1 week. 46 These replicated findings add validity to our results.
Limitations
Our study had several limitations. First, although our study is one of the largest studies of maternal polydrug use and preterm birth, the sample contained a small number of substance users, and subgrouping by dose or drugs reduced the power to detect group differences. For example, our findings for using only stimulant drugs were inconsistent, even though cocaine use is a well-known risk factor for preterm birth. Similarly, CIs between the depressant drug and smoking estimated effects overlapped; as such, although there were clear independent effects of each substance compared with not using these substances during pregnancy, our study lacked the power to determine whether the difference between their independent and joint effects was notable. One potential explanation for this finding may be the small number of women who used substances and did not smoke. Second, substance use was based on self-report rather than toxicological testing, which may have led to misclassification of cases. Although our study obtained a National Institutes of Health Certificate of Confidentiality to increase the likelihood of accurate reporting, it is likely that misclassification remained, leading to underreporting of drug use because of social desirability. A recent small study found that opioid use was more accurately reported than other substance use during pregnancy, but the sensitivity of the study was limited. 47 Similarly, residual confounding may have been a factor in our study, although our sensitivity analyses largely supported our primary findings among measured confounders. Supplementary E values also suggested that a residual confounder would need an effect size of at least 2-fold with both the exposure and outcome to remove the relationship between these combined stimulant drugs and smoking or depressant drugs and smoking categories in our primary analysis. Unmeasured factors, such as maternal infections, housing stability, and other barriers to care that may be associated with substance use during pregnancy, may still affect this relationship. Future studies should address these areas. Finally, grouping substances into stimulant drugs and depressant drugs did not allow for generating substance-specific estimates. However, this grouping was necessary to maintain sufficient power while stratifying in analyses and may reflect data on women who change substances, such as women entering methadone maintenance after using heroin.
Conclusion
Rich data from the Boston Birth Cohort offers the opportunity to study combined drug effects with tobacco on preterm birth in a large, multiethnic, urban, low-income population in Boston. We showed an independent effect of using depressant drugs on preterm birth; the magnitude of this effect was greater than the effect of smoking. Our study highlights the importance of smoking as an effect modifier between other substances and preterm birth, given high rates (about 80%) of concurrent use. Future studies are needed to understand the effects of dose and timing on these risks and the effects on other important birth outcomes, such as size for gestational age and pregnancy complications. Given the rising rates of opioid overdose in the United States 1 and the continued use of cocaine, these findings are important for informing health care provider and patient decisions during pregnancy. Opioid use must be considered in the landscape of broader polydrug use, and attention must be paid to mothers because substance use fuels a harmful intergenerational cycle, with adverse effects on these women and future generations.
Footnotes
Authors’ Note
The following materials are available upon request from the corresponding author: a flowchart of inclusion criteria from initial cohort to analytic study sample, data on self-reported dose of substances used during pregnancy and missingness in sociodemographic covariates, and sensitivity analyses of (1) associations between using stimulant drugs and depressant drugs after adjusting for perinatal care visits, (2) associations between using stimulant drugs and depressant drugs when including body mass index categories, (3) associations between using stimulant drugs and depressant drugs when including preeclampsia categories and intrauterine growth restriction, and (4) primary depressant drug analysis stratified by giving birth before or after the mean year of the sample.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Boston Birth Cohort (the parent study) is supported in part by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under grant number R40MC27443 and cooperative agreement UJ2MC31074; by the March of Dimes Foundation (20-FY02-56 and 21-FY07-605) and by the National Institutes of Health (NIH) under grants number R01HD086013, 2R01HD041702, R21ES011666, R21HD066471, R21HD085556, and R01 HD098232. This information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, NIH, HHS, or the US government.