
Abstract

This supplement on HIV, hepatitis, sexually transmitted disease, and tuberculosis is timely and important because it highlights the many ways that law, regulation, and institutional policy affect the incidence and prevalence of infectious disease. Law is a causal factor that deserves careful scientific research attention, not only because it is central to understanding disease variation across time and space, but also because law is, importantly, a malleable cause. “Law” has many meanings, but for purposes of this article is defined as a set of rules developed and enforced by government. In a democracy, we collectively create the law and, in so doing, we create the conditions that affect public health, including fostering or impeding the spread of infectious disease. In this commentary, we briefly review the notable ties between law and public health and then present a version of our previously proposed causal framework of law’s impact on population health, now adapted to infectious disease. We then discuss current research in law and infectious disease in light of the causal framework and describe areas for future consideration.
Law and Public Health
Law deeply affects health, quality of life, and happiness—spanning every public health issue of concern. Some examples of how law affects public health in ways that prevent millions of deaths and untold human suffering are straightforward and easy to understand, because they operate through straightforward mechanisms, with only a few links in the mediating causal chain. Clean air to breathe and clean water to drink are essential for health, and a panoply of laws and regulations is necessary to ensure their continued availability. 1 Auto airbags reduce the probability of fatality by 30%. 2 Laws requiring the installation of auto airbags in new cars thus quickly began reducing morbidity and mortality, leading to more than 40 000 lives saved by 2012. 3 Among the many closely related examples of auto safety laws are vehicle crash standards, roll-over standards, and mandatory rear camera installation. 4
Other product safety standards have also had important effects, such as laws requiring childproof caps on medicine bottles, which reduce the incidence of childhood poisoning ingestions by 50%. 5 Safety standards may also have less clear health implications, such as the case of HIV preexposure prophylaxis (PrEP). PrEP is the provision of antiviral medication to uninfected persons, a highly efficacious strategy that reduces HIV transmission by more than 99% among men who have sex with men (MSM) when taken daily. 6 PrEP clinical practice guidelines provide guidance for clinicians 7 but result in a high clinical burden (ie, 4 clinic visits per year for laboratory testing and behavioral assessment) that may contribute to lower PrEP use. 8 -10 Moreover, one of our studies found that the guidelines perform little better than chance at predicting new HIV infections among African American MSM. 11 The poor performance of the screening tool could not only lead clinicians to exclude at-risk persons from PrEP but also contribute to increased black–white disparities in the HIV epidemic.
Laws that increase taxes on hazardous products such as tobacco and alcohol, and laws that reduce access to such products, substantially reduce their consumption and lead to concomitant reductions in acute and chronic health problems associated with their use. 12 -15 Even the spread of infectious diseases, such as sexually transmitted diseases, might be reduced by increasing the tax on alcoholic beverages. 16 Although these examples are conceptually easy to understand, they are examples of legal effects that required extensive research, science, and engineering advancements coupled with years of advocacy, legislation, and litigation to achieve their potential for improved public health.
After basic research reveals important causal factors, followed by the design and engineering of interventions and technologies to ameliorate or attenuate those causal effects, the role of law often moves to the forefront in encouraging, facilitating, or requiring adoption. PrEP is an excellent example of this phenomenon: basic research produced the necessary active pharmaceutical ingredients, 17 international human trials determined intervention efficacy, 18 analyses of blood assays determined efficacy among adherent persons, 7 clinical practice and demonstration projects determined feasibility of scale-up, 19,20 and laws and policies to enhance scale-up were lobbied for and implemented in numerous jurisdictions. 9,21
Law also shapes the missions, structures, and function of major systems in society. Such effects of law on population health are often overlooked but are easy to recognize by those working in or with a deep understanding of a given system. Most obviously, law determines the powers, duties, and restraints of public health agencies—the classic field of public health law. 22 Law creates the overall health care system, determines standards of care, structures financing and delivery, shapes who does and does not receive care, and influences which procedures and treatments are widely disseminated and which are not. 23 For example, the positive effects of the Ryan White HIV/AIDS and President’s Emergency Plan for AIDS Relief programs are well documented. 24 -26 Yet similar programs are lacking for hepatitis C treatment and for new biomedical prevention mechanisms such as PrEP.
Law similarly affects other major systems in society. The social welfare system profoundly affects population health and wellbeing, particularly for persons in the bottom quarter of socioeconomic hierarchies. Rules for foster care, mental health commitments, the degree to which persons who are disabled are provided a livable level of support without stigma, and many other dimensions are based in law. 27 Federal, state, and local law that structures the education system deeply affects who benefits from this core foundation for a healthy and meaningful life. 28,29 Laws and legal standards reflected in building codes, land-use law, and zoning rules profoundly influence health risks and health protections embedded in the homes, workplaces, neighborhoods, and cities in which people live. 30 These standards and rules affect a host of health risks that affect infectious disease transmission and susceptibility, from toxic environmental exposures to social connectedness and friendship/support networks.
Law creates other social subsystems with substantial consequences for public health. Consider contract law, tort law, and the civil liability statutes and case law that underlie most business operations. As one example, noncompete agreements (mandating that an employee not compete with an employer for a specified period after leaving employment) have recently spread widely. Noncompete agreements were originally used for a small number of top executives and high-status employees but are now being applied to many regular employees, including those working minimum-wage service jobs. The result is a less competitive labor market, increased stress, and reduced job opportunities and income among low- and moderate-income workers, with implications for the health of their families. Criminal law, seemingly unrelated to infectious disease, can facilitate onward transmission of damaging stigma that may impact the mental health of persons living with HIV. 31 As we move through the major social systems that are affected by law, the causal complexity increases, and many potential health effects are often largely hidden from view of policy makers, scientists, and the citizenry at large.
The public health field is increasingly returning to a traditional focus on the role of a diverse set of complex social systems in population health, after many decades of higher attention to biological mechanisms of disease. Under the rubric of the social determinants of health, the centrality of law in shaping social systems is increasingly coming to the fore.
Causal Framework for the Impact of Law on Infectious Disease
We propose a framework that places law as a causal factor influencing infectious disease outcomes (Figure), adapting a model we previously developed for general population health. 32 Laws can be used as a public health tool for intentional protection or prevention. Laws with no manifest focus on health can also have unintentional beneficial or harmful effects on health outcomes. Public health has traditionally used law as a tool for direct control of infectious disease. In the last decade, attention has been paid to the concept of Health in All Policies to understand the health implications of all laws, including laws that influence social determinants. 33 Law has a central role in altering economic, social, and health care conditions in ways that influence opportunity, exposures to risks and protections, psychosocial factors, and health behaviors. We highlight some components of the framework as it is adapted to infectious disease.
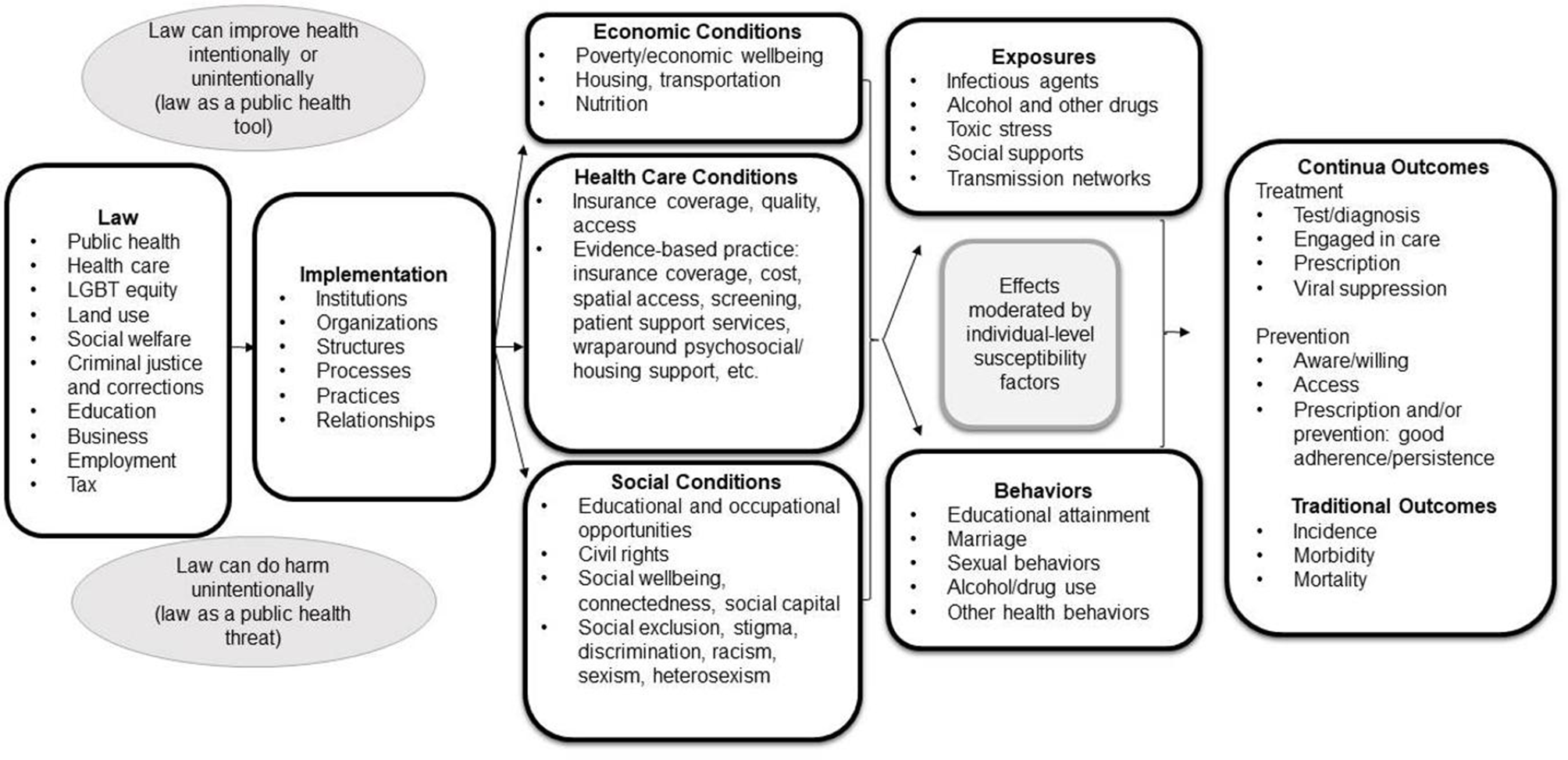
Causal framework of the impact of law on prevention and treatment continua for infectious diseases. Arrows represent the causal pathway from law to health outcomes, through living conditions that influence exposures and behaviors and, ultimately, health outcomes. The pathway may be moderated by individual-level susceptibility factors. Ovals clarify that a law may have a net positive or net negative effect. Adapted from Komro et al. 31 Abbreviation: LGBT, lesbian, gay, bisexual, transsexual.
Health care system conditions can be an intermediate determinant between law and infectious disease outcomes. Health care access, in particular health insurance coverage and its quality, is a key structural determinant. For example, a national study showed that coverage for more than one-third of prescriptions for direct-acting antiviral (DAA) therapies to treat hepatitis C virus infection were denied, and commercial health insurance was more likely to deny coverage (52%) than Medicaid (35%) or Medicare (15%). 34 DAA medications have high rates of cure, leading to important outcomes for patients and for onward disease transmission. Differential health insurance coverage levels by government payers illustrate the heavy influence of law and the organizations implementing it. Similarly, some states have implemented patient assistance programs to cover the costs of PrEP care, whereas other states have no support for PrEP use or its expansion. 35 Policy supports for PrEP are a key consideration because PrEP scale-up is directly tied to substantial declines in new HIV diagnoses at the population level. 36
The body of evidence-based practice for clinical prevention and treatment for infectious diseases is growing, with several literature reviews detailing effective interventions. 37 -39 Laws influence provision of these interventions. For example, funds from the Ryan White HIV/AIDS Program have been used to provide the evidence-based linkage case management intervention, which provides brief and intensive service to facilitate patient linkage to treatment. 40,41 Other efficacious support services funded by the Ryan White HIV/AIDS Program, such as wraparound service provision, are associated with numerous metrics of improved care. 24 Yet allocation of Ryan White program funds has been predominantly based on initial allocations rather than on current distribution equity standards such as HIV incidence or poverty rates among those receiving services, 25 impacting the ability for these services to be offered in jurisdictions with the greatest need. For commercially insured patients, distal legal requirements such as regulations in the Patient Protection and Affordable Care Act likely influence payer willingness to cover these types of evidence-based services.
To facilitate consideration of the effects of policies such as the Ryan White HIV/AIDS Program and the Affordable Care Act on outcomes, we have added treatment and prevention continua metrics as outcomes in the causal framework for infectious diseases, supplementing more traditional metrics of disease burden and mortality. Treatment and prevention continua/cascades serve as important conceptual models for advancing infectious disease control. Systematic reviews of care cascade outcomes for HIV treatment, 42 PrEP, 43 hepatitis C treatment, 44 and tuberculosis care 45 reveal comparative health care system performance and identify opportunities for progress. Continua metrics are also a powerful force for organizing responses to epidemics, such as the UNAIDS 90-90-90 targets: 90% of persons with HIV will be diagnosed, 90% of HIV-positive persons will access treatment, and 90% of HIV-positive persons on treatment will be virally suppressed by 2020. 42 Each component of the HIV and hepatitis care cascades has evidence-based interventions that improve outcomes, 46,47 yet understanding legal influences on implementation of such programs deserves additional research. One quasi-experimental study found that both general medical care and mental health care visits and costs were reduced among MSM after same-sex marriage was legalized in Massachusetts. 48 Similar quasi-experimental studies are needed to identify legal determinants of outcomes along treatment and prevention continua.
Evidencing on Law as a Determinant of Health
In our own research, causal frameworks structured a series of quasi-experiments examining the health effects of state laws that influence upstream social determinants of health. One of the Healthy People 2020 goals is to address the broad social determinants of health to achieve health equity and eliminate health disparities. 49 In a series of quasi-experiments, we are studying the health effects of state-by-state variations and, importantly, changes over time in tax credits for working families (eg, Earned Income Tax Credit [EITC]) and minimum wage standards. Research on the effects of major changes to the federal EITC shows that this tax policy reduces the number of persons living in poverty, increases labor force participation (particularly among single mothers), improves mental health and self-reported health among mothers, and increases birth weight among newborns. 50 -53 We also found that positive EITC effects were more pronounced for black mothers, indicating that the EITC may be an appropriate policy to address health disparities. 53
Similarly, state minimum wage laws may influence infectious disease outcomes, such as new HIV diagnoses. Black men and women bear a disparate risk of contracting HIV, 54 and poverty is a well-established risk factor for incident HIV infection. 55 -57 Therefore, we examined the ecological relationship between state minimum wage laws and rates of new HIV diagnoses among heterosexual black residents of US metropolitan statistical areas (MSAs) from 2008 through 2015. 58 We estimated that MSAs with a minimum wage that was $1 higher at baseline in 2007 had a 27% lower rate of subsequent newly diagnosed HIV cases in 2008. Exploratory analyses suggest that income inequality may mediate this relationship. Research has found that income inequality is among the strongest social predictors of HIV incidence and prevalence in the United States, and higher inequality may lead to decreased social cohesion, increased crime rates, and lower marriage rates, all of which are associated with HIV infection. 55 These findings point toward the importance of addressing income inequality with policy strategies.
One of our recent assessments of PrEP use in the United States examined proximal legal influences, specifically the influence of state Medicaid expansion status on health outcomes. 59 Our study found that states that adopted Medicaid expansion had higher rates of PrEP users than states that did not adopt Medicaid expansion, both per population (30 vs 19 per 100 000 population) and per new HIV diagnosis (2.4 vs 1.1 PrEP users per new diagnosis). Other studies have found that persons with health insurance are more likely to use PrEP and to remain on PrEP than their uninsured counterparts, 10,60 and Medicaid expansion has the potential to facilitate access to health insurance. The association we found between Medicaid expansion and PrEP use is cross-sectional; further quasi-experimental evaluations that combine legal data sets on variation in Medicaid expansion with longitudinal PrEP use data are needed to better assess whether the relationship is causal. We anticipate that the proposed causal framework for infectious diseases will provide utility for this and other assessments by informing identification of mediators and outcomes and by providing a model to structure analyses.
Conclusion
Controlled time-series policy evaluation studies on the health effects of distal causes (eg, minimum wage, EITC) and proximal causes (eg, Medicaid expansion) will play an increasingly important role in public debate on optimal strategies for addressing upstream legal determinants of population health and health equity. Such rigorous research is only possible by linking reliable and valid data on the independent variables of interest (ie, multiple dimensions of policy innovations and their implementation timing) with the key dependent variables (ie, health and wellbeing outcomes). To evaluate the broad scope of policy interventions that could affect population health, researchers must determine relevant measures not only of primary health outcomes, but also of mediators in the hypothesized causal links, including exposures to economic and social risks and protections, as well as relevant intervening behaviors. Frequently measured longitudinal data at varying levels of aggregation (for both the policy-independent variables and the mediating and health outcome measures) allow for time-series research designs that incorporate multiple elements that strengthen causal inference. 32,61 Ongoing surveillance and documentation of policy, including changes over time and geographic location, is a critical first step in facilitating rigorous science in public health law research. In the absence of such data systems, opportunities will be missed. For example, national surveillance systems are lacking for PrEP use and hepatitis care, challenging the use of quasi-experimental designs in these areas. Designing and implementing ongoing data collection efforts for these areas will facilitate not only monitoring, but also the evaluation of changes in laws, regulations, and implementation procedures.
Law is an important but often understudied force in shaping the social and economic environments in which people live. Historically, many public health accomplishments were achieved by using laws and regulations to help shape the physical and social environments. Because law shapes so many dimensions of society, and because so many dimensions of the economic and social environment affect one’s odds of optimal health, opportunities abound for research on how law shapes health. This supplement illustrates such opportunities and induces a broad set of legal researchers, epidemiologists, social scientists, economists, and biostatisticians to move the scientific base forward. Law is a key malleable cause for population health—one that already has improved health so much, but a malleable cause whose potential has only begun to be tapped to optimize health, wellbeing, and happiness.
Footnotes
Declaration of Conflicting Interests
The authors disclosed the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AJS is an investigator on a grant funded by Gilead Foundation, paid to his institution.
Funding
The authors disclosed the following financial support with respect to the research, authorship, and/or publication of this article: This research was supported in part by R01MD010241 from the National Institute on Minority Health and Health Disparities, National Institutes of Health (NIH) (Komro, Wagenaar), and by the National Institute of Mental Health (R01MH114692) and the Adolescent Medicine Trials Network for HIV/AIDS Interventions (Protocol 159) from NIH (U19HD089881). The work was facilitated by the Emory Center for AIDS Research (P30AI050409).