
Abstract
Objective:
A disproportionate number of tuberculosis cases and tuberculosis deaths occur among persons experiencing homelessness in the United States. Our objective was to identify risks for homelessness and death during mycobacterial treatment among persons experiencing homelessness with tuberculosis in Texas.
Methods:
Using data from the Centers for Disease Control and Prevention’s TB Genotyping Information Management System, we evaluated data on demographic, laboratory, and clinical characteristics of persons experiencing homelessness in Texas during the year before tuberculosis diagnosis, from January 1, 2010, through December 31, 2017.
Results:
Of 10 130 new diagnoses of tuberculosis among persons living in Texas during the study period, 543 were reported as being homeless in the year before tuberculosis diagnosis. The odds of dying during treatment were 2.26 (95% confidence interval, 1.68-3.03) times higher among persons with tuberculosis experiencing homelessness than among persons with tuberculosis living in homes.
Conclusions:
Our findings indicate that persons experiencing homelessness bear an undue burden of tuberculosis mortality in Texas. The burden may be related to poorer health caused by poverty stressors, comorbidities, or lack of access to health care.
Keywords
Tuberculosis (TB) is the leading cause of death by a single infectious agent, causing an estimated 1.3 million deaths worldwide in 2017. 1 The United States has a low incidence of TB: the incidence of TB was 2.8 cases per 100 000 persons in 2018, a 1.3% decrease from 2017. 2 Despite the recent overall decrease in the number of newly diagnosed TB cases in the United States (from 9547 cases in 2015 to 9029 cases in 2018), the current strategies used by TB control and elimination programs are not adequate to reach the TB elimination goal in the United States by 2035. 3 California, Florida, New York, and Texas account for half of the TB cases in the United States. The annual TB incidence among persons experiencing homelessness (PEH) in the United States ranged from 36 cases per 100 000 population in 2006 to 47 cases per 100 000 population in 2010, indicating that PEH shoulder a disproportionate burden of TB. 4 In 2017, the percentage of PEH with TB in Texas was lower than the percentage of PEH with TB nationally (4.0% vs 4.6%). 5 However, a population-based study that analyzed urban homelessness in persons with TB during 1995-2004 in Houston, the largest city in Texas, found a higher rate of TB among PEH (411 cases per 100 000 population) than among persons living in homes (9.5 cases per 100 000 population), indicating that PEH is a population at high risk that needs to be evaluated so that effective strategies for TB control and prevention can be developed. 6
The objective of our study was to determine trends and risk factors associated with morbidity and mortality among PEH with TB in Texas by using statewide surveillance data. With the changing demographic characteristics, diagnostic capabilities, and treatments available to public health entities and clinicians, a current picture of the TB burden, including homeless status, is needed to determine how resources are allocated and used in preventing and controlling TB in a state such as Texas, which, in a nation with a low prevalence of TB, has an incidence of TB that is higher than the national average.
Methods
We used retrospective de-identified surveillance data of all confirmed TB patients in Texas reported to the National TB Surveillance System during the 8-year period from January 1, 2010, through December 31, 2017. We downloaded these data from the Centers for Disease Control and Prevention’s TB Genotyping Information Management System, which includes genotyping information from Mycobacterium tuberculosis (MTB) isolates of persons with active TB disease (hereinafter, TB). 7 This study was approved by the Houston Methodist Hospital’s institutional review board.
We extracted data on the following demographic characteristics: age at diagnosis (categorized in groups as 0-4, 5-14, 15-24, 25-44, 45-64, ≥65 years), sex at birth (male, female), and self-reported race/ethnicity (non-Hispanic Asian, non-Hispanic African American, Hispanic, non-Hispanic white, and other). We examined the following, which are known to be risk factors for TB: nativity (born in United States vs non–US-born), living in an urban county or a rural county, excessive alcohol use within the past year, injection drug use within the past year, inmate at a correctional facility at the time of diagnosis, and living in a long-term care facility at the time of diagnosis. Clinical factors included contact with an infectious TB patient within the past 2 years, previous latent TB infection, previous TB, end-stage renal disease or chronic failure at time of diagnosis, organ transplant, tumor necrosis factor–α, status at diagnosis (alive or dead), HIV status at time of TB diagnosis, diabetes status previously or at time of TB diagnosis, immunosuppression, general site of infection, and specific site of infection. Laboratory factors included positive sputum smear, results of sputum culture, how diagnosis was verified, results of chest radiography, multidrug resistance, drug resistance, treatment outcome, and genotyping (whether genotyped, GENTypes, and lineage of genotype).
TB genotyping of isolates from persons with TB involves 2 separate techniques: 1 technique uses 12 mycobacterial interspersed repetitive units (MIRUs), and the other (MIRU2) uses 24 MIRUs combined with spacer oligonucleotide typing (spoligotyping). Each unique combination of spoligotype and MIRU is called a PCRType, and each unique PCRType and MIRU2 is called a GENType. Clusters are isolates found in the same public health jurisdiction with the same GENTypes within a specified 3-year period. TB cases within a cluster are potentially part of the same transmission chain. Each MTB isolate can be categorized into 1 of 6 major global genetic groups, or lineages, on the basis of large sequence polymorphisms.
We described and analyzed the frequency of demographic, clinical, and laboratory characteristics of persons with TB and their MTB isolates by using Pearson χ2 and Fisher exact tests. We defined homelessness as being without a fixed, regular, and adequate night-time residence or a primary night-time residence that was a supervised publicly or privately operated shelter, an institution that provided a temporary residence, or a public or private building not designated for, or ordinarily used as, a regular sleeping accommodation for human beings; or having no home or was alternating between multiple residences at any time during the 12 months before initiation of the TB diagnostic evaluation. 8 We excluded from analysis 5 persons with TB whose information on homeless status was missing or unknown. We used the Wilcoxon-type nonparametric trend test to evaluate the overall trend of the proportion of PEH over time. We used multiple logistic regression modeling to analyze and evaluate risk factors associated with PEH and risk factors associated with death during treatment among PEH with TB. We excluded 9 PEH with TB who were dead at the time of TB diagnosis from the analysis of risk factors for death among PEH with TB who died during treatment compared with PEH with TB who completed treatment. We included in our analyses persons who died after TB diagnosis and had at least 1 treatment (n = 553) and persons who completed therapy (n = 7333). We created maps by using Stata version 15.1 spmap functions, 9 and we conducted all analyses by using SAS version 9.4. 10 We considered P < .05 to be significant.
Results
We identified 10 125 persons with TB in Texas whose homeless status was known during the study period; of these, 543 (5.4%) persons with TB were experiencing homelessness in the 12 months before initiation of the TB diagnostic evaluation (Table 1). The annual proportion of PEH with TB ranged from 3.6% to 6.9% of all TB cases in Texas; we found no significant trend in the proportion over time (z = −0.65; P = .52) (Figure 1).
Demographic, clinical, and laboratory factors associated with persons with tuberculosis in Texas, stratified by homeless status, 2000-2017a
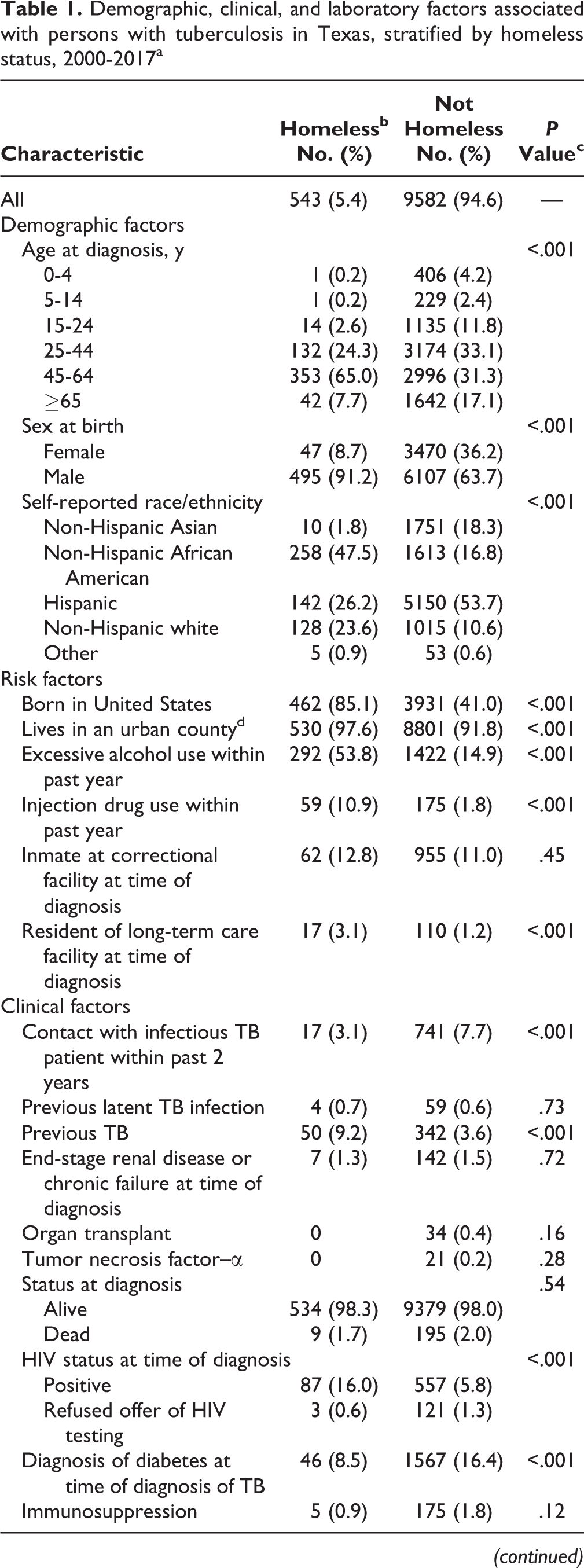
Abbreviations: AFB, acid-fast bacilli; TB, tuberculosis.
a Data source: Centers for Disease Control and Prevention. 8
b Defined as being without a fixed, regular, and adequate night-time residence or a primary night-time residence that was a supervised publicly or privately operated shelter, an institution that provided a temporary residence, or a public or private building not designated for, or ordinarily used as, a regular sleeping accommodation for human beings; or having no home or was alternating between multiple residences at any time during the 12 months before initiation of the TB diagnostic evaluation. 8
c Generated by using Pearson and Fisher exact tests. P < .05 was considered significant.
d Defined as a county with an estimated population of ≥50 000 persons in 2017.
e Resistant to treatment with ≥2 of the most powerful first-line anti-TB medications (drugs), isoniazid and rifampin.
f Patient had an initial positive sputum culture that converted to a documented negative culture during treatment.
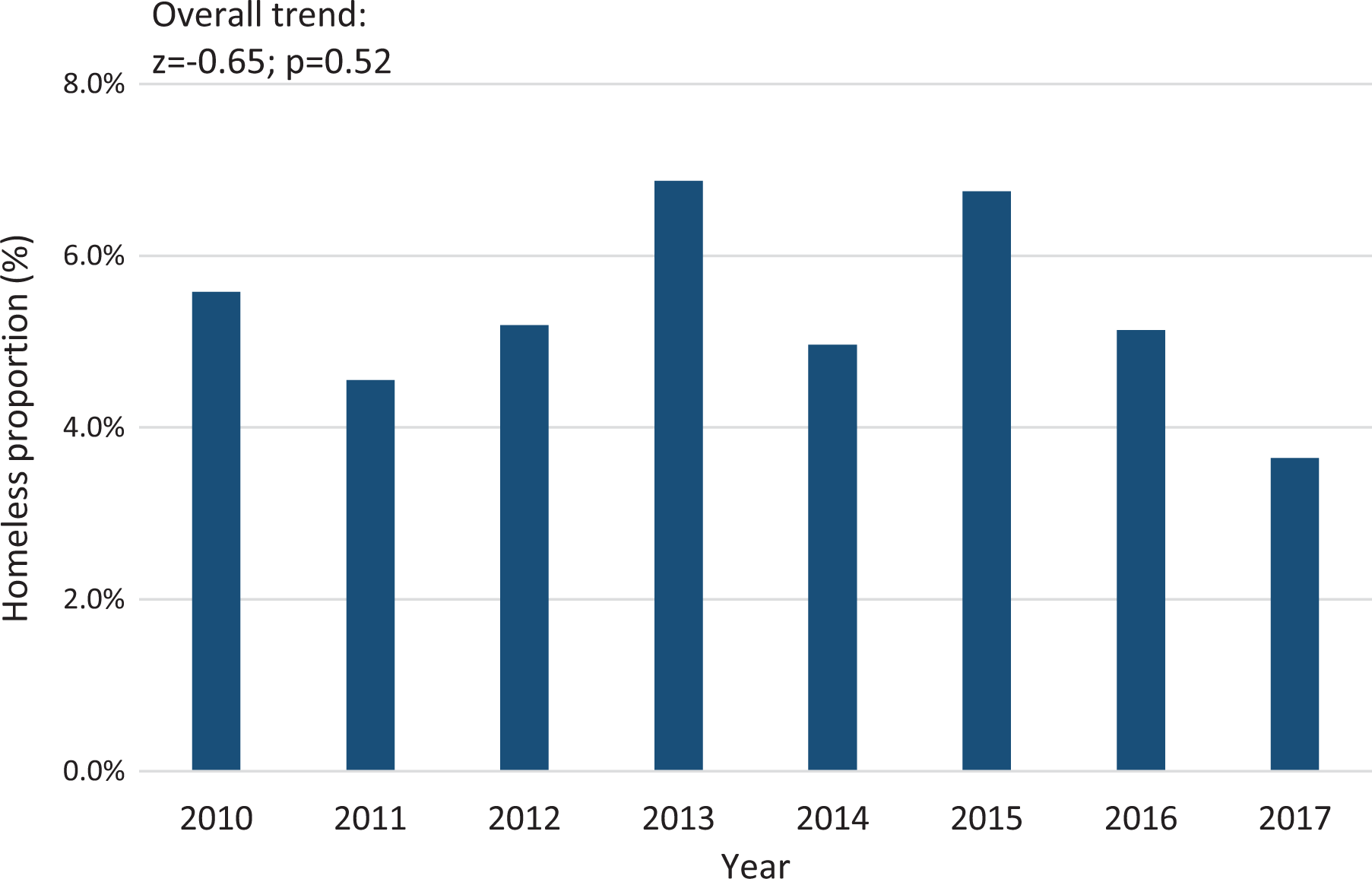
Percentage of persons with tuberculosis in Texas from January 1, 2010, through December 31, 2017, who were identified as experiencing homelessness in the 12 months before being reported to the National TB Surveillance System. Data source: Centers for Disease Control and Prevention. 8
Of the 543 PEH with TB, most were male (91.2%; n = 495), aged ≥45 (72.7%; n = 395), and non-Hispanic African American (47.5%; n = 258) (Table 1). Persons with TB living in homes were predominantly Hispanic (53.7%; 5150 of 9582). We found a significant difference between the proportion of US-born PEH with TB and the proportion of US-born persons with TB living in homes (85.1% vs 41.0%; χ2 = 409.1; P < .001). The proportion of PEH with TB was larger than the proportion of persons with TB living in homes for the following risk factors: excessive alcohol use (53.8% vs 14.9%; χ2 = 551.3; P < .001), injection drug use (10.9% vs 1.8%; χ2 = 185.7; P < .001), HIV positivity (16.0% vs 5.8%; χ2 = 92.9; P < .001), unemployment (70.7% vs 25.8%; χ2 = 517.9; P < .001), and having a previous report of TB (9.2% vs 3.6; χ2 = 43.9; P < .001). Clinically, a lower proportion of PEH with TB had completed treatment (75.5% vs 86.1%; χ2 = 126.5; P < .001) and a higher proportion had positive sputum smears (46.4% vs 36.0%; χ2 = 40.6; P < .001), positive sputum culture results (71.8% vs 53.5%; χ2 = 76.7; P < .001), and abnormal chest radiography (91.7% vs 82.5%; χ2 = 31.6; P < .001). We found only 1 case of multidrug resistance among PEH with TB during the study period.
MTB strains were genotyped among 82.1% (446 of 543) of PEH with TB and 71.0% (6804 of 9582) of persons with TB living in homes (Table 1). Of the 446 genotyped PEH with TB, 96.8% (n = 427) had East Asian or Euro-American lineages and 94.4% (n = 421) were included in 118 clusters. The largest cluster, TX 0002 (PCRType PCR00015), included 139 (31.2%) PEH with TB in Texas. Persons with TB living in homes had a significantly lower proportion of cases included in clusters (56.8% vs 77.5%; χ2 = 1439.2; P < .001).
Among persons with TB in Texas, being male increased the odds of being homeless compared with being female (odds ratio [OR] = 4.04; 95% confidence interval [CI], 2.94-5.56) (Table 2). Being aged ≥45 compared with being aged <45 (OR = 1.99; 95% CI, 1.60-2.46), being non-Hispanic African American compared with not being non-Hispanic African American (OR = 2.59; 95% CI, 2.11-3.18), living in an urban county compared with living in a rural county (OR = 3.08; 95% CI, 1.73-5.46), consuming excessive alcohol compared with not consuming excessive alcohol (OR = 3.23; 95% CI, 2.64-3.94), having a history of injection drug use compared with not having a history of injection drug use (OR = 2.32; 95% CI, 1.62-3.31), having a previous report of TB compared with not having a previous report of TB (OR = 2.09; 95% CI, 1.44-2.85), and having pulmonary TB compared with having extrapulmonary TB (OR = 1.95; 95% CI, 1.33-2.85) were associated with an increased risk of homelessness among persons with TB. Being non–US-born compared with being US-born (OR = 0.26; 95% CI, 0.20-0.34) and having a diagnosis of diabetes compared with not having a diagnosis of diabetes (OR = 0.58; 95% CI, 0.42-0.80) decreased the odds of being a PEH with TB.
Multivariate analysis for risk factors for homelessness among 10 098 persons with tuberculosis in Texas, 2000-2017a
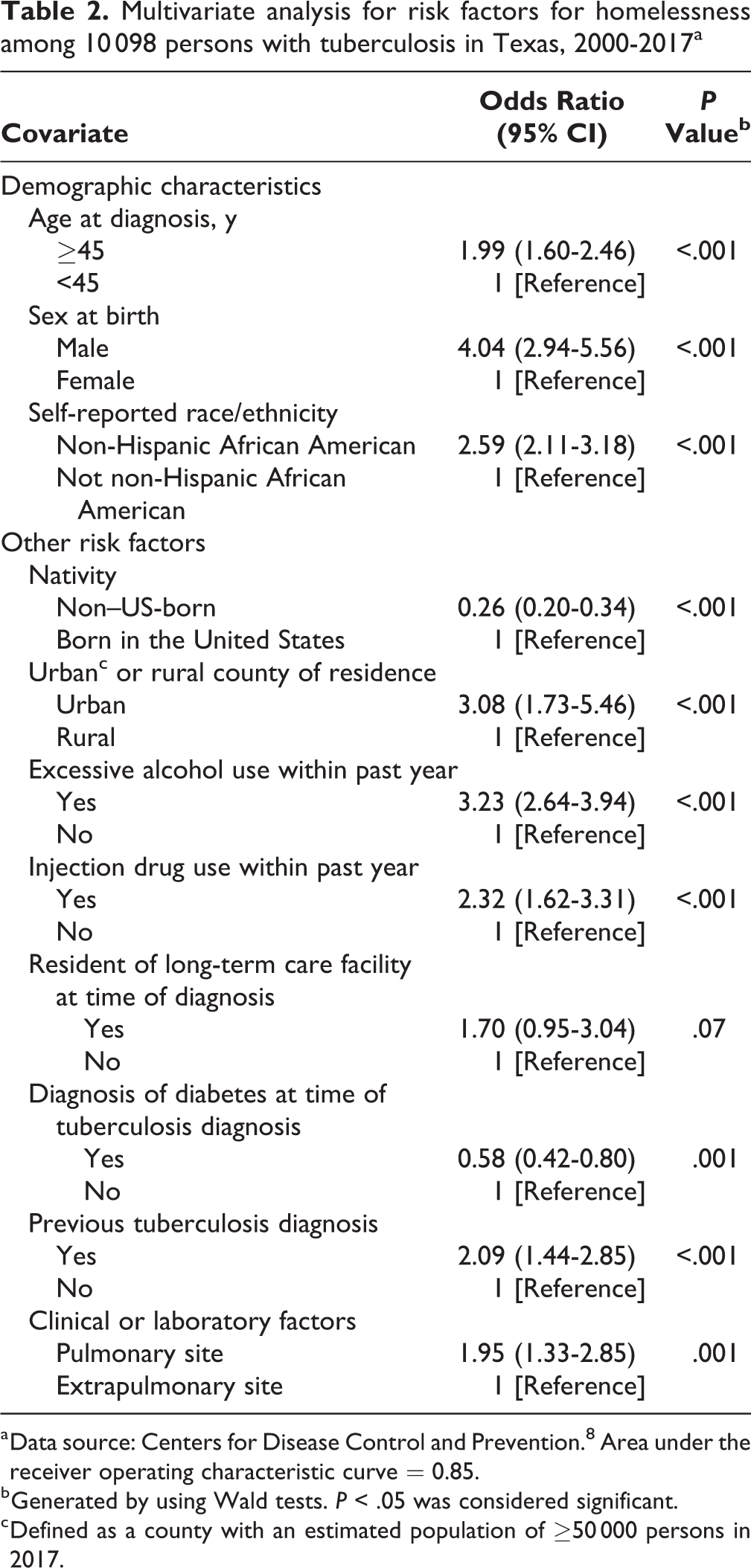
a Data source: Centers for Disease Control and Prevention. 8 Area under the receiver operating characteristic curve = 0.85.
b Generated by using Wald tests. P < .05 was considered significant.
c Defined as a county with an estimated population of ≥50 000 persons in 2017.
PEH with TB had 2.26 times increased odds of dying during treatment than persons with TB living in homes (OR = 2.26; 95% CI, 1.68-3.03). In the analysis of risk factors for death among PEH with TB during treatment, we found that not having a culture conversion or having an unknown culture conversion compared with having a culture conversion significantly increased the odds of death by 47.50 times (OR = 47.50; 95% CI, 15.90-142.30). TB case verification by a laboratory test compared with TB case verification based on clinical case definition also significantly increased the odds of death among PEH with TB (OR = 26.30; 95% CI, 3.27-211.20), as did radiographic evidence of cavitation compared with not having radiographic evidence of cavitation (OR = 4.95; 95% CI, 1.90-12.90) or miliary disease compared with not having miliary disease (OR = 8.74; 95% CI, 1.42-53.90), and 2 demographic characteristics: age ≥45 compared with age <45 (OR = 4.59; 95% CI, 1.39-15.20) and positive HIV status compared with negative or unknown HIV status (OR = 3.57; 95% CI, 1.14-11.20) (Table 3).
Multivariate analysis for risk factors for death during treatment among 355 persons experiencing homelessness with tuberculosis in Texas, 2000-2017a
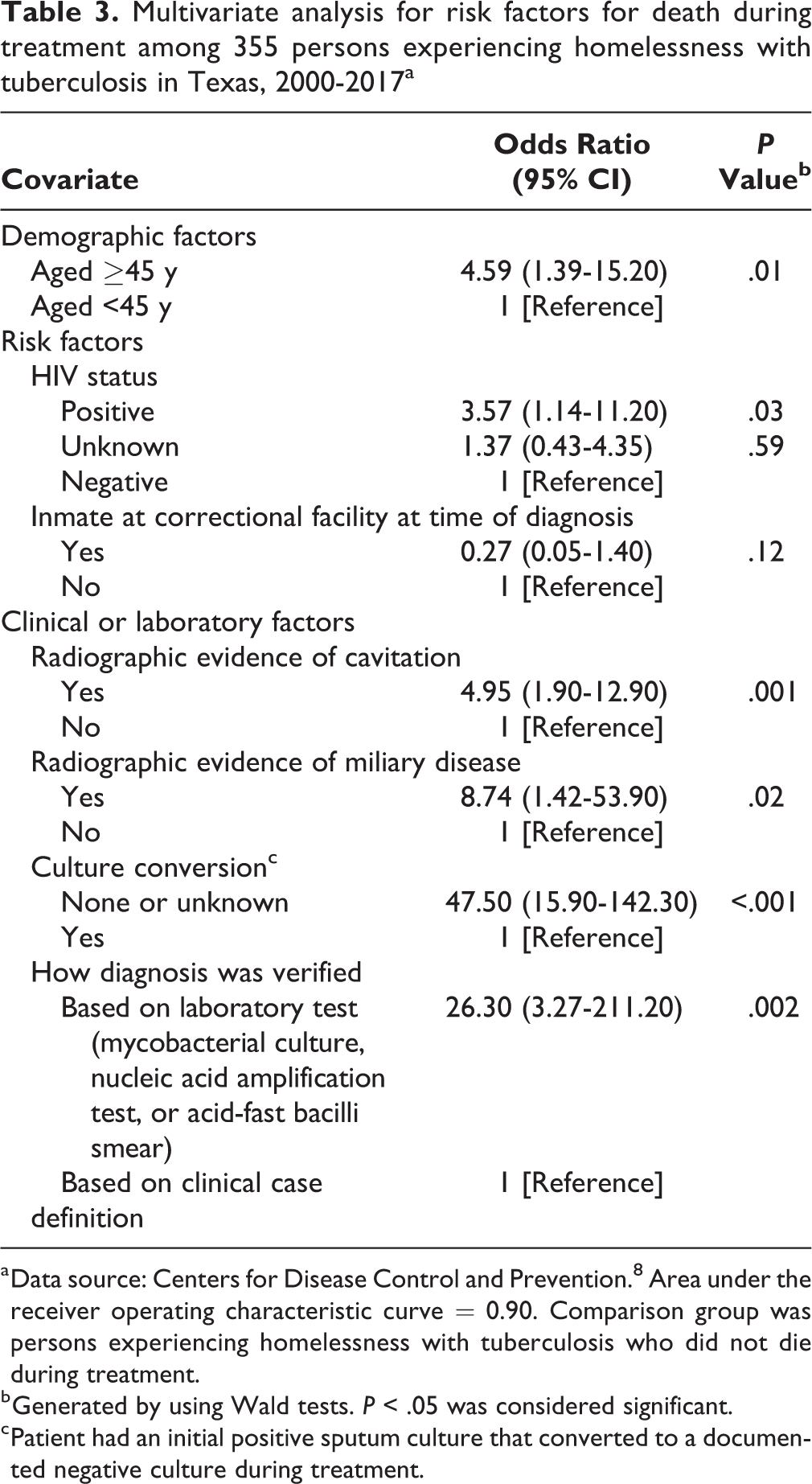
a Data source: Centers for Disease Control and Prevention. 8 Area under the receiver operating characteristic curve = 0.90. Comparison group was persons experiencing homelessness with tuberculosis who did not die during treatment.
b Generated by using Wald tests. P < .05 was considered significant.
c Patient had an initial positive sputum culture that converted to a documented negative culture during treatment.
More than 90% of PEH with TB in Texas lived in urban counties. Of the 2 most heavily populated counties in Texas, Dallas County accounted for 215 of 543 (39.6%) PEH with TB and Harris County (Houston) accounted for 125 of 543 (23.0%) PEH with TB (Figure 2). The most common GENType among PEH with TB in Dallas County was G10508 (PCRType PCR00015) (44.0%; 80 of 182); no PEH with TB in Harris County had this GENType. The most common GENType among PEH with TB in Harris County was G00010 (PCRType PCR00002) (48.4%; 46 of 95); 1.7% (3 of 182) of PEH with TB had this GENType in Dallas County. In Dallas County, being Hispanic (OR = 0.11; 95% CI, 0.05-0.21) or non-Hispanic white (OR = 0.53; 95% CI, 0.32-0.86), being an inmate at a correctional institution (OR = 0.48; 95% CI, 0.23-0.99), and having a positive acid-fast bacilli smear (OR = 0.54; 95% CI, 0.32-0.91) were significantly associated with decreased odds of homelessness, whereas mycobacterial culture positivity was associated with increased odds (OR = 1.92; 95% CI, 1.04-3.56) of being a PEH with TB. In Harris County, age ≥45 (OR = 2.17; 95% CI, 1.12-4.18), excessive alcohol use (OR = 3.00; 95% CI, 1.71-5.24), and being an inmate at a correctional institution (OR = 3.50; 95% CI, 1.77-6.95) were associated with increased odds of being a PEH with TB.
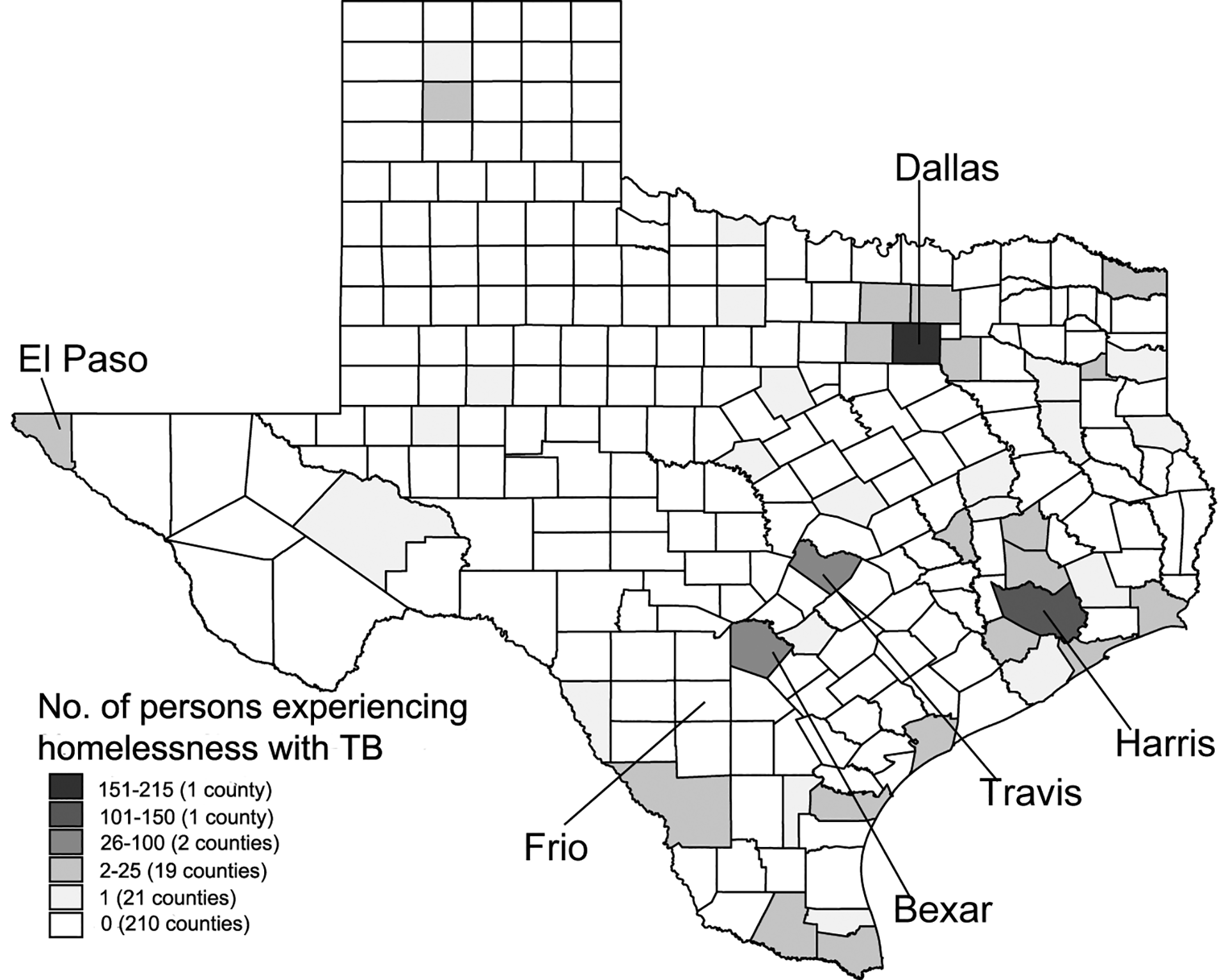
Map of Texas showing the frequency of persons with tuberculosis from January 1, 2010, through December 31, 2017, who were identified as experiencing homelessness in the 12 months before being reported to the National TB Surveillance System, by county of residence. Data source: Centers for Disease Control and Prevention. 8
Discussion
During 2010-2017, 5.4% of persons with TB who had MTB isolates submitted for genotyping in Texas were identified as being homeless. Two surveillance studies estimated the rate of homelessness among persons with TB as 6% in the United States from 1994 through 2010. 4,11 Although TB incidence is decreasing in the United States, 2 the proportion of TB cases among PEH was 4.1% in 2018 and has not changed greatly over time. 4 The proportion of persons with TB who were experiencing homelessness varied at most by 3.3% in this study. This result is similar to the results of a study showing that the proportion of PEH with TB ranged from 6.1% to 6.7% for all reported TB cases in the United States from 1994 to 2003. 11
PEH with TB are at a greater risk of death during treatment than persons with TB living in homes in Texas. Not having a culture conversion or having an unknown culture conversion, TB case verification by a laboratory test, radiographic evidence of cavitation or miliary disease, being aged ≥45, and being HIV positive increased the odds of death during treatment among PEH with TB compared with persons with TB living in homes. The greater risk of death among PEH may be due in part to a delay in diagnosis among PEH, who often face barriers to accessing care. It may also be due to greater severity of disease among PEH: evidence of cavitation and miliary disease reflects a high bacterial burden and greater disease severity. 12 Treatment completion rates among PEH with TB in Texas (75.5%) were lower than treatment completion rates reported in a national study that analyzed data from 1994 through 2010 (89% among US-born PEH and 81% among non–US-born PEH); this lower completion rate may have contributed to the greater risk of death among PEH with TB than among persons with TB living in homes. 4 Homelessness in persons with TB in the United States can be associated with being hospitalized more frequently and with longer stays than persons with TB living in homes. 13 A study following TB patients in multiple public health programs in the United States found that 9.9% of study participants who were homeless accounted for 15.9% of hospitalizations and 17.7% of total hospitalization costs generated by study participants. 14 A study of PEH with TB in Houston found that the degree of homelessness (living in someone else’s home, transient, sheltered in a public shelter, or on the street) influenced TB incidence and that different demographic and lifestyle factors were associated with each level of homelessness. 6 The Houston study also showed that the length of hospitalization (in mean number of days) increased as the level of homelessness increased. In addition, it indicated that persons on the street were in poorer physical health or at a more advanced stage of TB disease than persons who had a lesser degree of homelessness, before they sought health care. 6 The proportion of PEH who were infected with drug-resistant MTB isolates was low in the Houston study, which agrees with a nationwide study conducted from 1994 to 2003 that found that PEH with TB were no more likely than persons with TB living in homes to have a drug-resistant strain of MTB. 11
We found significantly more MTB strain clustering among PEH with TB than among persons with TB living in homes, and a greater proportion of PEH who had TB were in urban counties compared with persons with TB living in homes (97.6% vs 91.9%). Clustering is a surrogate marker for recent transmission of MTB. 15 Homelessness has been found to be a significant risk factor for MTB strain clustering in both US-born and non–US-born PEH with TB. 16 PEH are also more likely than persons living in homes to have other risk factors, such as participation in congregate settings and malnutrition, known to be associated with TB transmission. 17 In our study, PEH with TB had a significantly lower proportion of drug-resistant MTB and significantly more clustering than persons with TB living in homes, indicating that local strains of MTB were being introduced and transmitted in communities of PEH. More than 30% of the genotyped strains found in PEH with TB were in a single cluster, indicating continuous transmission among this group. Outbreaks among congregate settings such as homeless shelters have been documented, 18 and frequent use of public transportation has also been found to be a risk factor for TB infection. 6 However, PEH are known to have several locations that they visit often, and these locations are often near to where they sleep. Transmission patterns among PEH may be complex and require a network analysis to identify and disrupt the transmission dynamics. 19,20
The Texas Department of State Health Services reported TB case rates in several counties in Texas to be 0 per 100 000 population in 2017; the same report noted 61.2 cases per 100 000 population in Frio County, Texas. 21 In our study, most (85.1%) PEH with TB were US-born, and most (59.0%) persons with TB living in homes were non–US-born. Nationally, most persons with TB are non–US-born. 5 Being of Hispanic ethnicity significantly reduced the odds of a TB patient being homeless in Dallas County, which reflects the national trend of Hispanic persons composing a small percentage of PEH in the United States. Five percent of PEH in the United States in 2017 were Hispanic or Latino. 22
In Texas, 62.6% (340 of 543) of PEH with TB were in Dallas and Harris counties. Understanding the epidemiology of PEH with TB in urban areas is important in Texas. Unexpectedly, although the 2 counties are not far apart (approximately 240 miles), the characteristics associated with PEH with TB differed between Dallas and Harris counties. The most common GENType (cluster) among PEH with TB in each county differed, indicating that no dynamic transmission is taking place between PEH populations in the 2 counties. When TB prevention and control programs evaluate their allocation of resources, they should consider regional differences in PEH who have TB and populations at high risk for morbidity and mortality.
Limitations
Our study had several limitations. First, the data set was incomplete. Our analyses comprised data on persons reported to have TB, so a bias may have resulted from TB cases that were not reported. However, it is unlikely that there were enough nonreported TB cases to introduce a systemic bias. The GENType analysis may not represent the genotypes for all TB patients; genotyping coverage was only 88.2% in the United States in 2010, although it increased to 96.3% by 2017. 23 Texas has a high coverage of MTB isolate genotyping, so most of the culture-positive persons with TB (>97%) had isolates sent for genotyping in 2016. 24 Second, the discriminatory power of the MTB genotyping techniques used may have been insufficient to resolve various endemic strains being transmitted and, thus, may have led to low resolution of GENTypes and clusters. Third, to capture data on all persons with unstable housing or no housing, the Centers for Disease Control and Prevention’s instruction manual for reporting a case of TB broadly defines homelessness. 8 Even when using this broad definition, the surveillance mechanism may not be able to capture data on all PEH, or some minimal reporting bias may exist. PEH in general and PEH with TB may not accurately indicate their residential status to prevent being stigmatized or dehumanized. Despite these limitations, the analysis still allows for policy and planning of resource allocation to public health jurisdictional areas in Texas.
Conclusions
The incidence of persons with TB per year is declining in the United States, but PEH continue to bear an undue burden of mortality from the disease. Older age, positive HIV status, and radiographic evidence of cavitation or miliary disease indicate advanced TB disease due to delayed diagnosis. Prioritization of the identification and treatment of PEH with TB disease is essential for public health entities in Texas to control and eliminate TB in the state.
Footnotes
Acknowledgments
Each author contributed equally to the research, authorship, and publication of this article. We acknowledge the selfless work of public health officials and staff members at the City of Houston Bureau of Tuberculosis Control, Houston Department of Health & Human Services; the Harris County Public Health and TB Elimination Program; the Dallas County Public Health and TB Elimination Program; the Texas Department of State Health Services; and the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.