
Abstract

Public health issues, such as emerging health threats, globalization of health, and a rapidly aging population, are challenging the public health system. 1 -4 These health demands require public health leaders who have the skills and competencies to address a changing landscape. 5,6 These skills go beyond discipline-specific domains. To address public health challenges, leaders need skills that span areas that might not be taught in traditional schools and programs of public health, 7 including “less definable skills in leadership, communication, problem solving, and systems thinking.” 8
The public health workforce is also changing. The Public Health Workforce Interests and Needs Survey—a nationally representative survey conducted in 2014 with respondents from 37 state health agencies and a convenience sample of local health departments in the 14 Big Cities Health Coalition and more than 50 local health departments 9 and again in 2017 with 47 state health agencies and 97 local health departments 10 —examined various topics related to public health employees’ perceptions of workforce issues. Among these issues was a respondent’s intention to leave his or her organization. The percentage of staff members who intended to leave their organizations within the next year or retire within 5 years increased from 44% to 48% from 2014 to 2017 among the 33 state health agencies that participated in both survey years. When retirement was excluded, the increase was from 22% in 2014 to 31% in 2017. 11 In the 2017 survey, a comparable number of respondents indicated leaving public health altogether (6%) and finding another public health position (7%). 12 Although not all staff members who intend to leave public health are in a leadership role, the loss of effective employees at all levels negatively affects the potential talent pool of future organizational leaders.
The federal system is also facing workforce challenges. According to the US Government Accountability Office, an estimated 31% of federal employees in 2012 were eligible for retirement by fall 2017; the estimate from the US Department of Health and Human Services was 35%. 13 The 2018 Federal Employee Viewpoint Survey captured information on federal employees’ perceptions about workplace issues. A total of 598 003 government employees responded to the 2018 Federal Employee Viewpoint Survey. Of the 563 434 respondents to a question about their plans to retire, 142 459 respondents reported plans to retire within the next 5 years. Moreover, when asked about their turnover plans, 100 354 (18%) of the total 567 838 respondents to the question planned to take another position in the federal government, and 22 298 (4%) planned to leave for a position outside government. 14
The 2014 State of Human Capital Report noted that federal agencies in particular lack adequate leadership preparation, 15 underscoring the potential effect on organizational leadership that can result from workforce loss. With many vacancies occurring in leadership positions, 16,17 the public health system risks losing institutional memory and leadership skills that can negatively affect agency performance.
The potential effect of retirement and other retention challenges in all public health sectors requires a deliberate examination of how these organizations are addressing loss of workforce and leadership skills and capacities. A 2017 report by the Center for State and Local Government Excellence noted recruitment and retention as the top workforce priority for state and local public health organizations, followed closely by staff development, leadership development, and succession planning. 18 A focus on leadership development as essential to building and maintaining public health infrastructure was a focus of sentinel reports by the Institute of Medicine 19 -21 and others, 15 -18 who noted deficiencies in public health infrastructure and called for an examination of how public health organizations were addressing and prioritizing leadership development. In addition, the 2013 National Public Health Workforce Strategic Roadmap called for the development of “robust leader and leadership offerings” as a strategy for strengthening the public health workforce. 22
At a time when public health leadership development programs are most needed, they are on the decline. 23 This decline can be especially concerning in organizations that have scientific subject matter experts who are skilled in disciplines but who might lack broad-based leadership skills. For example, in 2010, the US Merit Systems Protection Board found that supervisors in scientific institutions were often selected on the basis of technical or scientific achievements and expertise rather than leadership ability. 24 The board noted that technical skills rather than supervisory skills were prioritized in leadership position announcements. This prioritization can be problematic because the skills needed to be effective in leadership roles might not align with the skills developed over time by persons applying for these positions. 25 -28 As a result, scientific staff members entering into nonscience leadership roles often must develop skills that are not part of their career development. 29
Similar to other public health organizations, the Centers for Disease Control and Prevention (CDC) is often challenged with transitioning scientific staff members into nonscience leadership roles, often when they were not fully developed for these roles. Not having the necessary skills can result in an ineffective leader, low morale, and a decline in program effectiveness. It is important, then, to understand what factors successful public health leaders identify as contributing toward their transitions into supervisory leadership roles. Public health organizations can then use these factors to inform comprehensive leadership development programs that help ensure relevance, sustainability, and effectiveness of the work.
To identify these factors, the lead author (A.L.F.) conducted in-person interviews with 21 supervisory leaders at CDC’s Atlanta, Georgia–based offices who had transitioned successfully (ie, received leadership awards and high performance ratings) from primarily scientific roles into supervisory leadership roles by using the appreciative inquiry approach, which examines past experiences to inform future success. 30 Interviews took place from February 3 through March 23, 2016. Supervisory leadership roles were defined as CDC branch leaders or higher (branch leaders, division directors, associate directors for science, and center directors) with primarily supervisory, non-science–specific duties.
Factors That Affect Transitions Into Supervisory Leadership Roles
Respondents noted 58 factors that potentially leveraged the transition of technical experts into leadership positions (Box). Although no single factor emerged as sufficient for transitioning into a successful leadership role for all respondents, 3 factors appeared to support a successful transition into leadership for most respondents: (1) receiving support from leadership throughout one’s career (support from leadership), (2) leading an activity through which one could demonstrate leadership beyond one’s scientific role (leading an activity), and (3) obtaining opportunities for new roles (opportunities).
Most respondents discussed having had support from leadership throughout their professional careers. This support included expressions of confidence. As the most frequently mentioned factor, support from leadership appeared to positively affect the professional experiences of most respondents. One respondent said: [Leadership] spent enough time with me to understand what I needed about what they were trying to do and gave me feedback and gave me exposure and time with them and brought me into meetings—the meetings I would never have been brought into before—and kind of expressed one-on-one and publicly great confidence in me, which does wonders for anybody.
Respondents discussed times when they were leading an activity as allowing them to do something outside of their exclusively scientific roles and demonstrate leadership skills. Although many respondents were chosen for leadership because of their scientific skills, this new role was a chance for them to develop and demonstrate additional leadership abilities beyond those that they had used as a scientist. Working in this new role or capacity often led to increasing levels of responsibility and an eventual move into leadership. Respondents noted: At that time, I had to do the whole budget, the contracting work, all [of those things]. I was learning all [of those things] for the first time. The 2 years was actually a really tough job, but what it did was it got me my foot in the door…and eventually [helped me] get into trusted positions within that office. I think people knew that I had an interest in global health and so just in a perfectly happy situation over there and then somebody called me one day and said, “Would you like to do global health?” So that’s how these things have all sort of come about. It was because I was given an opportunity to interact with quite a few leaders and meet with them and try to understand what it is they needed and then provide a solution. I would say [leadership] was supportive that somebody was willing to take [a leadership activity] on; recognizing that somebody needed to take it on and was willing. Again, it was this opportunity to have autonomy, to build something in this branch and in our division that had never been built before. I had free reign in terms of how I wanted that to look, and I thought, “What an opportunity.” So I said, “Of course I would like to do that.” I can’t emphasize how important this was…that when your boss comes to you and says, “I have a meeting with [leadership] the day after tomorrow on this topic and I would really like you to go with me and present the overview and then I’ll be there with you” as opposed to a different approach that would be, “Can you please give me a briefing document because I’m gonna go and present this.” It’s huge.…Or, you know, “I really think this would be a good opportunity for you to present at this international conference and would you like to go?” Mentorship is important to give you guidance, to help you avoid those landmines. And if you fall into a landmine or encounter one as a supervisor or something else, how to negotiate and get out of those things.
Implications for Public Health Organizations
In scientific organizations that are facing large numbers of retirements, scientific staff members are often asked to step into roles that require a set of skills that differs from those they have primarily used during their careers. Therefore, it can be valuable for scientific organizations not only to develop a broad talent pool from which leaders can emerge for a wide variety of roles but also to identify staff members who are interested in leaving their scientific roles for positions requiring different skill sets. Regular staff-supervisor meetings could allow leaders to assess and support their staff members’ interest in such activities by identifying and providing growth opportunities and leadership roles.
Mentorship emerged as influential for staff members who later transitioned into successful leaders. Interestingly, all of the mentor relationships mentioned had developed organically rather than via formal mentoring programs. Supporting informal mentorship can prove to be a win-win for organizations and their employees. Staff members who serve as informal mentors can include these relationships in their own performance evaluations. Documenting the value of informal mentoring to an organization can reinforce the importance of such relationships to professional growth.
Support from leadership was a key factor for respondents. Many respondents indicated having supervisors who had confidence in them, often more confidence than they had in themselves. This confidence could have developed as they demonstrated their abilities and skills, resulting in increased leadership confidence and additional opportunities. The shared responsibility for professional growth is reflected in this factor. By recognizing talent, providing staff members with opportunities, and forging relationships with their staff members, organizational leaders can be willing and equally active respondents in the growth and development of staff members at all levels.
Another consideration is that of leading activities. As noted by several respondents, leading an activity provided exposure to new areas of work and responsibilities and a way for them to develop new strengths. Because supervisors are generally best positioned to provide staff members with a chance to lead an activity, supportive and open dialogue are needed. For example, performance evaluation discussions can provide dedicated time for staff members and supervisors to discuss goals and objectives for professional growth. Through these discussions, supervisors can help staff members discover ways for them to lead activities and learn and demonstrate new skills.
Interestingly, training that respondents had received did not emerge as a primary factor. Eight of the 21 respondents indicated that training courses would have been more helpful earlier in their career development. An alternative model to the traditional training approach could be one of action learning, defined broadly as acting on a particular concern, reflecting on the action taken, and modifying the action as needed. 31 Applying action learning to leadership development can provide hands-on opportunities to develop or demonstrate a new skill in real time. CDC conducts a yearly training needs assessment to determine and increase the number of offerings for employees. Incorporating questions that are specific to employees who are considering leadership roles can help inform offerings, ensure that training programs are tied to relevant hands-on practice, and give leadership a better understanding of the demand for transition-related information.
Given these findings, a consideration becomes how to provide opportunities to lead or grow and how to ensure support from leadership, both overall and as scientific staff members transition to leadership positions. For example, supervisors and staff members can discuss what leadership opportunities are available or which leadership course offerings can couple curriculum with applied experience, making leadership development part of the organizational culture.
The 3 primary factors highlighted in this article are starting points for further research and discussion about public health workforce development. Public health organizations can benefit from investing thought and resources to enhance the development of scientists and all staff members to ensure a talent pool from which organizational leaders may emerge.
Although the 3 primary factors were relevant to the experiences of most respondents, no 2 experiences were exactly the same. This finding speaks to the importance of applying research to practice and indicates that leadership development efforts can be tailored to the individual. Organizations can create leadership development initiatives that integrate personal strengths so that staff members can note their growth over time and how it affects the organization. 32 Furthermore, seeking ways to integrate leadership development initiatives into the existing organizational infrastructure and align with the overall strategic direction of the organization can make such efforts part of the organizational culture. 33 Over time, it is possible that organizations that integrate leadership development into their cultures might find that factors such as leadership support and providing opportunities for staff members become the norm. Elements of success can inform what is offered to help transition staff members (eg, trainings, development opportunities, mentorship) into the organizational culture. 8
The public health sector faces challenges with leadership development. These challenges are heightened for science-based public health organizations that need to transition scientific professionals who might not have developed the skills necessary for new leadership roles. Such initiatives, then, are critical to helping ensure the transfer of knowledge and leadership skills that can keep these organizations functioning at their best. Implementing timely and relevant leadership development that provides opportunities to learn and demonstrate skills and lead activities—and cultivating it through supportive leadership and mentors—can make the difference.
Factorsa for transition of scientific experts into successful supervisory leadership positions (in alphabetical order) among supervisory leaders at CDC (N = 21), Atlanta, Georgia, 2016b
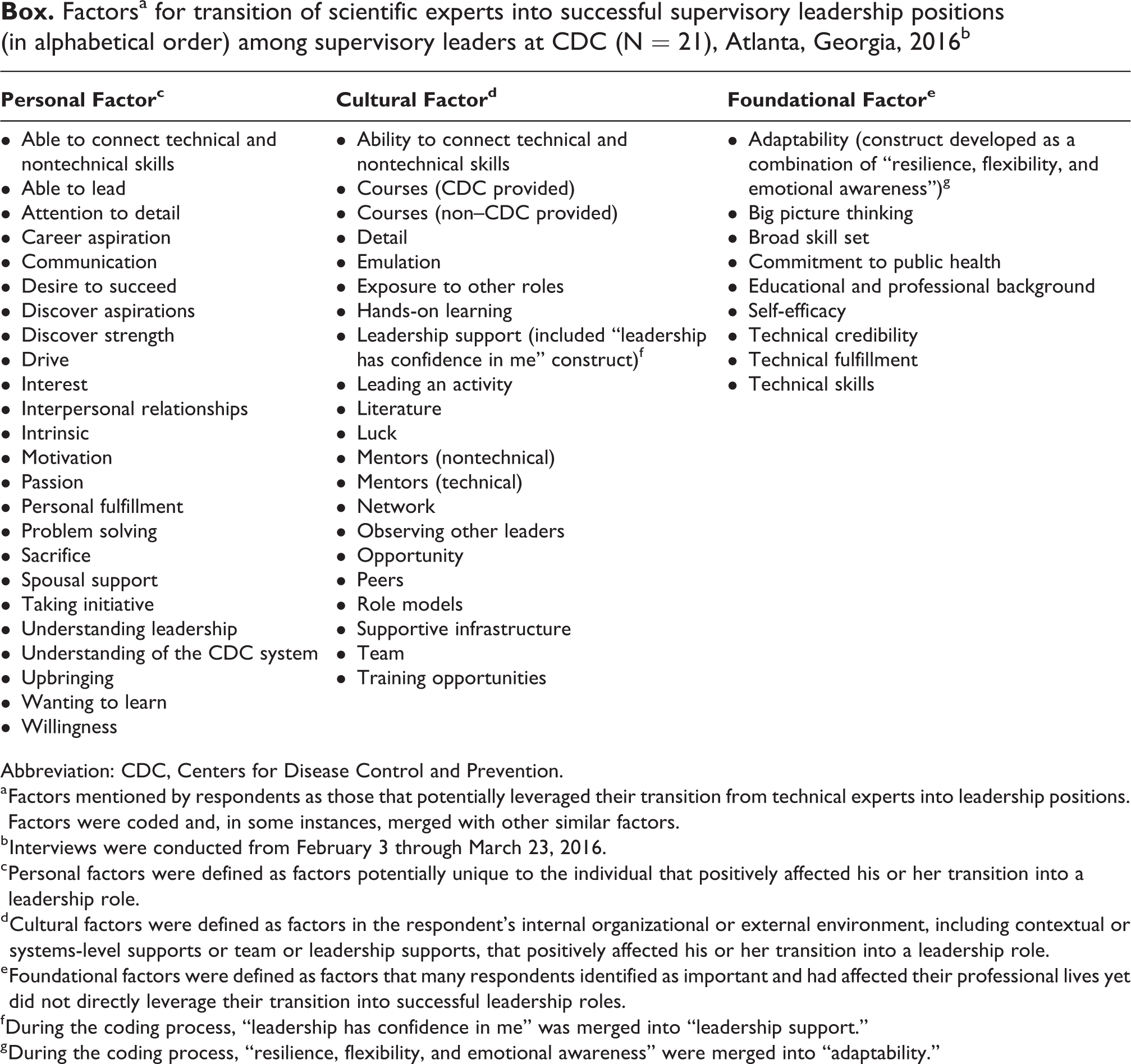
Abbreviation: CDC, Centers for Disease Control and Prevention.
a Factors mentioned by respondents as those that potentially leveraged their transition from technical experts into leadership positions. Factors were coded and, in some instances, merged with other similar factors.
b Interviews were conducted from February 3 through March 23, 2016.
c Personal factors were defined as factors potentially unique to the individual that positively affected his or her transition into a leadership role.
d Cultural factors were defined as factors in the respondent’s internal organizational or external environment, including contextual or systems-level supports or team or leadership supports, that positively affected his or her transition into a leadership role.
e Foundational factors were defined as factors that many respondents identified as important and had affected their professional lives yet did not directly leverage their transition into successful leadership roles.
f During the coding process, “leadership has confidence in me” was merged into “leadership support.”
g During the coding process, “resilience, flexibility, and emotional awareness” were merged into “adaptability.”
Footnotes
Acknowledgments
The authors thank Dr Joseph Sniezek, Tracy Hilliard, Med Sohani, and Dr Patrick Lenihan for their guidance and insights. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. The material is based upon a dissertation, submitted in partial fulfillment of the requirements for the doctoral degree at the School of Public Health of the University of Illinois at Chicago.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.