
Abstract

Keywords
Few national data collection efforts have provided public health data on the criminal justice–involved population (defined hereinafter). The Bureau of Justice Statistics, an agency in the US Department of Justice, routinely collects, analyzes, and disseminates data on health and mortality in prisons and jails to monitor trends and inform policy and planning (Table 1). 1 -4 Agencies such as the Substance Abuse and Mental Health Services Administration and the National Institute on Alcohol Abuse and Alcoholism direct or conduct surveys of the currently noninstitutionalized population to characterize substance use among persons with a history of criminal justice involvement. 18
Known health data currently collected on persons in criminal justice systems,a by agency and country
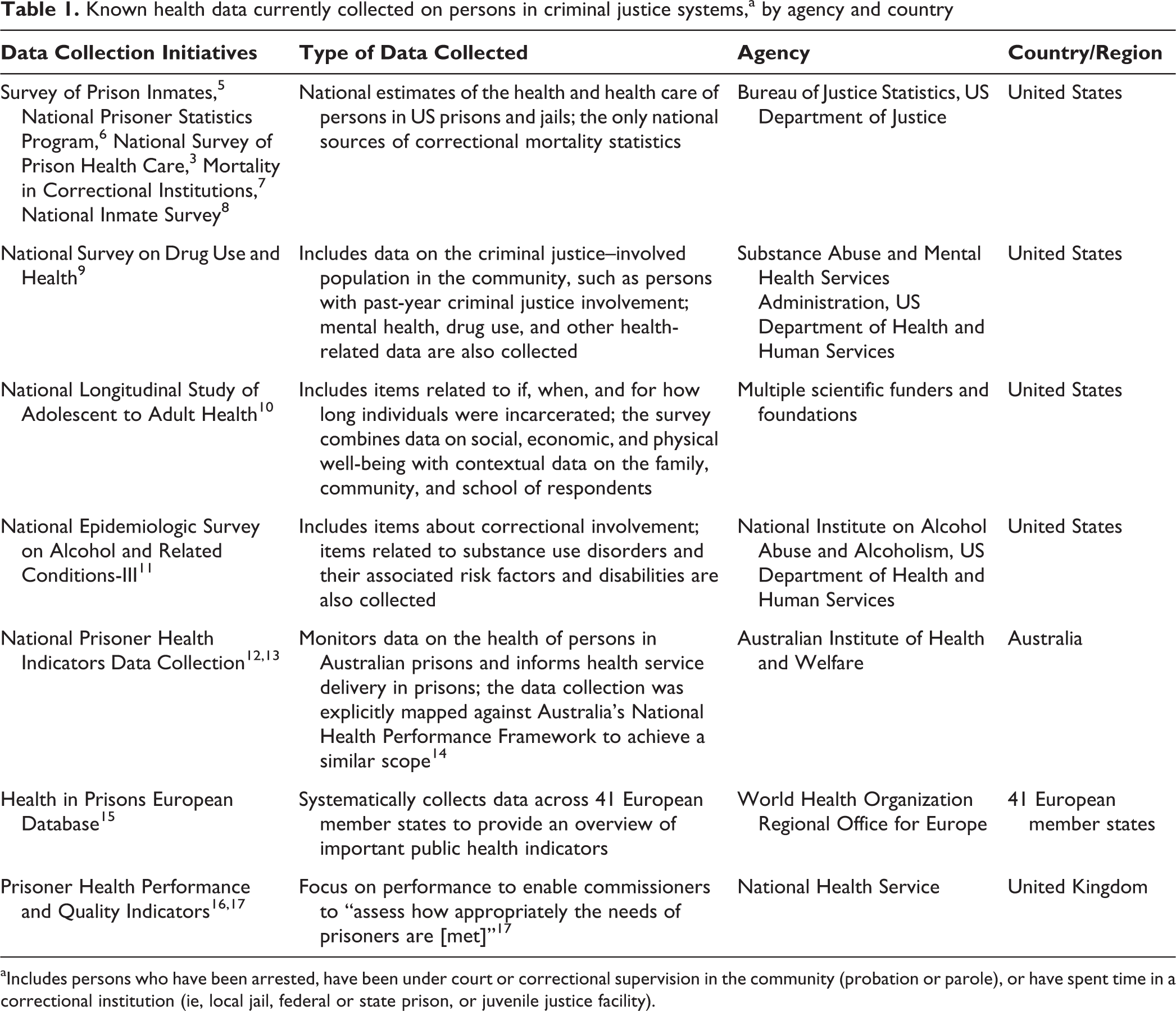
aIncludes persons who have been arrested, have been under court or correctional supervision in the community (probation or parole), or have spent time in a correctional institution (ie, local jail, federal or state prison, or juvenile justice facility).
Most national public health data collection systems exclude persons in correctional facilities and do not record information about previous involvement in the criminal justice system, such as the number of arrests and incarcerations or how much time was spent on probation and parole. 10 Thus, existing data may not be meeting the needs of public health and medical practitioners, policy makers, and the public for health data on this population.
Therefore, we need to expand the collection of national data on the health of the criminal justice-involved population. To make sure that the data collected effectively address the needs of various stakeholders, it is important to identify the purposes for their collection. Defining the purposes would help ensure that the data elements and frequency of collection are consistent with the intended uses of this information. This practice is particularly important for health data related to the criminal justice system because of the unique ethical, logistical, timing, and scientific challenges involved in collecting data in these settings. Such challenges also make adhering to established principles of public health data collection more difficult. Thus, the Bureau of Justice Statistics supported a project to identify the major purposes for collecting data on the criminal justice population and to define fundamental principles for collecting data on this population. The findings of this project were presented at a 2016 workshop hosted by the National Academies of Sciences, Engineering, and Medicine on how to improve the collection of health data among persons involved in the criminal justice system. 19 We summarize the findings here.
The Importance of Collecting Health Data on the Justice-Involved Population
The health and medical needs of the large criminal justice–involved population 20 have important implications for public health. This population includes persons who have been arrested, who have been under court or correctional supervision in the community (probation or parole), or who have spent time in a correctional institution (ie, local jail, federal or state prison, or juvenile justice facility). On a given day, the number of persons on parole and probation or admitted to and released from jails and prisons may be many times greater than the estimated size of the incarcerated population. 21 In the United States, 6.6 million persons were under the supervision of probation, parole, prison, or jail authorities at the end of 2016, of which 2.2 million were in prisons or jails. 21 However, on a given day, the number of persons on parole and probation or admitted to and released from jails and prisons may be many times greater than the size of the incarcerated population estimated at the end of the year. For example, an estimated 10.6 million persons were admitted to jails during 2016. 22
Justice-involved persons often have social and economic vulnerabilities that affect their health, such as low educational attainment and limited employment opportunities. 2,5,23 This population does not have the same freedom of choice regarding health services or health behaviors as does the general population. Criminal justice settings are also a nexus for complex and syndemic health problems, such as HIV and hepatitis C virus (HCV) infection, tuberculosis, mental disorders, substance use disorders, cognitive disabilities, and, increasingly, noncommunicable diseases. 1,13,24 -29 Given the high prevalence of these health conditions, correctional health services can be costly and require a specialized infrastructure, specialty medical services, and dedicated pharmacy services. 30 In addition, because most justice-involved persons live in or return to the community, their health is an integral part of public health and even global health. 31
The health care quality and health service experiences of the justice-involved population are of interest, not only to those in the justice system but also to their families, social networks, and communities. In addition, public health officials, health care professionals, correctional health and non-health administrators, policy makers, legislators, governmental organizations, and human rights organizations use health data on this population. These interests are based on professional goals such as improving patients’ health (eg, for physicians and public health officials), organizational missions (eg, for human rights organizations), budget considerations (eg, for legislators), and mandates to maintain the safety and well-being of the population for which they are responsible (eg, for correctional administrators and policy makers). For example, data on common conditions in this population (eg, HCV infection) serve public health agencies by improving estimates of these conditions in the general population. 32 Health data on this population can also help correctional health administrators and professionals develop, select, evaluate, and, where appropriate, eliminate policies, programs, and interventions to allocate scarce resources more efficiently. Finally, policy makers can use these data to evaluate the impact of criminal justice and health policies on the health of the justice-involved population and of the general population.
Challenges to Collecting Health Data on the Criminal Justice–Involved Population
Despite its public health importance, knowledge about the health of the justice-involved population has important gaps. Persons in correctional facilities, including persons who may be lost to follow-up because of pending jail or prison stays, are often excluded from surveys, clinical trials, and other research studies. 33 -35 These exclusions may be driven by ethical guidelines or regulations designed to protect vulnerable populations, 36 -38 prohibitive research policies of individual facilities, or logistical barriers. These exclusions unintentionally limit the knowledge about the health of this population compared with that of the noninstitutionalized population.
Collecting data in correctional facilities requires addressing ethical concerns about research in prisons, as well as historical and cultural barriers to data collection. Extra precautions are needed to avoid coerced participation. Asking questions about past or current criminal justice involvement may be perceived as sensitive or stigmatizing; thus, it is important to keep data confidential.
Data collection in correctional facilities is also logistically complex, time consuming, and costly. The United States has about 2000 state and federal prisons and 2850 jail jurisdictions. Correctional facilities have rapidly cycling populations, are located in diverse geographic areas, and vary widely in size, with small jails holding fewer than 50 persons and large jails holding more than 2500 persons. 22
Criminal justice health data collection requires unique collaborations between the legal and justice system, public health experts, and government statistical agencies. Criminal justice agencies may not wish to participate in data collection because studies about unmet health needs may attract negative media attention. Other studies might lead to mandates that jails and prisons assume additional functions, but without additional funding. 39
Given these numerous challenges, agencies collecting health data on justice-involved populations need to identify and rank their purposes for collecting health data, which may differ from those of agencies collecting health data on other populations and from agencies collecting non-health data on the criminal justice population. To guide improvements in data collection by the Bureau of Justice Statistics, US public health agencies, and public health agencies involved in criminal justice health in other countries or regions, we identified the purposes for such data collection. To ensure that the resultant data can effectively address the purposes for their collection, even if collected by non-public health agencies, we also defined 5 principles to guide sampling, measurement, and reporting activities consistent with sound public health practice.
Identifying the Purposes and Principles of Data Collection in the Justice-Involved Population
To identify the major purposes for collecting data on the health of justice-involved populations and the principles to guide such collection, we reflected on our experiences collecting data in jails and prisons for research and health surveillance purposes and reviewed the literature and governmental and nongovernmental population health reports. Consistent with the World Health Organization’s definition of health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity,” 40 we considered purposes relevant to collecting data on acute and chronic diseases, unintentional and intentional injuries, health behaviors, health status, and well-being. We also considered purposes relevant to health service experiences, such as access to care, receipt of appropriate health services, and satisfaction with care.
Throughout the process of identifying the purposes of data collection, we considered the perspectives of diverse stakeholders, including public health practitioners, medical professionals, correctional health administrators, the general public, organizations seeking to improve justice health care delivery, policy makers, and persons who have had contact with the criminal justice system. We obtained this information through local and national meetings and through telephone calls and in-person meetings with national and international experts.
We contacted persons involved in collecting health data for prisons worldwide (eg, in the United States, Australia, Canada, United Kingdom, and the World Health Organization Regional Office for Europe) and stakeholders at conferences related to health in criminal justice settings. Their perspectives helped us to identify and refine the major reasons stakeholders seek data on the health and health service experiences of the justice-involved population and to ensure that the principles were relevant to the unique challenges of collecting data in criminal justice settings. Although the purposes and principles discussed below are designed to be relevant to the US justice-involved population, they may be modified to be applicable to other populations and countries.
Purposes of Data Collection
The purposes of data collection broadly represent the interests of stakeholders in 2 overlapping categories: (1) public health and medicine, which includes health surveillance, health promotion and disease prevention, and health care performance and patient value, and (2) government and society, which includes policy relevance, health equity, and human rights and legal considerations (Table 2).
Data on the health of the criminal justice–involved populationa and the purposes for collecting these data
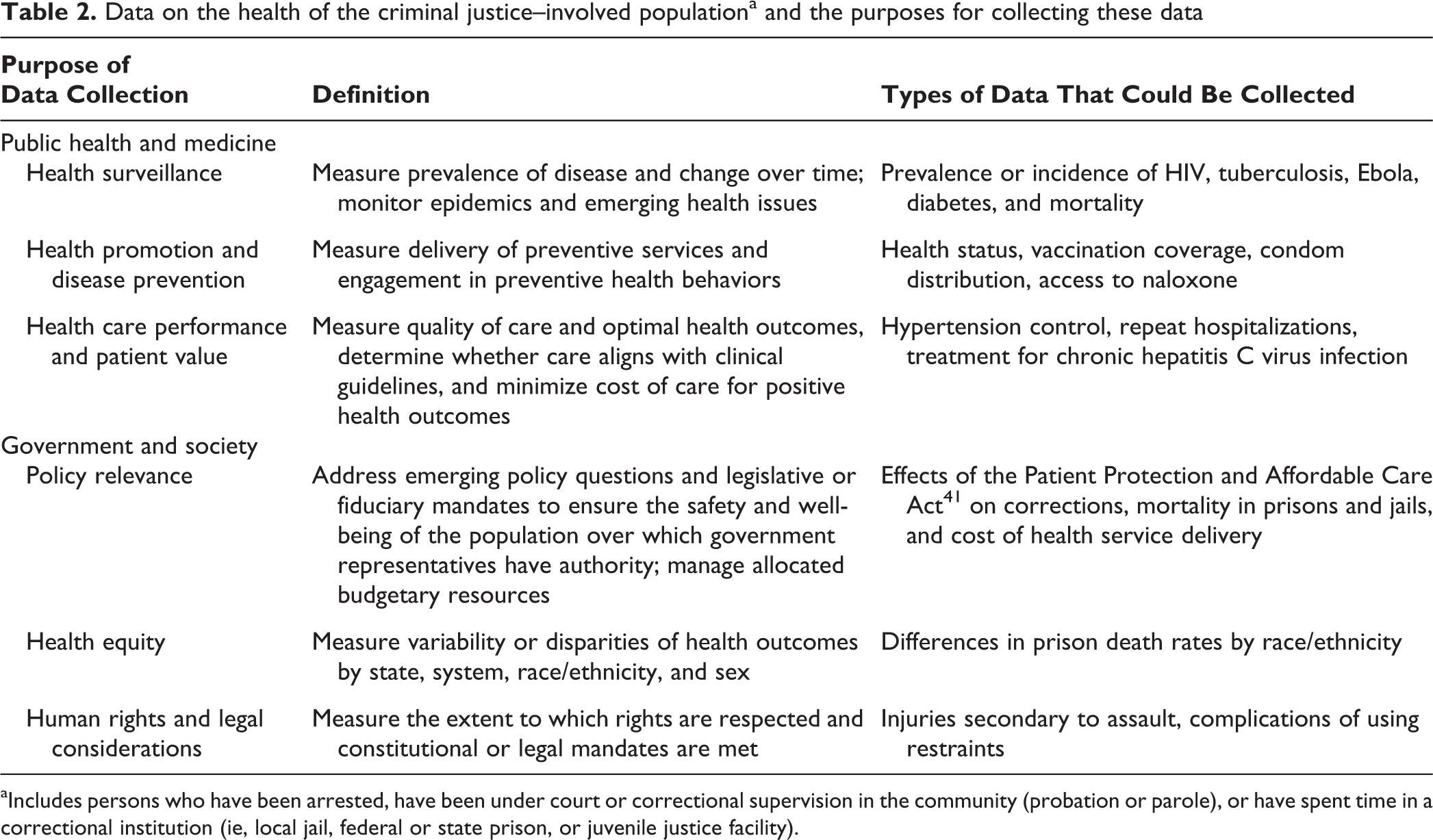
aIncludes persons who have been arrested, have been under court or correctional supervision in the community (probation or parole), or have spent time in a correctional institution (ie, local jail, federal or state prison, or juvenile justice facility).
Collecting Data for the Needs of Public Health and Medicine
Health surveillance
Surveillance of morbidity and mortality is a key function of national public health data collection and is particularly relevant for the justice-involved population. Examples of existing health surveillance data collection in this population include annual surveys of HIV/AIDS prevalence and deaths among incarcerated persons 1,4 and periodic surveys of the prevalence of other chronic medical conditions, behavioral health conditions, and sexually transmitted infections conducted by the Bureau of Justice Statistics. 2,42 Although the Centers for Disease Control and Prevention does not conduct ongoing health surveillance of the justice-involved population, it has released surveillance reports on outbreaks of HIV, tuberculosis, methicillin-resistant Staphylococcus aureus, and hepatitis B virus infection in correctional facilities, 43 -46 and it has worked with the Bureau of Justice Statistics to describe the delivery of prison health services. 3
Surveillance data help public health practitioners identify the health risks faced by the criminal justice–involved population in different settings, such as the incidence of arrest-related injuries and deaths, acute illness and deaths in correctional facilities, and hospitalizations and deaths on release. 47 In addition, surveillance data can add precision to population-wide estimates of disease prevalence because conditions that disproportionately affect this population, such as HCV infection, may be underestimated in surveys of noninstitutionalized individuals. 32 Ultimately, surveillance data can inform the development and implementation of preventive interventions, disease-containment efforts, proportionate and equitable resource allocation, and the acquisition of specialized public health and medical expertise to work in criminal justice settings.
Selecting which conditions and events to monitor—and which population(s) to sample—should be driven by knowledge gaps, burden of disease, costs of care, special requirements for disease containment, and outcome severity. For jails and prisons, surveillance is particularly important for monitoring new or emerging diseases that require planning and response. For example, preventing transmission of tuberculosis requires special screening, testing, and isolation in correctional settings. Surveillance is also important for common and severe outcomes in correctional settings, such as self-harm and suicide.
Health promotion and disease prevention
Data collection focused on health promotion and disease prevention measures health conditions that can be prevented, managed, treated, or contained, as well as the delivery of preventive health services, overall health status, health-related quality of life, and health behaviors that can prevent or reduce morbidity and mortality (eg, exercise and harm reduction). Collecting data on health promotion and disease prevention in the justice-involved population is important to public health because the benefits of preventive activities accrue as persons move between criminal justice and community settings. Persons in correctional facilities may have had poor access to preventive services in the community, making correctional health services the de facto providers for their preventive care needs. 48
Examples of data that have been collected to support health promotion and disease prevention in justice-involved populations include providing hepatitis B virus vaccination and HCV testing. 2,13,49 However, national surveys of other health promotion and disease prevention activities, such as cancer screening and other vaccinations, are lacking.
Health promotion and disease prevention data could be used to help correctional health administrators and providers identify opportunities to improve the health of persons in correctional facilities. For example, documenting low HCV screening rates in prisons through national data collection could drive efforts to expand HCV screening at prison admission through correctional health care provider training and policies. Because almost all incarcerated persons return to the community after incarceration, the resultant increase in HCV screening could ultimately result in a public health benefit by leading to more individuals being aware of their HCV status and seeking treatment.
However, correctional facilities participating in health promotion and disease prevention–oriented data collection may be concerned that such data will identify areas that need improvement without leading to additional funding to address them. This concern could be particularly salient for facilities with short stays (eg, jails) and for some health promotion and disease prevention activities with a long latency between the activity and potential individual or public health benefits (eg, HCV screening). Because of such concerns, collecting data on health promotion and disease prevention activities should focus on activities supported with strong evidence (eg, lipid disorders, diabetes, and cervical cancer screening), information on barriers to the delivery of health promotion and disease prevention activities (eg, cost, attitudes of custody staff members), and evaluation of whether such activities improve the health of the communities to which incarcerated persons return.
Health care performance and patient value
Data collection focused on health care performance and patient value would include data on health service delivery costs, processes, and rates of use across the spectrum of criminal justice settings, as well as outcomes. Consistent with the purpose of measuring health care performance and patient value, efforts have been made to collect data on the costs of correctional health care. For example, the Bureau of Justice Statistics used the US Census Bureau Annual Survey of State Government Finances to estimate state prison medical costs in 2001 and 2008. 50 These efforts highlight the myriad ways correctional facilities measure the costs of health services, either by facility or by system, as a part of the general operating budget or as a separate line item. The Pew Charitable Trusts, in partnership with the Vera Institute of Justice, reported on prison health care spending in fiscal year 2015. 51 To generate accurate national estimates, various models of paying for contracted health care services in the criminal justice system (eg, capitation, a per-person payment model, or cost-plus, a fee-for-service plus management charge) 51 need to be accounted for. Furthermore, generating accurate national cost estimates is complex because care for justice-involved populations may involve multiple types of services, providers, and payer units. Ideally, costs should be measured during a care cycle and include measurements of resources shared across facilities and the community.
Performance-focused data collection is important for the justice-involved population for at least 3 reasons. First, payers, including local and federal governments, have an interest in knowing whether purchased services are of high quality. Second, performance data have the potential to drive improvements in the health of, and delivery of health services to, persons in correctional institutions and potentially benefit the communities to which they return. Third, the data may help correctional health administrators improve the efficiency of service provision, program design, program evaluation, and resource allocation.
Patient value, which involves maximizing the health benefits of a given health care investment, is emphasized in the general population 52 and is important in the justice-involved population. Value as the primary purpose for collecting data necessitates assessing not only the costs of care but also its associated benefits, both in direct financial terms and with established metrics, such as quality-adjusted life years (a measure of the length of life in a given state of health). Measuring health care quality and health service overuse, underuse, and misuse is also consistent with a patient-value purpose. For example, the correctional health patient safety indicators selected by Stern et al 53 (eg, access to prenatal care, provider competency evaluation, monitoring medication expiration dates) and the correctional health indicators selected by using a modified Delphi method conducted by Asch et al 54 (eg, receipt of colorectal cancer screening in appropriate age groups, number of suicides) were quality-oriented performance measures for incarcerated persons. Many quality measures assess processes rather than outcomes, 52 making value difficult to measure. Thus, selecting value as the focus of data collection would require including outcome measures in addition to costs.
Collecting Data for the Needs of Government and Society in General
Policy relevance
Collecting data on the health of the criminal justice–involved population can help answer important policy questions; assess the effects of local, national, and international criminal justice and health policies on this population; and measure adherence to legislative mandates and budgetary constraints. One example of a policy-relevant study that used national prison mortality data is a study of the effects of tobacco bans in prison on tobacco-related deaths in prison. 55 Tobacco bans were rapidly implemented in US correctional facilities in the early 2000s, but their effectiveness was unknown. Mortality data from the Bureau of Justice Statistics were used to assess the impact of these bans on mortality rates in prisons and found that smoking bans were associated with reductions in the number of deaths due to smoking-related causes. 55 Policy-focused data collection could evaluate the effects of the Patient Protection and Affordable Care Act 41 and Medicaid expansion on the insurance status of the criminal justice–involved population in the new US health insurance marketplace. Other policy-relevant evaluations include assessing the effects of new payment models for correctional health care, various models of governance for health care delivery in jails and prisons, and the increasing use of electronic health records in these settings.
To conduct policy-focused evaluations, national data on the insurance status and health care use of the criminal justice–involved population are needed. Further, data need to be collected regularly, at appropriate times, and be consistently gathered over time and across sites before and after policy implementation. Extracting data from administrative or clinical records routinely collected for other purposes (eg, electronic health records) is an emerging approach to obtaining such data. However, these data sources require local expertise to ensure that the data fields are capturing meaningful data and that efforts are coordinated across facilities so that the variables are similarly collected and coded. Thus, selecting policy as the primary rationale for data collection should encourage the groups collecting such data to develop tailored data infrastructure and expertise to support this goal.
Health equity
Concerns that criminal justice involvement may exacerbate disparities in health outcomes by race and ethnicity, sex, or other individual and social characteristics have led researchers and policy makers to call for collecting data to assess health equity among the justice-involved population. 10,23,56 Defining, measuring, and reducing health disparities, particularly racial and ethnic health disparities, in the general population have been active areas of research 57,58 and are also relevant in the justice-involved population. Incarceration rates differ by race and ethnicity, 59,60 and incarceration and other criminal justice contacts are linked to overall health disparities. 23,56,61 -65 Yet little is known about such disparities in this population. Data on correctional health and health service experiences would inform society-wide responses to such disparities. Emphasizing health equity as a rationale for data collection may be important to policy makers and public health stakeholders interested in reducing such disparities.
Health equity data include measures of variability or disparities in health outcomes across populations and settings, such as populations in jails and prisons, men and women, incarcerated persons and the general population, and incarcerated persons in various countries. Given the constraints of providing care in a closed facility (eg, limited patient choice in providers, increased risk of transmitting infection) and differences in the underlying risk of disease among persons in correctional facilities (ie, high prevalence of infectious diseases), the care provided in jails and prison will not be the same as in the community. Thus, tuberculosis screening is universal in some jails and prisons but rare in community-based primary care clinics. Because of these differences, ethicists have called for equivalent access to care and similar outcomes. 66 Rule 24.1 of the United Nations Standard Minimum Rules for the Treatment of Prisoners (ie, the Mandela Rules)—often referred to as the “principle of equivalence”—states that “prisoners should enjoy the same standards of health care available in the community.” 67 Thus, the Prison Health Performance and Quality Indicators system in the United Kingdom sought to measure whether health care in prison was equivalent to health care in the community; “equivalence of care” did not mean the same care but care equivalent in terms of outcomes and quality of care. 17,68 Thus, data collection with a health equity focus should permit comparisons between health service experiences across diverse criminal justice settings and the community, accounting for differences in complexity of health problems between correctional and community settings. A focus on health equity would also require collecting adequate, accurate data across systems or populations suitable for stratified analyses by selected characteristics (eg, race and ethnicity, indigenous status, and age).
In the United States, focusing on health equity would prioritize indicators that measure progress toward national health priorities, such as those described in Healthy People 2020, 69 which is aimed at increasing the number of persons with health insurance and reducing the number of adults who use tobacco. Aligning these measures with the health priorities of the general population will ensure that the measures are also relevant to public health. To permit comparisons of the US justice-involved population to the justice-involved population in other countries, groups may select indicators related to global health priorities, such as the Good Health and Well-Being and the Reduced Inequalities goals of the United Nations’ Sustainable Development Goals. 70
Human rights and legal considerations
Persons in the criminal justice–involved population are under government authority and have had certain rights revoked, increasing the salience of a human rights and legal rationale for collecting data on the health of this population. Data on human rights and legal considerations could be used to evaluate correctional facilities’ adherence to laws governing environmental conditions (eg, temperatures in housing units, crowding) that influence health, well-being, and access to care. Health measures consistent with a human rights and legal focus include the number of injuries incurred through the use of seclusion or restraint for persons who have mental health disorders and caused by force during police encounters. Although the United States currently does not collect such data, the World Health Organization’s Regional Office for Europe has sought to describe and improve the health of incarcerated persons based on human rights considerations. 15,25 As another example, the Health in Prisons European Database 15 has measured compliance with ethical recommendations that prison health services be independent of prison administrative functions to avoid potential conflicts between professional medical standards and the legal functions of prisons. 71 The use of international standards to guide the development and selection of indicators to address human rights and legal considerations for the criminal justice–involved population 67,71,72 would permit cross-national comparisons in the health and health service experiences of justice-involved populations. For example, the standard on access to specialty care 67 could inform the development of measures on the availability of specialty care in prisons. As another example, Article 37 of the United Nations Convention on the Rights of the Child states that arrest, detention, and imprisonment of children are measures of “last resort.” 73 Under a human rights focus, data collection systems should cover young persons in detention and persons supervised by the criminal justice system but still living in the community and measure efforts to divert at-risk young persons from entering the justice system. 74
Principles of Data Collection
We identified the following 5 fundamental principles of data collection consistent with sound public health practice to consider when collecting data on the health of persons in the criminal justice system: (1) ensure reliable and valid data collection and measurement, (2) use measures of evidence-based health practices, (3) align measures and approaches with general population data collection and across regions and settings, (4) promote transparency while maintaining trust and ensuring individual privacy, and (5) encourage greater patient-centeredness.
Ensuring reliable and valid data on persons in the criminal justice system
Representativeness: Conduct a census or apply a replicable sampling strategy that produces representative data and is large enough to produce precise, reliable estimates.
Basic epidemiologic principles: Collect numerator and denominator data consistent with basic epidemiologic concepts, such as prevalence and incidence.
Specificity: Ensure adequate specificity in the measures used (eg, self-report, clinical, billing, laboratory, or biomarker data) to reflect clinically meaningful categories, such as active and latent infections (eg, tuberculosis) and current and historical conditions (eg, injuries, cancer, asthma, hepatitis C virus infection).
Comparability: Collect or ensure access to comparator data from other populations (eg, the non-incarcerated population) to contextualize findings.
Stability over time: Ensure repeated, consistent, and reliable measurement at multiple appropriate intervals (eg, at prison entry and release, yearly, every decade) to detect meaningful changes.
Ensure Reliable and Valid Data Collection and Measurement
Valid data collection is achieved by adhering to the 5 principles listed previously and ensuring representativeness, basic epidemiologic principles, specificity, comparability, and stability over time (Box). These principles are not intended to be comprehensive or universal, and other sources provide greater detail on survey methodologies intended to improve and evaluate national indicators. 75 Adopting the standard of representativeness would provide more consistent data collection across federal, state, and county correctional facilities.
Use Measures of Evidence-Based Health Practices
Agencies should prioritize collecting data on health measures, particularly performance measures, proven to have high value in the general, noninstitutionalized population; the criminal justice–involved population; or both and that are based on evidence-based care guidelines, such as the US Preventive Services Task Force recommendations. 76 For example, in the National Health Interview Survey and the Behavioral Risk Factor Surveillance System, some clinical guidelines, such as colon cancer screening or aspirin use for persons with cardiovascular disease, have been adopted as general population indicators. 77,78 For the criminal justice–involved population, however, one challenge to using measures of evidence-based health practices is that incarcerated persons are often excluded from clinical trials, so it is not always clear to what extent evidence can be applied to this population. 34,35
Align Measures and Approaches With General Population Data Collection and Across Regions and Settings
Several health measures used in the criminal justice–involved population, including health care performance, patient value, and health equity, should be identical or nearly so to those used in the general population to facilitate comparisons. To the extent possible in correctional facilities, the Bureau of Justice Statistics has aligned measures of self-reported health to measures collected in the National Health Interview Survey 77,79 and measures of disability to the question sets of the Washington Group on Disability Statistics. 80 Aligning measures across countries permits cross-national comparisons. 81 Furthermore, denominator data (eg, person-years) and data required to standardize measures by age, sex, and race/ethnicity need to be collected consistently across data-collection efforts.
To address the cost and personnel requirements of collecting data on health in jails and prisons, groups conducting the surveys (eg, government agencies, nongovernmental organizations, academia) should align their requests for data with other groups collecting similar data.
Promote Transparency While Maintaining Trust and Ensuring Individual Privacy
Transparency is consistent with the ideals of a democratic government and is likely to enhance public trust. Because correctional health services are publicly funded, legal scholars have called for increased transparency, particularly with regard to the operation of private prisons, including prison health care. 82 Under a transparency principle, providing routine public reporting of aggregate data on the criminal justice–involved population is important to permit independent evaluation while protecting participant privacy. With appropriate privacy protections and infrastructure (eg, distributed data networks that permit analysis of electronic health data resources across sites), 83 analyses have been conducted across correctional health systems. 35
Transparency is important for populations traditionally overrepresented in criminal justice settings and that may have experienced discrimination, bias, or abuse. Transparency can highlight areas in which correctional health service experiences and outcomes are better or worse than in the community, consistent with the principle of health equity, and provide insight into improving outcomes for both this and the general population, consistent with the principles of quality health care performance and patient values. The need for transparency, however, must be balanced with the need to maintain patient privacy and should address concerns about how data on site- or system-specific outcomes might be used by the media and in litigation.
Encourage Greater Patient-Centeredness
The Institute of Medicine defines patient-centered care as “care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions.” 84 Consistent with the principle of human rights, data collection should be relevant to patients and their families and caregivers, that is, to the stakeholders most affected by criminal justice health care. 85 To support a principle of patient-centeredness, the criminal justice–involved population should be included in the process of selecting measures, developing data-collection protocols, interpreting results, and identifying forums for disseminating findings.
Summary
Fulfilling the 6 purposes for collecting data on the health and health service experiences of the criminal justice–involved population and adhering to the 5 data-collection principles should result in valid, reliable, and useful data to help understand the health needs and characteristics of this population. Such a process should yield data that allow comparisons with the general population, guide the organization of health services, help assess outcomes, evaluate the impact of policies, and, ultimately, improve public health. In addition, these data have the potential to improve the comprehensiveness and accuracy of estimates based on general-population household surveys and other national public health data collection. Finally, such a process should promote public trust and highlight areas of both high and low performance on health quality metrics.
Although we considered the perspectives of diverse stakeholders, such as incarcerated persons, correctional administrators, and legislators, we (the authors) represent the fields of health professions, public health, and justice statistics. To better integrate the perspectives of diverse stakeholders, future research should formally engage these stakeholders and apply qualitative approaches to ensure that the full spectrum of stakeholder views is represented in future data collections. Research should examine barriers that may limit the ability to collect comprehensive data on persons in the criminal justice system, including financial, structural, historical, and cultural barriers. This research should also identify policy strategies to address these barriers.
Each group collecting health data on this population should identify its primary purpose for collecting data to ensure that the data elements support this purpose, to avoid duplicate efforts, and to permit the data to be evaluated against its goals. Given the large number of potential health measures, identifying the primary purposes for collecting data can focus the scope of the data collected and inform by what means and how often each measure is assessed. Various groups should also consider coordinating data collection efforts to maximize coverage of diverse populations and settings.
Footnotes
Acknowledgments
The authors acknowledge the helpful input of William J. Sabol, PhD; Lars Møller, MD, DrMSc; Ingrid Johnston; Éamonn O’Moore, MB, BCh, BAO, MPH; and Fiona G. Kouyoumdjian, MD, PhD, MPH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, or publication of this article: This article was commissioned by the National Academies of Sciences, Engineering, and Medicine Standing Committee on Improving Collection of Indicators of Criminal Justice System Involvement in Population Health Data Programs on behalf of the US Department of Health and Human Services (HHS). Opinions and statements included in this article are not necessarily adopted, endorsed, or verified as accurate by the National Academies of Sciences, Engineering, and Medicine or any other organization or agency that provided support for the project. Support for the Standing Committee was provided by HHS through an interagency agreement with the National Science Foundation (No. SES-1 024 012). Support for portions of this project was provided by the US Department of Justice, Bureau of Justice Statistics under Bureau of Justice Statistics Visiting Fellowship Program grant 2011-BJ-CX-K073 and Intergovernmental Personnel Agreement 2016R2R7943. Stuart Kinner is supported by the Australian National Health and Medical Research Council Senior Research Fellowship APP1078168.