
Abstract
Objectives:
The effect of incarceration on HIV risk–related behaviors among at-risk heterosexual men is understudied. The objective of our study was to examine the association between incarceration and HIV risk–related behaviors among a sample of predominantly non-Hispanic black and Hispanic heterosexual men residing in urban areas in the United States with a high prevalence of AIDS.
Methods:
We analyzed data from the 2013 National HIV Behavioral Surveillance system on 5321 at-risk heterosexual men using log-linked Poisson regression models, adjusted for demographic characteristics and clustered on city.
Results:
Of 5321 men, 1417 (26.6%) had recently been incarcerated (in the past 12 months), 2781 (52.3%) had ever been incarcerated but not in the past 12 months, and 1123 (21.1%) had never been incarcerated. Recent incarceration was associated with multiple casual female sexual partners (adjusted prevalence ratio [aPR] = 1.23; 95% confidence interval [CI], 1.05-1.44), condomless sex with multiple female sexual partners (aPR = 1.32; 95% CI, 1.06-1.66), injection drug use (aPR = 3.75; 95% CI, 2.64-5.32), and having sexual partners who were more likely to have ever injected drugs (aPR = 1.84; 95% CI, 1.48-2.28), been incarcerated (aPR = 2.28; 95% CI, 2.01-2.59), or had a concurrent sexual partner (aPR = 1.08; 95% CI, 1.05-1.11), as compared with never-incarcerated men.
Conclusions:
Incarceration history was associated with HIV risk–related behaviors among heterosexual men from urban areas in the United States. Correctional rehabilitation initiatives are needed to promote strategies that mitigate HIV risk–related behaviors and promote healthy reentry into communities among heterosexual men at high risk for HIV.
In the United States, HIV infection disproportionately affects black and Hispanic/Latino persons of low socioeconomic status (SES). 1 Black and Hispanic/Latino men of low SES from urban communities are also disproportionately incarcerated in the United States. 2,3 In 2016, of 1 106 096 male state and federal prisoners, 34.9% were non-Hispanic black, 21.1% were Hispanic/Latino, and 30.6% were non-Hispanic white (the remaining 13.4% were of another race/ethnicity than those listed or identified themselves as being multiracial). 4 In comparison, according to the US Census Bureau’s American Community Survey, non-Hispanic black and Hispanic/Latino persons compose 12% and 18% of the general US population, respectively, and non-Hispanic white people compose 61% of the population. 5
From 2010 to 2015, the HIV infection rate among state and federal inmates declined from 1.8% to 1.3%, but the rates were still about 3 times higher than the rate in the general US population (0.5%). 6,7 During that same period, the prevalence of HIV infection in some state prisons in Florida, Louisiana, and New York was >3%, which was 10 times the rate in the general US population. 6,7 Almost all inmates with HIV become infected while in the community, where they engage in risk-related behaviors and encounter barriers to accessing prevention and treatment resources. 8,9
HIV research among men largely focuses on men who have sex with men (MSM) or men who inject drugs, whereas the HIV risk among heterosexual men in the United States is largely understudied. 9 -11 Research suggests that the HIV risk for heterosexual men is a major concern in low-income, urban black communities, where rates of sexually transmitted infections (STIs) and HIV are disproportionately high. 9 Of the 3037 new HIV cases attributed to heterosexual contact among men in 2016, black men accounted for 63% (n = 1926) and Hispanic/Latino men accounted for 19% (n = 581) of cases. 12
Incarceration can increase the risk of HIV among heterosexual men in several ways. 13 -17 Incarceration engenders housing instability, a well-known structural barrier to HIV prevention efforts, 18,19 and disrupts sexual networks, which increases the occurrence of concurrent and multiple sexual relationships, 20 STIs, and syringe sharing. 16,21,22 A 2014 study of black patients attending an STI clinic found that a history of incarceration and unstable housing interacted to increase the risk of having multiple sexual partners and condomless sex. 23 Recidivism is common, so inmates frequently move between prison or jail and their home communities, which may exacerbate social and economic instability. 24 Still, studies on incarceration and HIV risk among low-income heterosexual men in the United States are scant. 8 Understanding the prevalence of incarceration and its association with sexual and substance-use behaviors, health services use, and HIV infection among this population is important.
The objective of our study was to use recent national behavioral surveillance data to examine the association between incarceration and HIV risk–related behaviors among heterosexual men from urban areas in the United States with a high prevalence of AIDS, determine the prevalence of past and recent incarceration among heterosexual men from these areas and compare HIV-related behaviors and HIV infection rates among men who have a history of incarceration with risk behaviors and HIV rates of men without such a history.
Methods
Sample and Procedures
We used data from the 2013 National HIV Behavioral Surveillance (NHBS) system, 25 which surveys heterosexual men and women at increased risk for HIV infection from high-poverty communities in 20 metropolitan statistical areas with a high prevalence of AIDS (Atlanta, Georgia; Baltimore, Maryland; Boston, Massachusetts; Chicago, Illinois; Dallas, Texas; Denver, Colorado; Detroit, Michigan; Houston, Texas; Los Angeles, California; Miami, Florida; Nassau-Suffolk, New York; New Orleans, Louisiana; New York, New York; Newark, New Jersey; Philadelphia, Pennsylvania; San Diego, California; San Francisco, California; San Juan, Puerto Rico; Seattle, Washington; and Washington, DC). Details on recruitment methods are provided elsewhere. 26
Respondents were recruited using respondent-driven sampling, a peer-referral, social network–based sampling method primarily used to study hard-to-reach populations. 27 Eligibility was restricted to adults aged 18-60 who lived in the participating metropolitan statistical areas, completed the survey in English or Spanish, and reported vaginal or anal sex with an opposite-sex partner in the previous 12 months. The recruitment process continued until the sample size of heterosexual men and women of low SES was reached (n = 10 682) or the sampling period ended. Low SES was defined as having completed no more than a high school education or having a household income at or below the federal poverty level. 28 Details on recruitment methods are provided elsewhere. 12
After we obtained informed consent, we interviewed 8104 male and female respondents about sexual behaviors, drug use, HIV testing, and use of HIV prevention services by using a standardized, anonymous questionnaire. Interviewers administered the survey in person by using a portable computer. The survey included questions about respondents’ demographic characteristics, sexual and drug-use behaviors, HIV testing history, hepatitis vaccination status, STI diagnoses, and use of HIV behavioral interventions. Interviews averaged 32 minutes, and survey participants received $25 in cash or a gift certificate for the interview, as well as an additional $25 if they agreed to the HIV test.
All men and women who agreed to be interviewed were offered anonymous HIV testing, regardless of self-reported HIV infection status. Testing was performed by collecting blood or oral specimens for either rapid testing in the field followed by laboratory confirmation or by laboratory-based testing. We considered a nonreactive rapid test result to be a definitive negative result and a reactive (preliminary positive) rapid test result to be a definitive positive result only when confirmed by supplemental laboratory testing (eg, Western blot, immunofluorescence assay, or nucleic acid amplification test).
The present study focused on the outcomes of male NHBS participants. Local institutional review boards in each participating city approved all NHBS activities, and the Centers for Disease Control and Prevention approved the protocol.
Variables
Incarceration was defined as being held in a detention center, jail, or prison for more than 24 hours. Respondents were classified in 3 mutually exclusive categories: “never incarcerated,” “recently incarcerated” if detained during the previous 12 months, or “incarcerated in the past” if detained more than 1 year before the interview. This definition included men who had served a prison sentence and men who were detained for various reasons but against whom criminal charges may not have been filed.
Age, race/ethnicity, education, poverty, homelessness, and region of residence were regarded as potential confounders. Men who self-identified as American Indian/Alaska Native, Asian, Native Hawaiian or other Pacific Islander, white, and of multiple races were grouped as “non-Hispanic other” given the small sizes of each group.
Outcomes included the following: sexual risk behaviors with female partners (total number of female sexual partners, casual sexual partners, and casual condomless vaginal sexual partners), sex with another man, characteristics of most recent sexual partner (ever injected drugs, ever incarcerated, ever had a concurrent sexual partner), non-injection drug use, HIV testing, HIV status (based on the results of the test offered during the interview), and any STI diagnosis, all within the previous 12 months. Casual sexual partners were defined as women with whom respondents reported having vaginal, oral, or anal sex but to whom they did not feel committed. We dichotomized continuous responses into 1 or 2 partners and ≥3 partners. We based a positive history of STI on self-reports of receiving a diagnosis of chlamydia, gonorrhea, or syphilis during the previous 12 months. We recoded responses of “definitely did/probably did” as “yes” and “definitely did not/probably did not” as “no.” We examined the type of facility where the respondent reported receiving his most recent HIV test and whether recently jailed respondents reported being tested for HIV while incarcerated.
Statistical Methods
We analyzed data only from 5321 at-risk men who (1) had a valid HIV test result and (2) completed responses for all variables in the analysis. Data were based on respondent-driven sampling, in which respondents recruit other potential respondents in their friendship networks, forming recruitment chains in which respondents are clustered by peer groups. Due to the respondent-driven sampling structure of the data, observations in the same network were not independent. To account for respondent-driven sampling, we used a separate, log-linked Poisson regression model with generalized estimating equations with an exchangeable correlation matrix, 29,30 accounting for the non-independence of network data by clustering on recruitment chain, 31,32 to assess the association between incarceration history and each group of outcomes, that is, sociodemographic characteristics and HIV risk–related behaviors. An exchangeable correlation matrix is based on the assumption that all variances and covariances are equal in a model. We included respondents’ city and personal social network size in each model to adjust for variation within cities and intraclass correlations associated with respondent-driven sampling. We assessed differences in sociodemographic characteristics by using the Wald χ2 test, with P < .05 considered significant.
To assess the independent association between incarceration and each outcome, we estimated adjusted prevalence ratios (aPRs) and 95% confidence intervals (CIs) by including in each model the sociodemographic characteristics associated with incarceration in the Wald χ2 test. We included the following characteristics: race/ethnicity (non-Hispanic black, Hispanic, non-Hispanic other), age group (18-24, 25-29, 30-39, 40-49, ≥50), education (<high school diploma, high school diploma, at least some college), and income relative to the federal poverty level. We included the same confounders in all models. For the outcome of the most recent HIV test, we excluded 80 respondents who tested positive more than 12 months before the interview and were aware of their status. We used a 2-tailed test of significance, with α < .05 considered significant. We used SAS version 9.4 33 to conduct all statistical analyses.
Results
Of the 5321 at-risk heterosexual men in the analysis, 4198 (78.9%) had been incarcerated, including 1417 (26.6%) who were recently incarcerated and 2781 (52.3%) who were incarcerated in the past (Table 1). The following sociodemographic groups of men had the highest percentages of recent incarceration: non-Hispanic other (n = 173/550, 31.5%), aged 25-29 (n = 182/521, 34.9%), homeless (n = 629/1734, 36.7%), men with <high school diploma (n = 487/1571, 31.0%), and men with annual income at or below the federal poverty level (n = 1133/4076, 27.8%) (Table 1). Of 1417 recently incarcerated men, 524 (36.9%) reported receiving an HIV test while incarcerated.
Incarceration status of heterosexual men at increased risk of HIV infection, by sociodemographic characteristics, National HIV Behavioral Surveillance system, 20 US cities, 2013a
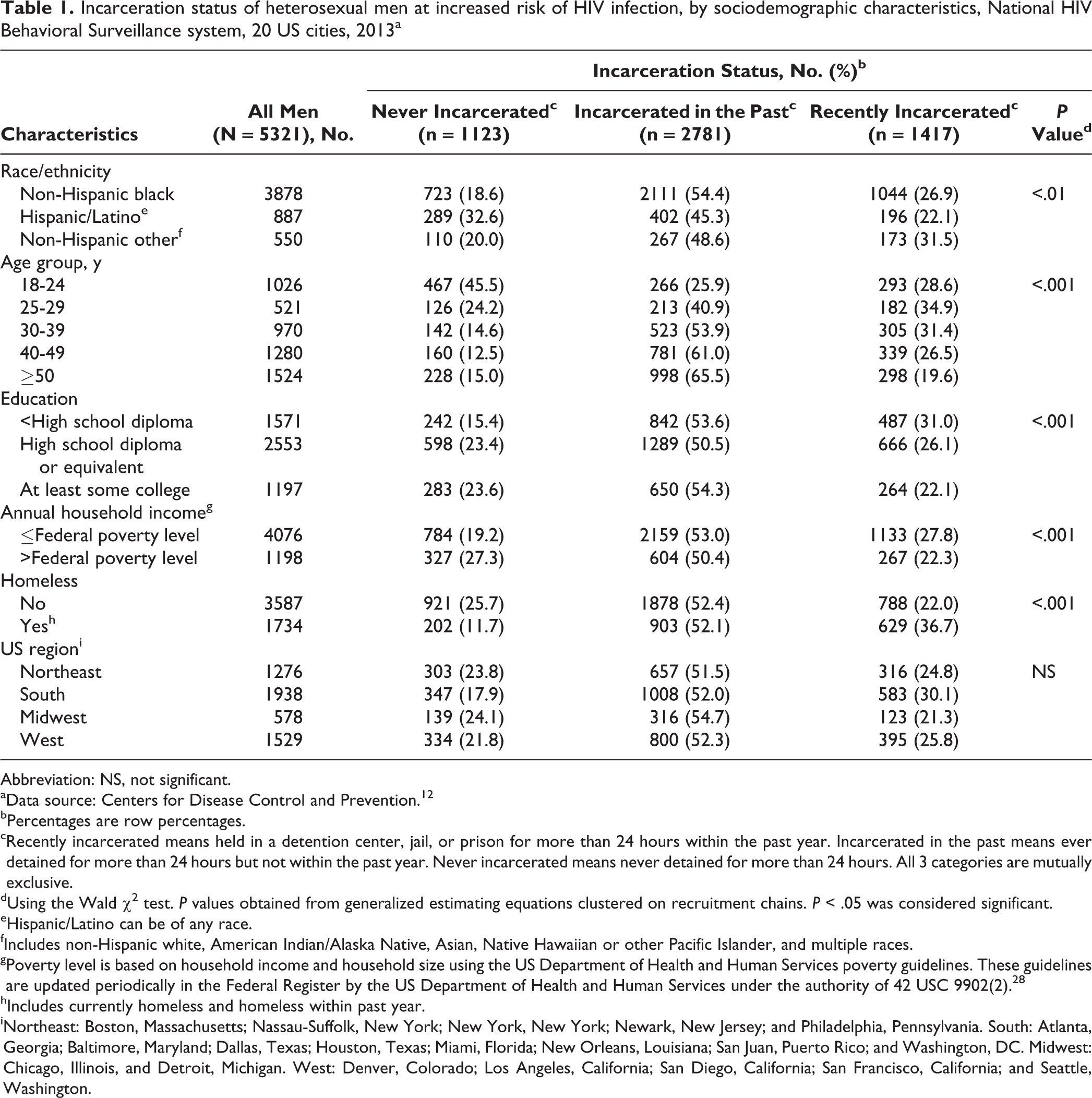
Abbreviation: NS, not significant.
aData source: Centers for Disease Control and Prevention. 12
bPercentages are row percentages.
cRecently incarcerated means held in a detention center, jail, or prison for more than 24 hours within the past year. Incarcerated in the past means ever detained for more than 24 hours but not within the past year. Never incarcerated means never detained for more than 24 hours. All 3 categories are mutually exclusive.
dUsing the Wald χ2 test. P values obtained from generalized estimating equations clustered on recruitment chains. P < .05 was considered significant.
eHispanic/Latino can be of any race.
fIncludes non-Hispanic white, American Indian/Alaska Native, Asian, Native Hawaiian or other Pacific Islander, and multiple races.
gPoverty level is based on household income and household size using the US Department of Health and Human Services poverty guidelines. These guidelines are updated periodically in the Federal Register by the US Department of Health and Human Services under the authority of 42 USC 9902(2). 28
hIncludes currently homeless and homeless within past year.
iNortheast: Boston, Massachusetts; Nassau-Suffolk, New York; New York, New York; Newark, New Jersey; and Philadelphia, Pennsylvania. South: Atlanta, Georgia; Baltimore, Maryland; Dallas, Texas; Houston, Texas; Miami, Florida; New Orleans, Louisiana; San Juan, Puerto Rico; and Washington, DC. Midwest: Chicago, Illinois, and Detroit, Michigan. West: Denver, Colorado; Los Angeles, California; San Diego, California; San Francisco, California; and Seattle, Washington.
Individual Risk-Related Behaviors and HIV Prevalence
Compared with never-incarcerated men, men who had been incarcerated (in the past or recently) were significantly more likely to report having ≥3 casual female sexual partners, engaging in injection drug use, having an STI diagnosis, and being tested for HIV in the past 12 months, after adjusting for other characteristics (Table 2). Compared with never-incarcerated men, men incarcerated in the past (aPR = 1.21; 95% CI, 1.08-1.35) and recently incarcerated men (aPR = 1.23; 95% CI, 1.05-1.44) were significantly more likely to report having multiple casual female sexual partners in the past 12 months. Similarly, recently incarcerated men were significantly more likely than never-incarcerated men to report multiple casual condomless vaginal sexual partners in the past 12 months (aPR = 1.32; 95% CI, 1.06-1.66). Men incarcerated in the past (aPR = 2.14; 95% CI, 1.63-2.81) and recently incarcerated men (aPR = 3.75; 95% CI, 2.64-5.32) were significantly more likely than never-incarcerated men to report injection drug use in the past 12 months.
Selected HIV risk–related outcomes of heterosexual men at increased risk of HIV infection, by incarceration status, National HIV Behavioral Surveillance system, 20 US cities, 2013a
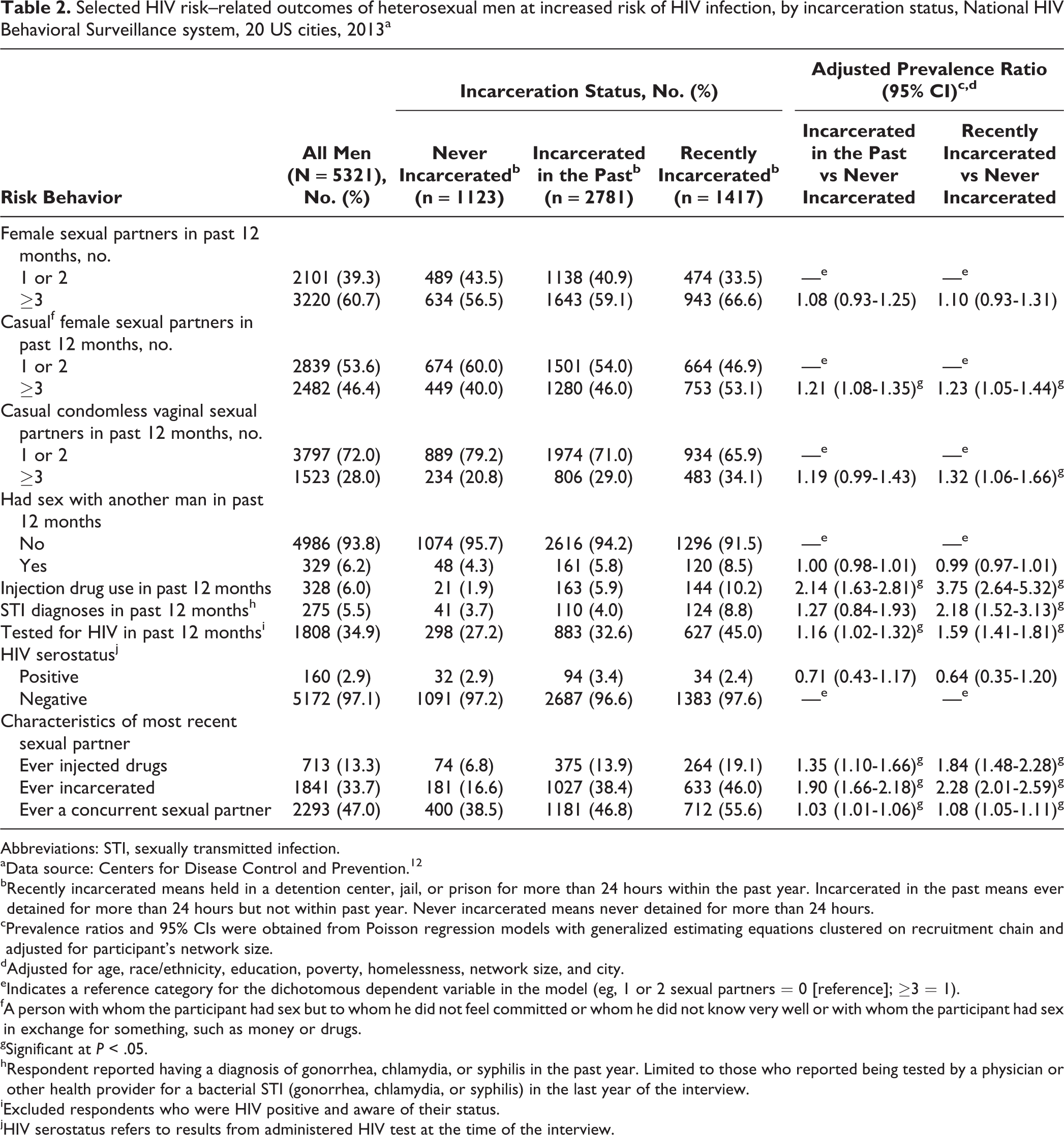
Abbreviations: STI, sexually transmitted infection.
aData source: Centers for Disease Control and Prevention. 12
bRecently incarcerated means held in a detention center, jail, or prison for more than 24 hours within the past year. Incarcerated in the past means ever detained for more than 24 hours but not within past year. Never incarcerated means never detained for more than 24 hours.
cPrevalence ratios and 95% CIs were obtained from Poisson regression models with generalized estimating equations clustered on recruitment chain and adjusted for participant’s network size.
dAdjusted for age, race/ethnicity, education, poverty, homelessness, network size, and city.
eIndicates a reference category for the dichotomous dependent variable in the model (eg, 1 or 2 sexual partners = 0 [reference]; ≥3 = 1).
fA person with whom the participant had sex but to whom he did not feel committed or whom he did not know very well or with whom the participant had sex in exchange for something, such as money or drugs.
gSignificant at P < .05.
hRespondent reported having a diagnosis of gonorrhea, chlamydia, or syphilis in the past year. Limited to those who reported being tested by a physician or other health provider for a bacterial STI (gonorrhea, chlamydia, or syphilis) in the last year of the interview.
iExcluded respondents who were HIV positive and aware of their status.
jHIV serostatus refers to results from administered HIV test at the time of the interview.
Recently incarcerated men (aPR = 2.18; 95% CI, 1.52-3.13) and men incarcerated in the past (aPR = 1.27; 95% CI, 0.84-1.93) were significantly more likely than never-incarcerated men to report having an STI diagnosis, after adjusting for confounders. Men incarcerated in the past (aPR = 1.16; 95% CI, 1.02-1.32) and recently incarcerated men (aPR = 1.59; 95% CI, 1.41-1.81) were also significantly more likely than never-incarcerated men to report an HIV test in the previous 12 months. HIV prevalence did not differ significantly by incarceration history: never (n = 32, 2.9%), past (n = 94, 3.4%), and recent (n = 34, 2.4%).
Risk-Related Behaviors of the Most Recent Sexual Partner
Compared with never-incarcerated men, men incarcerated in the past and recently incarcerated men were significantly more likely to report having a sexual partner who ever injected drugs (incarcerated in the past: aPR = 1.35; 95% CI, 1.10-1.66; recently incarcerated: aPR = 1.84; 95% CI, 1.48-2.28); to report that their last sexual partner had been incarcerated (incarcerated in the past: aPR = 1.90; 95% CI, 1.66-2.18; recently incarcerated: aPR = 2.28; 95% CI, 2.01-2.59); and to report that their last sexual partner had a concurrent partner (incarcerated in the past: aPR = 1.03; 95% CI, 1.01-1.06; recently incarcerated: aPR = 1.08; 95% CI, 1.05-1.11) (Table 2).
Discussion
HIV prevalence did not differ between at-risk heterosexual men with a history of incarceration and men without a history of incarceration. Research shows that HIV risk–related behaviors differ by incarceration history 15,21 and that HIV and STI are associated with risk-related sexual behaviors. 16 However, we found no other study that directly measured HIV serostatus and tested for differences by incarceration history among noninstitutionalized men. A 2017 NHBS study of at-risk heterosexual women found an overall HIV prevalence of 4%; HIV prevalence was higher among recently incarcerated women than among never-incarcerated women. 34 A 2010 study using NHBS-MSM data found that HIV prevalence was 11% among black MSM and 3% among non-black MSM, but that study did not test for differences by incarceration history. 35 A 2012 study in Baltimore found that the prevalence of STI was 14% among recently incarcerated men, 7% among men incarcerated in the past, and 6% among never-incarcerated men. 36
Our findings indicate that additional studies are needed to measure the association between HIV serostatus and incarceration, with measures of duration of incarceration, reason for incarceration, and facility type (eg, jail or prison) among heterosexual men. The lack of association between HIV and incarceration, despite higher odds of risk-related behavior among heterosexual men who reported a history of incarceration, may be due to the role of gender in the sociocultural and biological context of HIV transmission. HIV risk–related behaviors overlap with culturally acceptable displays of male “bad behavior,” including substance use, multiple female sexual partners, and lack of care for health. 37 Heterosexual men with a history of incarceration may be more likely in general to engage in HIV risk–related behaviors than men without a history of incarceration. On the other hand, men are less likely to acquire HIV when exposed to the virus by a female partner rather than by a male partner when engaging in sexual risk-related behaviors. 37
This study extends the extant literature on incarceration and HIV risk–related behaviors by focusing on at-risk urban heterosexual men, an understudied and hard-to-reach population, and using data from a large national surveillance data set. Our results are consistent with previous findings on the association between incarceration history and concurrent sexual partnerships, 17,35,36,38 multiple sexual partnerships, 36,37,39 STIs, 36 condomless sex, 16,17,21,22,24 and injection drug use. 40 In addition, we found that heterosexual men with a history of incarceration are embedded in sexual networks of partners who are at risk of acquiring HIV. 41 Incarceration may thus introduce potential at-risk sexual partners into an individual’s sexual network when he or she enters the criminal justice system. 21,36
Social policies that reduce recidivism could directly reduce HIV incidence at the individual and community levels. 42 Incarceration often disrupts supportive social and economic systems, which can make adhering to HIV risk–reduction behaviors difficult. 43 Educational interventions in correctional settings are effective in reducing post-release risk behaviors among inmates. 44 For example, Project START is a Centers for Disease Control and Prevention–initiated client-centered intervention for young men being released from prison, with demonstrated efficacy in reducing sexual risk behaviors. Project START was tested at 8 prisons in 4 states (California, Mississippi, Rhode Island, and Wisconsin) and found to result in a 60% decrease in unprotected vaginal or anal sex among men who received an enhanced intervention that addressed community reentry needs, compared with men who did not receive the enhanced intervention. 45 Involvement in the criminal justice system is strongly linked with HIV risk among economically disadvantaged black and Hispanic/Latino men and has deleterious effects on their communities, including social and economic instability and perpetuating HIV transmission. 46
Strengths and Limitations
This study had several strengths. One strength was the community-based recruitment of at-risk heterosexual men through the NHBS and the use of a validated questionnaire assessing sexual- and drug use–related behaviors. A second strength was that the sampling scheme used by the NHBS allowed for appropriate behavioral risk factor surveillance within this population.
This analysis also had several limitations. First, the NHBS samples low-SES heterosexuals in metropolitan areas; as such, it may not be representative of all heterosexuals in urban environments or non-urban environments. Second, we did not use respondent-driven sampling weights in our analysis; as such, point estimates may have been biased by overrepresented or underrepresented subgroups of the sample. However, we adjusted for potential sampling biases by accounting for recruitment chains and adjusting for respondents’ network size in the Poisson models with generalized estimating equations. Third, data were collected in 2013, and the nature of the study population and the association between the predictors and outcomes may have changed since then. However, we believe the strengths of the study, including the paucity of empirical studies on incarceration and HIV risk among heterosexual men, outweigh this limitation.
Fourth, because an interviewer administered the survey, certain behaviors might have been underreported or overreported. For example, respondents may have underreported socially undesirable behaviors (eg, injection drug use). We did not have data on respondents’ reasons for detainment, so we could not infer whether incarceration was because of reported illegal behaviors, such as injection drug use. In addition, we did not have data on when respondents were incarcerated in relation to their interview date, the length of their incarceration (except that it was at least 24 hours), or whether the respondent was in a local jail or a state or federal prison. These data could provide more information on the association between incarceration and HIV risk. For example, duration of incarceration may be more important than time since incarceration because persons who spend less time incarcerated have more high-risk sexual partners than persons who spend more time incarcerated. 15
Finally, because our data were cross-sectional, we could not infer causality or the temporal nature of the predictor and outcomes. Although our study corroborates previous findings on incarceration and HIV risk, we were not able to determine the temporal relationship between the two. Some longitudinal studies suggest that involvement with the criminal justice system may lead to increased risk-related sexual and drug-use behavior, 18,38 whereas other studies suggest that incarcerated persons have a higher prevalence of such behaviors than the general population before entering the criminal justice system. 47 Whether HIV risk is greater before or after incarceration is difficult to discern because recidivism is common. 44
Conclusions
Meeting the needs of recently incarcerated and ever-incarcerated men could directly reduce the incidence of HIV at the individual and community levels. Our findings highlight the need for more initiatives that promote strategies to mitigate HIV risk–related behaviors, correctional rehabilitation, and healthy reentry into communities among heterosexual men at high risk for HIV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support for the research, authorship, and/or publication of this article.