
Abstract

Per- and polyfluoroalkyl substances (PFASs) are in the public spotlight because of mounting evidence for their ubiquity, prevalence in US drinking water, and negative health effects on persons. 1,2 PFASs have been in production since the 1940s 3 and are used in various products, including firefighting foam, nonstick cookware, food packaging, and stain- or water-resistant textiles. 3,4 As of June 2018, the Organisation for Economic Cooperation and Development had documented 4730 PFAS structures, including mixtures and several new groups of PFASs; however, it is unknown how many PFASs are in commerce. 5 Since 1999, the Centers for Disease Control and Prevention has measured at least 12 PFASs in serum samples from participants in the National Health and Nutrition Examination Survey, indicating widespread exposure across the country. 6 Although in this article we focus on drinking water guidelines for PFASs across the United States, it is important to recognize that the contribution of drinking water exposure to the total body burden of PFASs is uncertain, because compelling evidence indicates that exposures also occur through diet (including breastmilk for infants), dust, and inhalation of air. 7
In 2016, the US Environmental Protection Agency (EPA) established drinking water health advisories for the 2 most-studied PFASs: perfluorooctanoic acid (PFOA) and perfluorooctane sulfonate (PFOS). 8 The health advisories were developed under a federal provision of the Safe Drinking Water Act “to assist federal, state, tribal and local officials, and managers of drinking water systems in protecting public health when these chemicals are present in drinking water.” 8,9 The EPA recommends that no more than 70 ng/L or parts per trillion (ppt) of PFOA and PFOS combined be present in drinking water. This guidance is intended to protect the health of a person consuming the water every day during the course of a lifetime, but it is not legally enforceable. The health advisories were developed in response to data from the Unregulated Contaminant Monitoring Rule (UCMR3), which demonstrated that of 4920 public water supply systems evaluated for the presence of 6 PFAS chemicals, 117 systems tested positive for at least 1 of the 6 PFAS chemicals. 9 -11 An analysis of the UCMR3 data from 4064 water supply systems each serving at least 10 000 persons found that 66 of these water systems reported PFAS concentrations at or above the EPA’s health advisory. 10 The UCMR3 analyses were conducted using a reporting range of 10-90 ppt. However, detection of lower levels of PFASs is possible, and when the reporting limits are lowered to 2.5 ppt, reanalysis of the data by the Environmental Working Group suggests that up to 110 million Americans could be exposed to PFASs in drinking water. 12 The federal Safe Drinking Water Act applies only to public water supplies. 11 Thus, monitoring and controlling exposures of PFASs at private wells presents a challenge to state and local regulators. To date, attention is focused on PFAS source areas, such as PFAS manufacturing and use facilities, landfills, and fire-training facilities and operations. 13 As the PFAS problem evolves, lower-level contamination may prove more challenging because source areas may not be apparent, migration of PFASs may be more extensive than previously thought, and analytical detection methods are becoming more sensitive.
Health Effects of PFASs
Epidemiological and toxicological evidence for the health effects of PFASs is growing rapidly. Several communities in the mid-Ohio Valley have been exposed to releases of PFOA (known as C8) emitted from the Washington Works plant in Parkersburg, West Virginia, since the 1950s. As a part of the 2005 settlement for a class-action lawsuit filed against the plant, the C8 Science Panel was formed to study the associations between exposure to PFOA and health outcomes. 14 From 2005 through 2013, the panel conducted these exposure and health studies that established strong links between PFOA and diseases such as kidney cancer, testicular cancer, ulcerative colitis, thyroid disease, hypercholesterolemia, and pregnancy-induced hypertension. 15 Further research found relationships between levels of PFASs in serum and numerous additional health outcomes. These relationships include increased cholesterol levels, 16 high blood pressure, 17 decreased response to vaccines, 18 thyroid disease, 19 decreased fertility among women, 20 increased risk of high blood pressure or pre-eclampsia among pregnant women, 21 and lower infant birth weight. 22 The Agency for Toxic Substances and Disease Registry (ATSDR) toxicological profile for perfluoroalkyls reviewed studies demonstrating these adverse effects. 2
State PFAS Guidelines and Protections
As of August 2018, 14 states had adopted the EPA health advisory, 4 states had established their own health advisories or regulatory levels, and 31 states had remained silent on their approaches to PFOA and PFOS. In addition, New Hampshire and New York State were in the process of deriving drinking water standards. 23,24 Minnesota, New Jersey, and Vermont set allowable ppt concentrations that are lower than the EPA’s allowable concentration of 70 ppt for PFOA and PFOS, translating to more protective health advisories. The allowable concentration of 70 ppt in Arizona, Colorado, Connecticut, and Massachusetts uses the sum of multiple PFASs, including PFOA and PFOS, recognizing the potential additivity of effects (Table 1).
Per- and polyfluoroalkyl substances detected in public drinking water supplies with state and federal drinking water guidelines, United States, 2018a
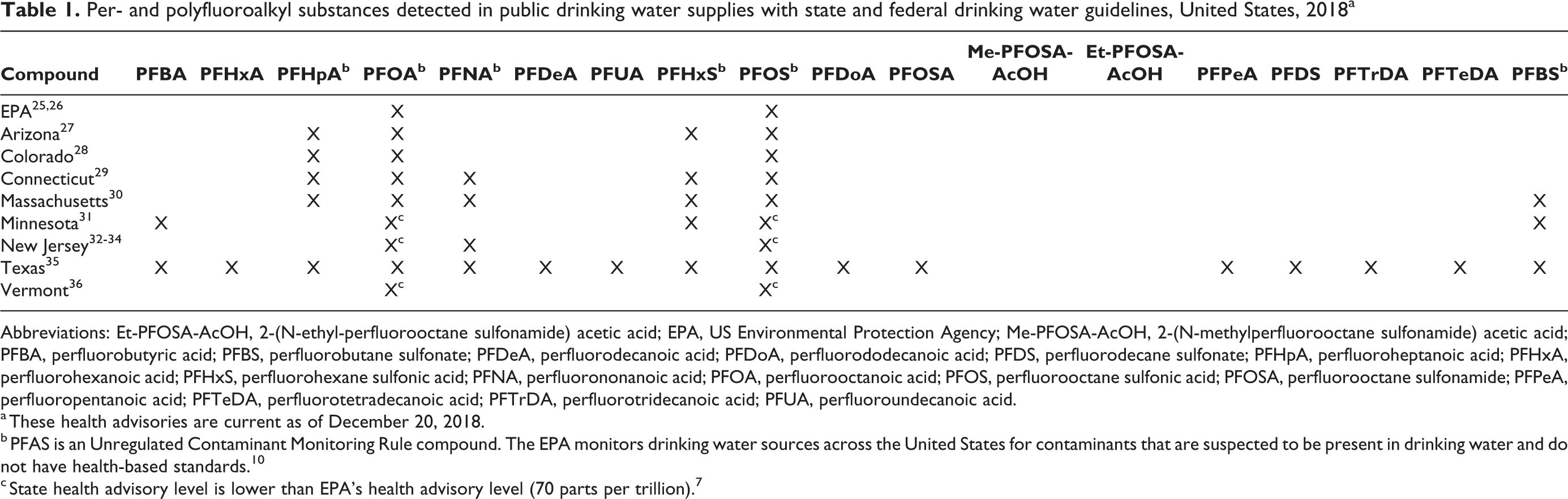
Abbreviations: Et-PFOSA-AcOH, 2-(N-ethyl-perfluorooctane sulfonamide) acetic acid; EPA, US Environmental Protection Agency; Me-PFOSA-AcOH, 2-(N-methylperfluorooctane sulfonamide) acetic acid; PFBA, perfluorobutyric acid; PFBS, perfluorobutane sulfonate; PFDeA, perfluorodecanoic acid; PFDoA, perfluorododecanoic acid; PFDS, perfluorodecane sulfonate; PFHpA, perfluoroheptanoic acid; PFHxA, perfluorohexanoic acid; PFHxS, perfluorohexane sulfonic acid; PFNA, perfluorononanoic acid; PFOA, perfluorooctanoic acid; PFOS, perfluorooctane sulfonic acid; PFOSA, perfluorooctane sulfonamide; PFPeA, perfluoropentanoic acid; PFTeDA, perfluorotetradecanoic acid; PFTrDA, perfluorotridecanoic acid; PFUA, perfluoroundecanoic acid.
a These health advisories are current as of December 20, 2018.
b PFAS is an Unregulated Contaminant Monitoring Rule compound. The EPA monitors drinking water sources across the United States for contaminants that are suspected to be present in drinking water and do not have health-based standards. 10
c State health advisory level is lower than EPA’s health advisory level (70 parts per trillion). 7
Health advisories are developed for the protection of public health; as such, it is important to base them on the most relevant, sensitive endpoint. The EPA health advisories for PFOA and PFOS are based on toxicological studies in animals. No state or federal guidelines have been derived from epidemiological evidence. The critical effects used to derive these guidelines are described in Table 2. Many states have considered only PFOA and PFOS. Colorado, Connecticut, and Massachusetts have included other PFASs that, when their concentrations are added to those of PFOA and PFOS in drinking water, cannot exceed 70 ppt. Minnesota recognized that the assumptions made about the proportion of Americans’ daily PFAS exposure that comes from drinking water in the derivation of the national health advisory may underestimate exposure from other sources. In July 2018, Vermont revised its health advisory to protect a developing fetus, stipulating that the sum of 5 PFASs are not to exceed 20 ppt. New Jersey is the first state to promulgate a drinking water standard for perfluorononanoic acid, 1 of the 14 PFASs measured in drinking water supplies. 34 Pregnant women and bottle-fed infants are the most susceptible, because data demonstrate that PFASs cross the placenta, are present in breastmilk, and can adversely affect young children. 2 Drinking water estimates used to derive health advisories protect bottle-fed infants, because the intake-to-body weight ratio is greatest for this population.
Toxicological basis for federal and state drinking water health advisory levels for perfluorooctanoic acid (PFOA) and perfluorooctane sulfonic acid (PFOS), United States
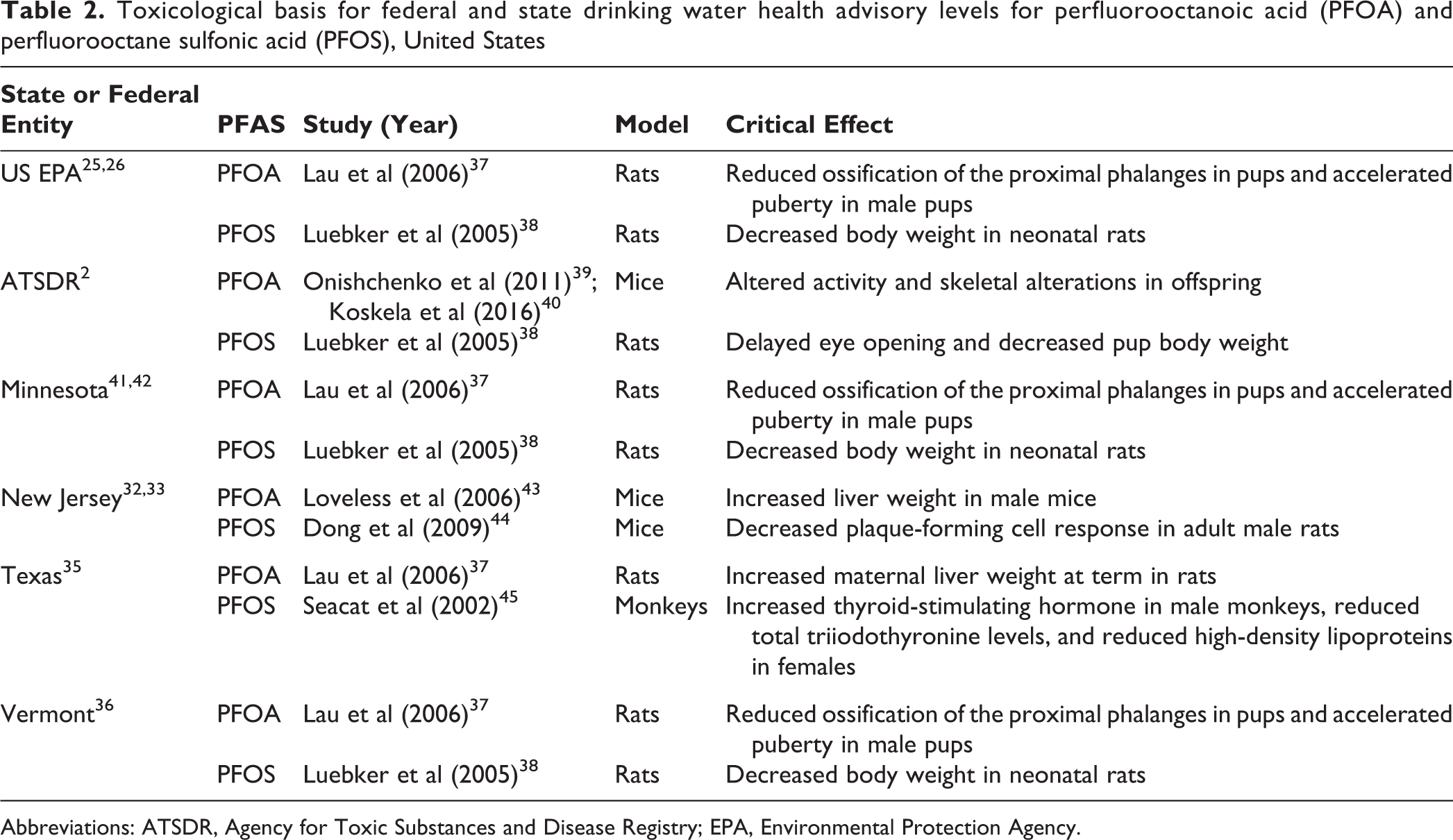
Abbreviations: ATSDR, Agency for Toxic Substances and Disease Registry; EPA, Environmental Protection Agency.
The focus on PFOA and PFOS neglects the presence and toxicity of the other 13 PFASs that have been detected in drinking water. Concerns about the lack of protections afforded by the EPA’s health advisory are echoed in ATSDR’s newly issued minimal risk levels, which are nearly an order of magnitude lower. 2 The minimal risk levels are similarly derived but are based on the ability of PFOA and PFOS to cause immune suppression and negatively affect mammary gland development in animal studies. Taking these data into account, if the EPA lowered its health advisory by at least 1 order of magnitude, an estimated 100 million more persons in the United States are drinking water with levels of PFASs that pose unacceptable health risks. 2,12
Risk Reduction and Communication Efforts
In 2016, researchers demonstrated that the presence of firefighting facilities that used or stored PFAS-containing aqueous film-forming foams co-located with elevated concentrations of PFASs in drinking water. 13 Some states initiated risk-reduction measures. For example, Washington State is moving to replace aqueous film-forming foams with non–fluorine-containing foams, 46 and Massachusetts is taking back foams manufactured before 2003. 47 In Washington State, restrictions will not apply to the military, the Federal Aviation Administration, petroleum refineries and terminals, or large chemical factories. 46
As members of communities with contaminated water seek health information, clinicians are tasked with communicating uncertainty and should become familiar with conditions for which the evidence strongly suggests an association with PFAS exposure. ATSDR provides a list in its interim communication guide for clinicians. 48 It is important to explain ways to decrease exposure—using alternative water sources for teeth brushing, drinking, preparing food, and cooking—to persons in affected communities. Clinicians should be aware that not all analytical laboratories can reliably test for PFASs in human serum and water, and should convey to patients that these tests do not necessarily predict health outcomes. 48
Public Demand for PFAS Regulation
In July 2018, the EPA began holding community engagement sessions across the country in recognition of the nationwide concern about PFASs. After the release of the EPA health advisory, PFASs received a surge of attention from communities, advocacy groups, and elected officials on a scale and time frame that was unmatched in recent US environmental history. Public interest has been so strong that 3 PFASs were removed from the US Food and Drug Administration’s Food Contact Notification list for safety concerns. 49 This type of action is almost unprecedented: previously, the Food and Drug Administration had only removed trans fats and bisphenol A (BPA) from this list of safe substances. Although trans fats were removed for health reasons, BPA was deemed unfit for the list because of “market abandonment.” 50
Social media may be further engaging the public with environmental issues and persons who are affected by them. Research indicates that using social media during environmental disasters can enhance one’s ability to share knowledge about the situation and help others who are affected. 51 In addition, the framing of environmental issues and subsequent public perception of them is influenced by the media, and PFAS contamination events and ensuing lawsuits have generated considerable media attention in recent years. 50
The EPA responded to the issues voiced by affected communities, states, and water utilities with the following priorities: (1) initiate the development of a drinking water standard for PFOA and PFOS; (2) designate PFOA and PFOS as “hazardous substances”; (3) develop toxicity values for 2 additional PFASs, perfluorobutane sulfonate and 2,3,3,3-tetrafluoro-2-(1,1,2,2,3,3,3- heptafluoropropoxy)propanoic acid or hexafluoropropylene oxide dimer acid—and 2,3,3,3-tetrafluoro-2- (1,1,2,2,3,3,3-heptafluoropropoxy)propanoate—or hexafluoropropylene oxide dimer acid ammonium salt (known as “GenX” compounds); and (4) develop recommendations for groundwater cleanup levels. The EPA is listening to persons who are directly affected at the continuing community engagement sessions, although states are taking the lead on setting guidelines and standards.
Regulation of PFASs
Regulation of the manufacture and use of PFASs in the United States focuses on reporting, alternatives to long-chain PFASs, and voluntary bans. It also covers the continued production of a subset of PFASs, characterized by the EPA as very low volume, low exposure, and low release, for which no alternatives are available. PFOA has been phased out of production in the United States but may be present in some imported items. PFOS is no longer manufactured or imported into the United States, although some limited uses for PFOS remain. 52 The Helsingør Statement was published in response to the replacement of long-chain compounds with alternative PFASs. The authors argued that because of insufficient toxicological testing, the chemical behavior, and potentially persistent terminal transformation products of PFASs, continued use and development of nonpersistent alternatives should be strongly encouraged to protect humans and the environment. 53
Conclusions
As the EPA continues its community engagement sessions, the magnitude of PFAS contamination in US water supplies is unprecedented. Millions of persons are affected, and the challenges ahead are great. Studies have found previously undocumented sources of PFASs, additional PFASs in water supplies, and more health effects associated with exposure to PFASs at decreasing doses, including below the EPA guidelines of 70 ppt. Communities and organizers are demanding that drinking water with measurable PFASs be treated to remove these chemicals and that establishing toxicity and drinking water guidelines for PFOA and PFOS alone is insufficient. Protecting public health means preventing exposure to all PFASs that are present in water supplies and other environmental media above risk thresholds. Because the risk thresholds continue to decrease, prevention may be accomplished only by controlling and decreasing exposures to PFASs already in the environment. Measures also need to be taken to restrict or ban the manufacture of these toxic chemicals. Alternatives to the fluorinated products are strongly encouraged. We believe the new Lautenberg Amendment to the Toxic Substances Control Act should be leveraged to require PFAS replacements to be subject to robust premarket testing. 54
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: W.H.-B. is partially funded by National Institutes of Health P42 ES007381.