
Abstract
Objective:
Although research suggests racial/ethnic disparities in influenza vaccination and mortality rates, few studies have examined racial/ethnic trends among US adolescents. We used national cross-sectional data to determine (1) trends in influenza vaccination rates among non-Hispanic white (hereinafter, white), non-Hispanic black (hereinafter, black), and Hispanic adolescents over time and (2) whether influenza vaccination rates among adolescents varied by race/ethnicity.
Methods:
We analyzed provider-reported vaccination histories for 2010-2016 from the National Immunization Survey–Teen. We used binary logistic regression models to determine trends in influenza vaccination rates by race/ethnicity for 117 273 adolescents, adjusted for sex, age, health insurance, physician visit in the previous 12 months, vaccination facility type, poverty status, maternal education level, children in the household, maternal marital status, maternal age, and census region of residence. We calculated adjusted probabilities for influenza vaccination for each racial/ethnic group, adjusted for the same demographic characteristics.
Results:
Compared with white adolescents, Hispanic adolescents had higher odds (adjusted odds ratio [aOR] = 1.11; 95% confidence interval [CI], 1.06-1.16) and black adolescents had lower odds (aOR = 0.95; 95% CI, 0.90-1.00) of vaccination. Compared with white adolescents, Hispanic adolescents had significantly higher adjusted probabilities of vaccination for 2011-2013 (2011: 0.22, P < .001; 2012: 0.23, P < .001; 2013: 0.26, P < .001). Compared with white adolescents, black adolescents had significantly lower probabilities of vaccination for 2016 (2016: 0.21, P < .001).
Conclusions:
Targeted interventions are needed to improve adolescent influenza vaccination rates and reduce racial/ethnic disparities in adolescent vaccination coverage.
Influenza is a major cause of morbidity and mortality in the United States. 1 -6 From the 2010-2011 through 2015-2016 influenza seasons, influenza-associated hospitalizations ranged from 139 000 to 708 000, and influenza-associated deaths ranged from 16 000 to 76 000. 7 The youngest and oldest members of the US population are the most likely to die from influenza-related complications. 5,6,8 -11
The risks of influenza-related morbidity and mortality can be mitigated through the use of annual vaccinations, which can result in fewer influenza-related hospitalizations and deaths. 2,12 -15 Influenza vaccinations are particularly important for children and adolescents, not only for self-protection but also for preventing the transmission of the virus to others in their households and communities. 16 -21 Recent research suggests that routinely vaccinating children and adolescents against influenza would substantially reduce influenza-related morbidity and mortality at the population level. 22 -25 For example, achieving an 80% influenza uptake rate among children and adolescents would likely result in a 91% reduction in the total number of influenza illness cases on a population-wide basis. 25
Despite the proven effectiveness of influenza vaccination, disparities in vaccination coverage exist for certain age groups. From the 2007-2008 influenza season through the 2011-2012 influenza season, vaccination rates increased for children as a single group, but most of that growth was among children aged 6 months to 4 years. 26 Influenza vaccination rates tend to decrease as children age through childhood and into adolescence. 27 The result is that adolescents aged 13-17 routinely have the lowest vaccination rates among all children aged <18.
Disparities in vaccination rates also exist for certain racial/ethnic groups. National estimates showed that during the 2015-2016 influenza season, non-Hispanic white (hereinafter, white) adults were immunized at higher rates (45%) than either non-Hispanic black (hereinafter, black; 37%) or Hispanic (34%) adults. 27 The negative effect of these disparities is magnified by the higher risk of influenza-related death among black and Hispanic adults compared with white adults. 28 -33 Racial/ethnic vaccination disparities among children and adolescents may exacerbate influenza-related death, because unvaccinated children and adolescents who develop influenza may interact with older racial/ethnic minority adults who also are unlikely to have been vaccinated against influenza. Such disparities and vulnerabilities highlight the importance of influenza vaccination for children and adolescents.
Despite research suggesting racial/ethnic variations in influenza vaccination and mortality rates, few studies have examined racial/ethnic trends in influenza vaccination rates among US adolescents. 34,35 In addition, few reports on racial/ethnic variations in influenza vaccination and mortality rates have been published since the passage of the Patient Protection and Affordable Care Act in 2010. The Affordable Care Act increased access to health care and preventive health services, including immunizations, among adolescents and young adults, largely benefiting racial/ethnic minority groups and socioeconomically disadvantaged groups. 36 -39 At present, it is unclear whether the Affordable Care Act has led to reduced disparities in influenza vaccination coverage and improved influenza vaccination rates among adolescents. Understanding influenza vaccination trends among adolescents could guide public health interventions to prevent adolescent infection and reduce the effect of influenza on communities.
We used national cross-sectional data to determine (1) trends in influenza vaccination rates among white, black, and Hispanic adolescents over time and (2) whether influenza vaccination rates among adolescents varied by race/ethnicity.
Methods
We analyzed provider-reported vaccination histories for adolescents aged 13-17 from the 2010-2016 National Immunization Survey–Teen (NIS-Teen). The NIS-Teen is a national, random-digit-dial survey of parents and adolescents that is conducted annually and uses a dual-frame sampling design (landline and cellular telephone). The National Center for Health Statistics collected data for 2010 through 2014, and the National Center for Immunization and Respiratory Diseases collected data for 2015 through 2016. 40 The NIS-Teen relies on both parental and provider reports to estimate vaccination coverage for adolescents. After parental consent is obtained, vaccination histories are gathered for each adolescent from all known vaccination providers since birth. Providers are then asked to complete immunization history questionnaires for the adolescents. Parental reports of influenza vaccination tend to overestimate vaccination rates, and provider reports of influenza vaccination tend to slightly underestimate vaccination rates. 41 Thus, to avoid overestimating the vaccination rates, we chose to use only provider-reported vaccination histories for this study.
We pooled data from 2010-2016 and stacked them into a single data set for the entire study period. The initial sample included 266 093 adolescents. We then excluded any adolescents who had missing or unknown data for provider facility type (n = 125 400) or for total family income (n = 16 177). We also excluded adolescents who did not have adequate provider-reported vaccination histories (n = 119 700) and who reported a racial/ethnic category other than Hispanic, white only, and black only (n = 26 148). Finally, we also excluded adolescents who had missing data for health insurance (n = 356), recent physician visit (n = 693), and census region of residence (n = 1482). We excluded some adolescents based on more than 1 exclusion criteria. As such, using listwise deletion, we excluded a total of 148 820 (55.9%) adolescents, resulting in a final sample size of 117 273 adolescents.
Response rates for the landline surveys averaged 56% (of which about 58% had adequate provider-reported data) and for the cellular telephone surveys averaged 27% (of which about 52% had adequate provider-reported data). The institutional review board at Florida State University approved this study.
Measures
Influenza vaccination
The dependent variable of interest was any provider-reported seasonal influenza vaccination between September 1 and January 31 of each survey year, measured as a binary variable (1 = received at least 1 influenza vaccination during this period; 0 = did not receive influenza vaccination during this period). For example, for the 2010 survey year, adolescents who were vaccinated between September 1, 2009, and January 31, 2010, were considered to have received influenza vaccination for the 2009-2010 influenza season. To examine trends in influenza vaccination, we created additional variables indicating the year of the survey.
Race/ethnicity
Our primary independent variable was adolescent race/ethnicity. This variable included white, black, and Hispanic adolescents. Although the NIS-Teen allows respondents to choose other racial/ethnic groups, few adolescents selected other racial/ethnic groups, making it difficult to assess within-group variation. Thus, we excluded from our analysis those who chose multiple races or ethnicities or who were classified as “other.”
Adolescent characteristics
In our analyses, we controlled for the following characteristics: age (in years), sex (1 = male, 0 = female), census region of residence (Midwest, Northeast, South, and West), poverty status (total family income below the federal poverty level, total family income at or above the federal poverty level but ≤$75 000, and total family income >$75 000), 42 health insurance (Medicaid, private insurance, other insurance, and uninsured), physician visit in the previous 12 months (1 = yes, 0 = no), and vaccination facility type (public [eg, clinic, community health center], hospital, private practice, and other).
We also controlled for the following maternal characteristics: age (<34, 35-44, and ≥45), education level (<high school, high school, some college, and ≥college), marital status (1 = married, 0 = unmarried), and number of children residing in maternal household (1, 2 or 3, ≥4).
Analysis
We calculated descriptive statistics for each measure and stratified the results by race/ethnicity. We displayed unadjusted influenza vaccination rates for each racial/ethnic group. We then performed binomial logistic regression analyses to determine whether influenza vaccination rates varied by race/ethnicity and whether the impact of year on vaccination rates varied by race/ethnicity. We reported results as adjusted odds ratios (aORs) and 95% confidence intervals (CIs).
We used model 1 primarily to determine significant trends in vaccination rates over time. We used a 2-tailed test of significance and considered P < .05 to be significant. An aOR >1 that was significant indicated higher odds of being recently vaccinated against influenza. We used model 2 primarily to determine whether trends in vaccination rates varied by race/ethnicity. In this model, significant aORs for the interaction terms “race × year” indicated that racial/ethnic differentials in vaccination rates in that year varied compared with vaccination rates in 2010. We used models 3 through 5 primarily to determine whether variables for each characteristic (eg, sex, year) differed significantly from the reference variable in vaccination coverage within each race/ethnicity (eg, black male adolescents compared with black female adolescents).
Finally, we determined temporal trends in influenza vaccination rates during the 7-year period for all adolescents and for the 3 racial/ethnic groups. We calculated probabilities for influenza vaccination for each racial/ethnic group and adjusted them for all adolescent and maternal characteristics. We then displayed the point estimates graphically for each racial/ethnic group, by year, with vertical lines depicting 95% CIs around each probability estimate.
We conducted all statistical analyses by using Stata version 13. 43 We used Stata’s margins command to calculate probabilities and to perform the difference tests.
Results
The study sample included 117 273 adolescents aged 13-17, with a mean age of 15 (Table 1). Of these, 85 444 (72.9%) were white, 19 415 (16.6%) were Hispanic, and 12 414 (10.6%) were black. Twenty-four percent of white adolescents (20 330 of 85 444), 22.6% of Hispanic adolescents (4393 of 19 415), and 20.5% of black adolescents (2546 of 12 414) received an influenza vaccination.
Characteristics of non-Hispanic white, non-Hispanic black, and Hispanic adolescents aged 13-17, US National Immunization Survey-Teen, 2010-2016a,b
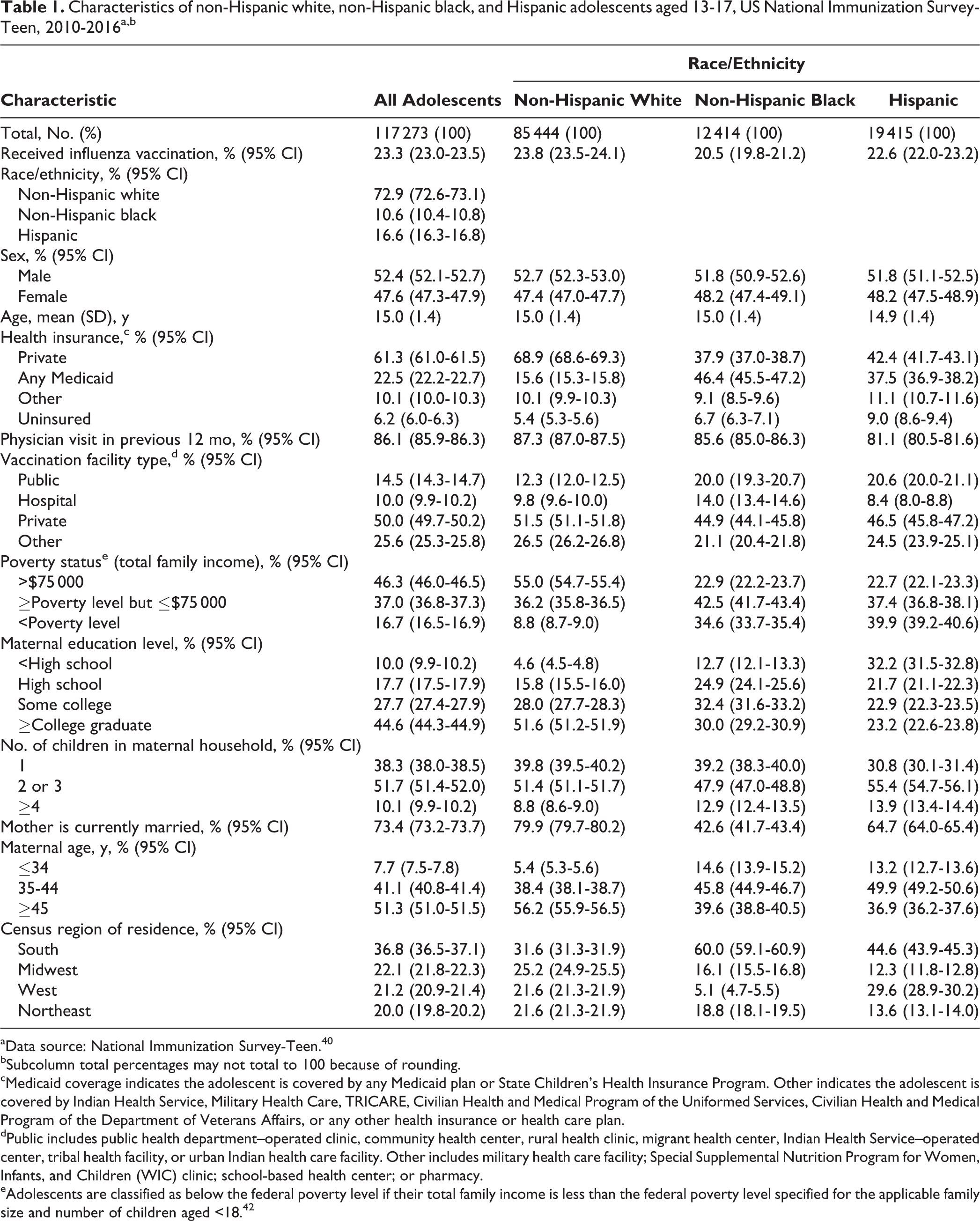
aData source: National Immunization Survey-Teen. 40
bSubcolumn total percentages may not total to 100 because of rounding.
cMedicaid coverage indicates the adolescent is covered by any Medicaid plan or State Children’s Health Insurance Program. Other indicates the adolescent is covered by Indian Health Service, Military Health Care, TRICARE, Civilian Health and Medical Program of the Uniformed Services, Civilian Health and Medical Program of the Department of Veterans Affairs, or any other health insurance or health care plan.
dPublic includes public health department–operated clinic, community health center, rural health clinic, migrant health center, Indian Health Service–operated center, tribal health facility, or urban Indian health care facility. Other includes military health care facility; Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) clinic; school-based health center; or pharmacy.
eAdolescents are classified as below the federal poverty level if their total family income is less than the federal poverty level specified for the applicable family size and number of children aged <18. 42
Influenza vaccination rates among all adolescents rose steadily during the initial study period, rising from 19% in 2010 to 27% in 2014, before declining slightly to 26% in 2015 and 2016 (Figure 1). In 2010, white adolescents (19%) had a significantly higher unadjusted vaccination rate than Hispanic adolescents (17%; OR = 0.87; 95% CI, 0.77-0.98; P = .03). In 2016, white adolescents (27%) had significantly higher unadjusted vaccination rates than Hispanic (23%; OR = 0.83; 95% CI, 0.75-0.91; P < .001) and black (21%; OR = 0.71; 95% CI, 0.63-0.81; P < .001) adolescents.
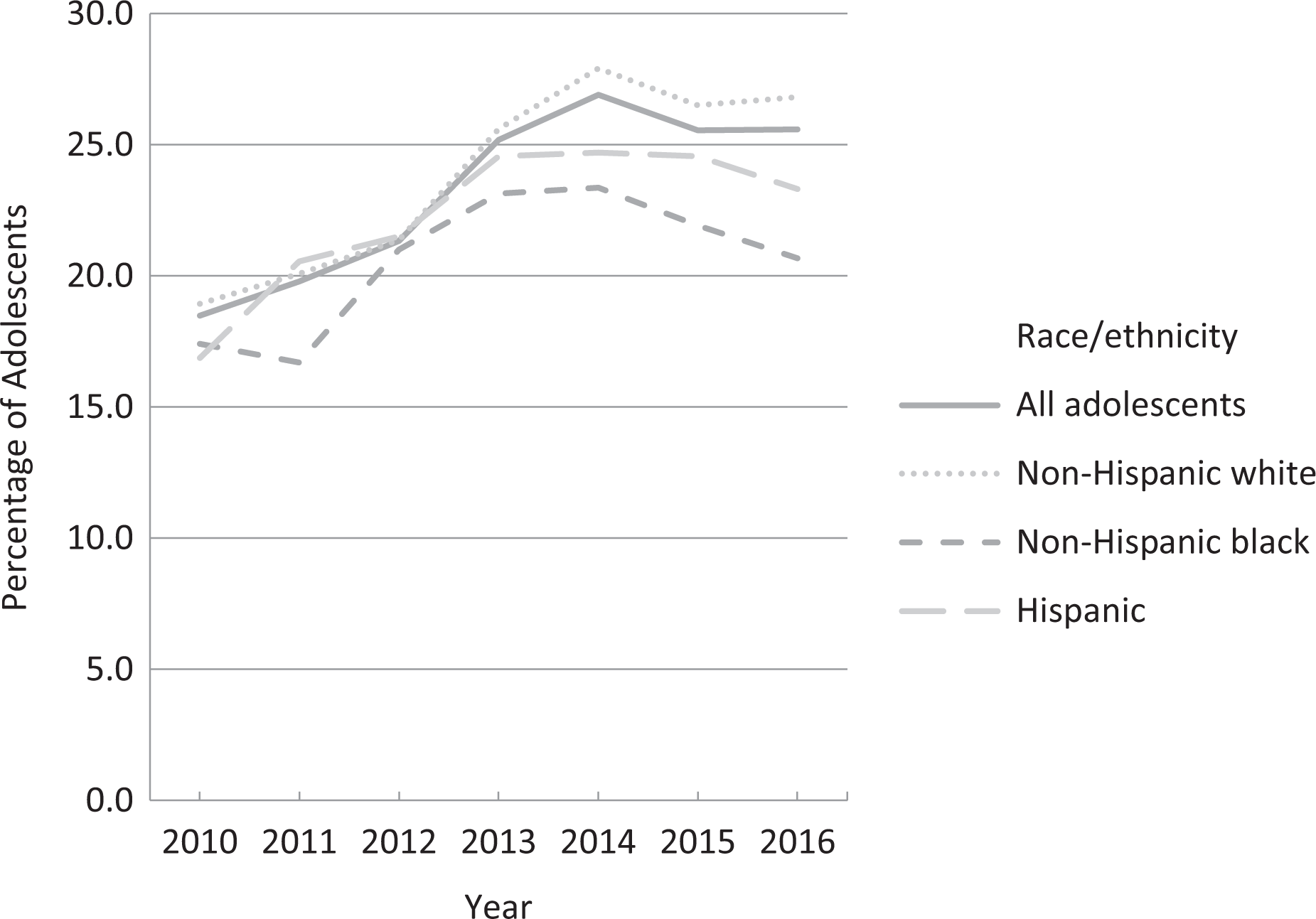
Influenza vaccination rates of non-Hispanic white, non-Hispanic black, and Hispanic adolescents aged 13-17, US National Immunization Survey-Teen, 2010-2016. 40 The study sample comprised 117 273 adolescents, of whom 85 444 were non-Hispanic white, 12 414 were non-Hispanic black, and 19 415 were Hispanic.
Model 1 suggests that, after adjusting for other factors, the odds of receiving an influenza vaccination among all adolescents increased by 9% (aOR = 1.09; 95% CI, 1.03-1.15) in 2011, 18% (aOR = 1.18; 95% CI, 1.12-1.25) in 2012, 43% (aOR = 1.43; 95% CI, 1.36-1.52) in 2013, 59% (aOR = 1.59; 95% CI, 1.50-1.67) in 2014, 48% (aOR = 1.48; 95% CI, 1.40-1.56) in 2015, and 44% (aOR = 1.44; 95% CI, 1.36-1.52) in 2016, as compared with the referent year of 2010 (Table 2). Compared with white adolescents, Hispanic adolescents had higher adjusted odds of vaccination (aOR = 1.11; 95% CI, 1.06-1.16) and black adolescents had lower adjusted odds of vaccination (aOR = 0.95; 95% CI, 0.90-1.00). In Model 2, the interaction term “Hispanic × 2011” (aOR = 1.19; 95% CI, 1.01-1.39) was positive and significant. The interaction term “black × 2016” (aOR = 0.77; 95% CI, 0.64-0.93) was negative and significant.
Logistic regression estimates (odds ratios) predicting influenza vaccination status of non-Hispanic white, non-Hispanic black, and Hispanic adolescents aged 13-17, based on US National Immunization Survey-Teen, 2010-2016a
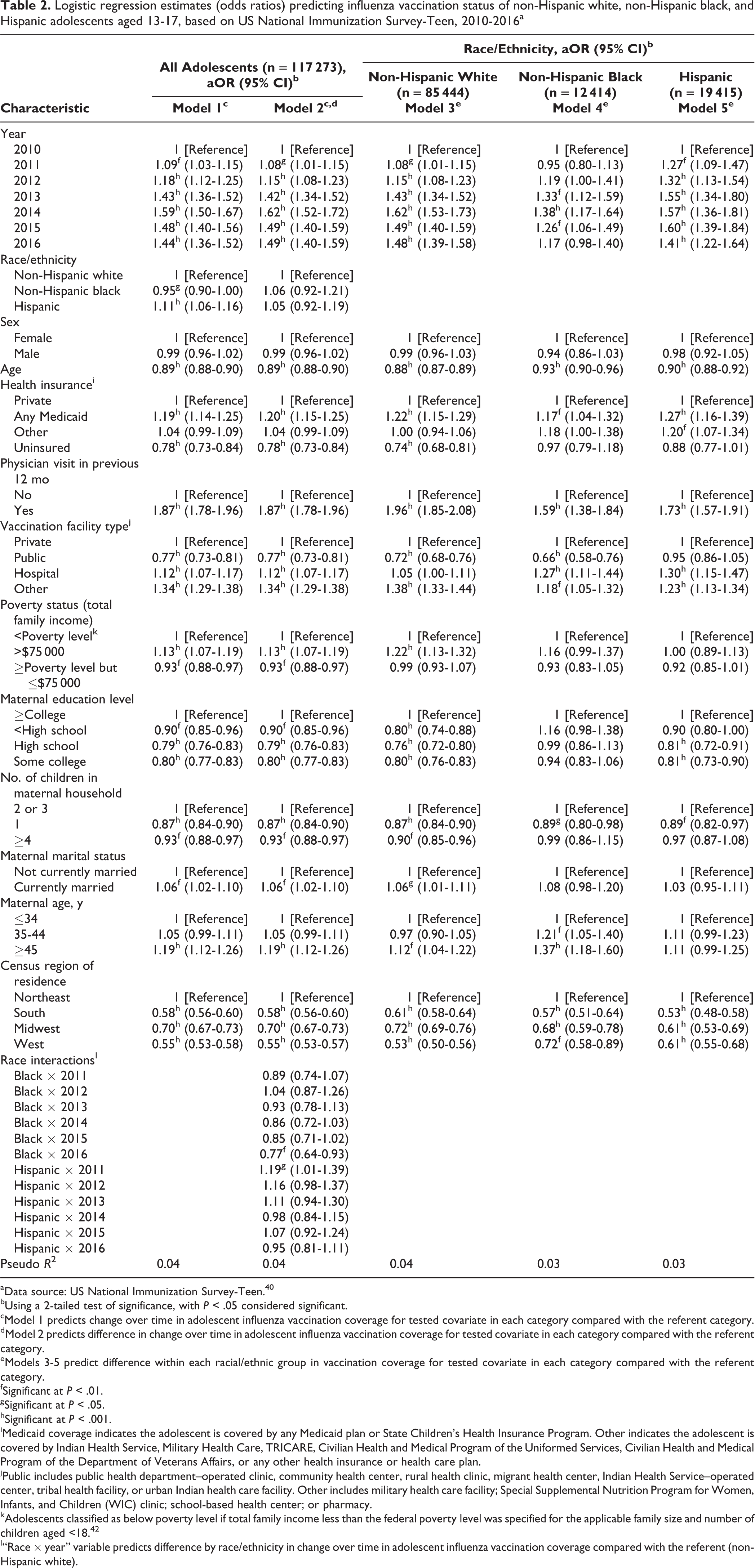
aData source: US National Immunization Survey-Teen. 40
bUsing a 2-tailed test of significance, with P < .05 considered significant.
cModel 1 predicts change over time in adolescent influenza vaccination coverage for tested covariate in each category compared with the referent category.
dModel 2 predicts difference in change over time in adolescent influenza vaccination coverage for tested covariate in each category compared with the referent category.
eModels 3-5 predict difference within each racial/ethnic group in vaccination coverage for tested covariate in each category compared with the referent category.
fSignificant at P < .01.
gSignificant at P < .05.
hSignificant at P < .001.
iMedicaid coverage indicates the adolescent is covered by any Medicaid plan or State Children’s Health Insurance Program. Other indicates the adolescent is covered by Indian Health Service, Military Health Care, TRICARE, Civilian Health and Medical Program of the Uniformed Services, Civilian Health and Medical Program of the Department of Veterans Affairs, or any other health insurance or health care plan.
jPublic includes public health department–operated clinic, community health center, rural health clinic, migrant health center, Indian Health Service–operated center, tribal health facility, or urban Indian health care facility. Other includes military health care facility; Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) clinic; school-based health center; or pharmacy.
kAdolescents classified as below poverty level if total family income less than the federal poverty level was specified for the applicable family size and number of children aged <18. 42
l“Race × year” variable predicts difference by race/ethnicity in change over time in adolescent influenza vaccination coverage compared with the referent (non-Hispanic white).
Models 3 through 5 suggest that, after adjusting for other factors, the odds of receiving an influenza vaccination increased among white adolescents by 8% (aOR = 1.08; 95% CI, 1.01-1.15) in 2011, 15% (aOR = 1.15; 95% CI, 1.08-1.23) in 2012, 43% (aOR = 1.43; 95% CI, 1.34-1.52) in 2013, 62% (aOR = 1.62; 95% CI, 1.53-1.73) in 2014, 49% (aOR = 1.49; 95% CI, 1.40-1.59) in 2015, and 48% (aOR = 1.48; 95% CI, 1.39-1.58) in 2016, as compared with the referent year of 2010; among black adolescents by 33% (aOR = 1.33; 95% CI, 1.12-1.59) in 2013, 38% (aOR = 1.38; 95% CI, 1.17-1.64) in 2014, and 26% (aOR = 1.26; 95% CI, 1.06-1.49) in 2015, as compared with the referent year of 2010; and among Hispanic adolescents by 27% (aOR = 1.27; 95% CI, 1.09-1.47) in 2011, 32% (aOR = 1.32; 95% CI, 1.13-1.54) in 2012, 55% (aOR = 1.55; 95% CI, 1.34-1.80) in 2013, 57% (aOR = 1.57; 95% CI, 1.36-1.81) in 2014, 60% (aOR = 1.60; 95% CI, 1.39-1.84) in 2015, and 41% (aOR = 1.41; 95% CI, 1.22-1.64) in 2016, as compared with the referent year of 2010 (Table 2).
Adjusted probabilities and tests for marginal effects for each year identified significant differences in influenza vaccination trends among the 3 racial/ethnic groups (Figure 2). Based on tests for marginal effects, Hispanic adolescents, as compared with white adolescents, had significantly higher adjusted probabilities of vaccination from 2011 through 2013 (2011: 0.22, P < .001; 2012: 0.23, P < .001; 2013: 0.26, P < .001), with similar adjusted probabilities of vaccination in 2010 and 2014-2016. Based on tests for marginal effects, black adolescents, as compared with white adolescents, had similar adjusted probabilities of vaccination from 2010 through 2015, but they had significantly lower probabilities of vaccination in 2016 (2016: 0.21, P < .001).
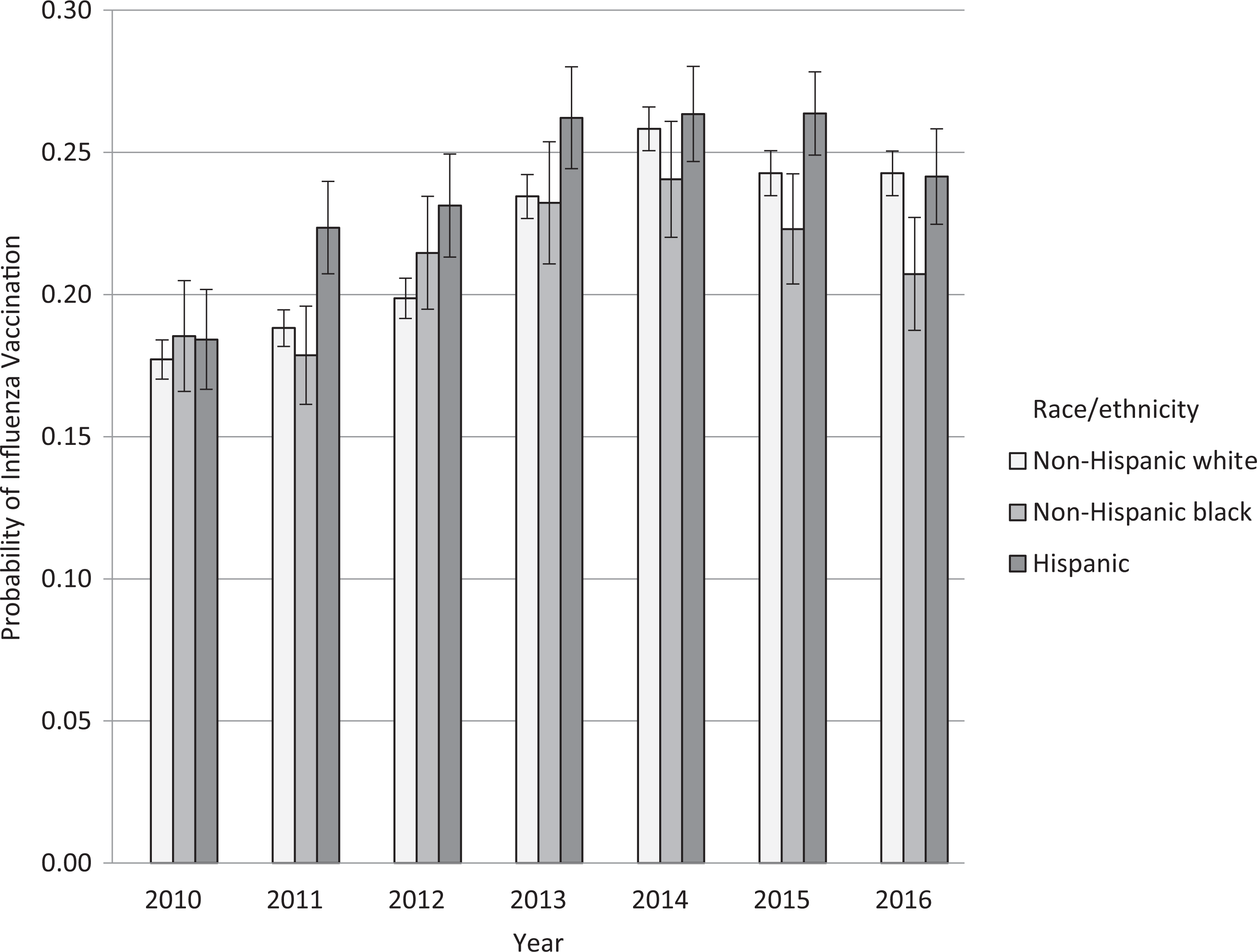
Adjusted probabilities for influenza vaccination status of non-Hispanic white, non-Hispanic black, and Hispanic adolescents aged 13-17, by year, based on US National Immunization Survey-Teen, 2010-2016. 40 Significant differences in adjusted probabilities of adolescent vaccination coverage (compared with non-Hispanic white race/ethnicity). Probabilities based on marginal effects tests of race/ethnicity by year, adjusted for sex, age, type of health insurance, physician visit in previous 12 months, vaccination facility type, poverty status, maternal education level, children in household, maternal marital status, maternal age, and US Census region of residence. A total of 117 273 adolescents comprised the study sample, of whom 85 444 were non-Hispanic white, 12 414 were non-Hispanic black, and 19 415 were Hispanic.
Discussion
We identified low influenza vaccination rates in adolescents of all 3 racial/ethnic groups, confirming reports that adolescents consistently have the lowest vaccination rates among children aged <18 in the United States. 27,34,44 Two important findings emerged from this research. First, although influenza vaccination rates increased steadily during the initial study period for each racial/ethnic group, coverage peaked in 2014 and then declined slightly through 2016. Second, influenza vaccination rates were unevenly distributed across the 3 racial/ethnic groups from 2010 through 2016, and these between-group differences persisted even after controlling for other demographic characteristics, including sex, health insurance status, socioeconomic status, maternal education level, and region of residence.
Vaccination Coverage Disparities
We found that, after controlling for key demographic characteristics, Hispanic adolescents had higher influenza vaccination rates than white adolescents for much of the study period. However, that advantage tapered roughly midway through the study period, and influenza vaccination rates among white and Hispanic adolescents became similar. It has previously been reported that white adults have higher influenza vaccination rates than both Hispanic and black adults. 27 Additional research is warranted to better understand how these racial/ethnic trends in influenza vaccination rates vary by age.
We also found that whereas influenza vaccination rates during the initial 6 years of the study period varied only slightly between white and black adolescents, a disparity in these rates began emerging in 2014. By 2016, black adolescents received influenza vaccinations at significantly lower rates than their white counterparts. This finding is important because black adolescents and young adults consistently have worse health profiles than white and Hispanic adolescents and young adults. 45,46 Thus, vaccination disparities could further undermine the health of black people and contribute to the intergenerational transmission of adversity through illness. 47 -51 This finding is also important because disparities in vaccination rates could lead to increased transmission of influenza to other household and community members, resulting in further disparities in health and mortality in the black population. 16 -21 Compared with white adults, black and Hispanic adults have higher rates of cardiovascular disease, cerebrovascular disease, and diabetes—conditions that make contracting influenza particularly harmful. 28 -33 Additional research is needed not only to increase influenza vaccination rates among all adolescents but also to reduce these racial/ethnic disparities in vaccination coverage.
Comparability With Other Studies
The vaccination rates presented in this study were lower than rates in other studies for the same years and population. 27,34,44 Recent estimates suggest average adolescent vaccination rates of 29.4, 34.4, 34.5, 38.4, 42.0, 42.3, and 44.2 from the 2009-2010 influenza season to the 2015-2016 influenza season. 44 However, these estimates were based on parental reports and may be subject to recall bias. Parental reports, relative to provider reports, tend to overestimate influenza vaccination rates. 41 To our knowledge, no other studies have reported influenza vaccination rates stratified by race/ethnicity among adolescents for the same years.
Practical Implications
Our findings of low adolescent influenza vaccination rates and racial/ethnic disparities in these rates could have substantial implications for public health departments and public health workers looking to reduce influenza transmission rates. Older children and adolescents who contract influenza may transmit the virus to at-risk friends and family members, including young siblings, parents, and grandparents. Vaccinating more adolescents could strengthen herd immunity, which could ultimately protect vulnerable populations and reduce the direct and indirect costs associated with influenza. 52 Although the Advisory Committee on Immunization Practices recommends that all people aged 6 months or older receive an annual influenza vaccination, its recommendations place greatest emphasis on vaccinating those in age groups deemed to be at higher risk for influenza-related medical complications, particularly children aged 6-59 months and adults aged ≥50. 53 Also, physicians often preferentially recommend annual influenza vaccinations to the elderly, to limit the number of transmissions and to reduce the risk of health complications associated with influenza. 2,3,9,54 Shifting the emphasis from immunizing the youngest and oldest age groups to immunizing school-aged children and adolescents could have beneficial effects on influenza transmission rates for the entire population. 54
Limitations
This study had several limitations. First, the data we used limited our ability to understand the source of racial/ethnic variations in vaccination status. We were unable to determine the reasons for vaccination disparities across time or to provide actionable insights that could lead to potential interventions. Second, we relied on provider-reported medical data, which may have underestimated vaccination coverage rates among adolescents. 41 Previous reports of adolescent vaccination coverage for the 2009-2010 through 2015-2016 influenza seasons relied on parental reports. 27,34,44 Third, we used an abbreviated vaccination period (September through January), which could have resulted in underestimating vaccination rates or drawing different conclusions than if we had used a longer vaccination period. Adolescents whose data were collected before February 1 but who had their vaccinations after data collection would have had censored vaccinations, which could have resulted in underestimating vaccination rates. Also, if temporal vaccination trends or racial/ethnic vaccination disparities were substantially different from February through May than for September through January, then trend and disparity results for a study covering September through May could have differed from those that we observed. Fourth, record scattering (ie, data from multiple providers results in the lack of a consolidated immunization record) and underascertainment (ie, nonresponse from health care providers results in missing data) may have occurred. 55,56 If so, vaccination rates may have been underestimated. Fifth, we were unable to determine the nativity status of those responding to the NIS-Teen or to analyze the diversity within the multiple ethnic groups that comprised the Hispanic racial/ethnic group. Both of these limitations inhibited our ability to evaluate and control for potentially important within-group differences. Finally, because variables tapping parental hesitation about vaccination were not available in the NIS-Teen data, we were unable to assess the role that parental hesitation about vaccination might play in influenza vaccination noncompliance.
Directions for Future Research
Future research should examine within-group variations among Hispanic adolescents. Hispanic ethnicity is a grossly aggregated racial/ethnic distinction; as such, its use as a single group may hide important within-group variations in vaccination status and may make it difficult to assess the individual effects of ethnicity, nativity, and culture on influenza vaccination. 57 Future research should also explicitly focus on parental hesitations or concerns about vaccinations that lead to influenza vaccination noncompliance. Parents are hesitant to vaccinate their children and adolescents because of a lack of information, concerns about side effects, lack of access to health care due to cost, inadequate transportation, or inconvenient clinic hours. 58
Conclusion
Targeted interventions are needed, with the goal of improving adolescent influenza vaccination rates and reducing racial/ethnic disparities in adolescent vaccination coverage.
Footnotes
Acknowledgments
The authors are grateful for feedback on earlier drafts of this article from Dawn Carr, Stella Min, and Stephanie Ureña.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.