
Abstract

The federal Care and Prevention in the United States (CAPUS) Demonstration Project (hereinafter, CAPUS), which is featured in this supplemental issue of Public Health Reports, highlighted how addressing social determinants of health (SDHs) could reduce morbidity and mortality from HIV infection and AIDS. 1 In this commentary, we explore the rationale behind CAPUS and discuss how sustained efforts such as CAPUS could help reduce and ultimately eliminate racial/ethnic disparities in HIV/AIDS. We review growing scientific evidence documenting that interventions that address social and living conditions can be effective in reducing risks of HIV infection. We conclude that, to enhance our success in reducing morbidity and mortality from HIV/AIDS, we must understand the SDHs of HIV/AIDS, invest in efforts to dismantle the social conditions that lead to HIV/AIDS–related disparities, and strengthen the scientific evaluation of these efforts.
Disparities in HIV/AIDS
Although rates of HIV infection and AIDS and mortality of people with HIV infection declined from 2010 to 2014 in the United States, racial/ethnic disparities persist. HIV/AIDS is heavily concentrated among African American and Latino populations; African American people have higher rates of HIV/AIDS than do people of other racial/ethnic groups. 2 Data from the Centers for Disease Control and Prevention revealed that, although African American people represented 12% of the US population in 2015, they accounted for 42% of all people living with HIV in 2014, 44% of all deaths from HIV/AIDS in 2014, and 43% of new HIV diagnoses in 2015. Likewise, Latino people represented 18% of the US population in 2015 but accounted for 24% of new HIV diagnoses in 2015. In 2015, 22% of all people newly diagnosed with HIV infection were aged 13-24, and African American and Latino gay and bisexual males were overrepresented in this age group. African American men who have sex with men (MSM) have the highest incidence of HIV in the United States; they accounted for 26% (10 223 of 39 782) of new HIV diagnoses in 2016. 3 Racial/ethnic minority women account for a disproportionate share of diagnoses of HIV infection among women. In 2015, 61% of women newly diagnosed with HIV were African American, 19% were white, and 15% were Latino. 4 Racial/ethnic health disparities exist at every step in the HIV care continuum, from HIV testing to mortality. Compared with white people, African American and Latino people are less likely to be aware of their HIV status, to begin treatment, to be retained in care, and to have their viral load suppressed. 5
Social Determinants of Health
In this commentary, we use the terms health disparities and health inequities interchangeably. Although US researchers and policy makers have historically used the term disparities, the term inequities has increasingly been used to emphasize a focus on health differences that are avoidable and unjust. 6 Contextual factors for disease, known generally in many disciplines as SDHs, have been conceptualized as the drivers of health for decades by many public health experts. Indeed, SDHs embody the history of public health, which has focused on improving social conditions for all. 7 The SDH framework encompasses social, economic, and political systems and structural mechanisms that shape individual health-related risk behaviors (Figure). 8 For example, SDHs may include access to adequate housing, access to health care and/or health insurance, access to child care and education, employment status, gender equality, and income. 9 These upstream determinants help explain why race/ethnicity is associated with differential risks for disease and health outcomes. 10 They also create social stratification by income, education, class, gender, and race/ethnicity, including those associated with HIV/AIDS. 9
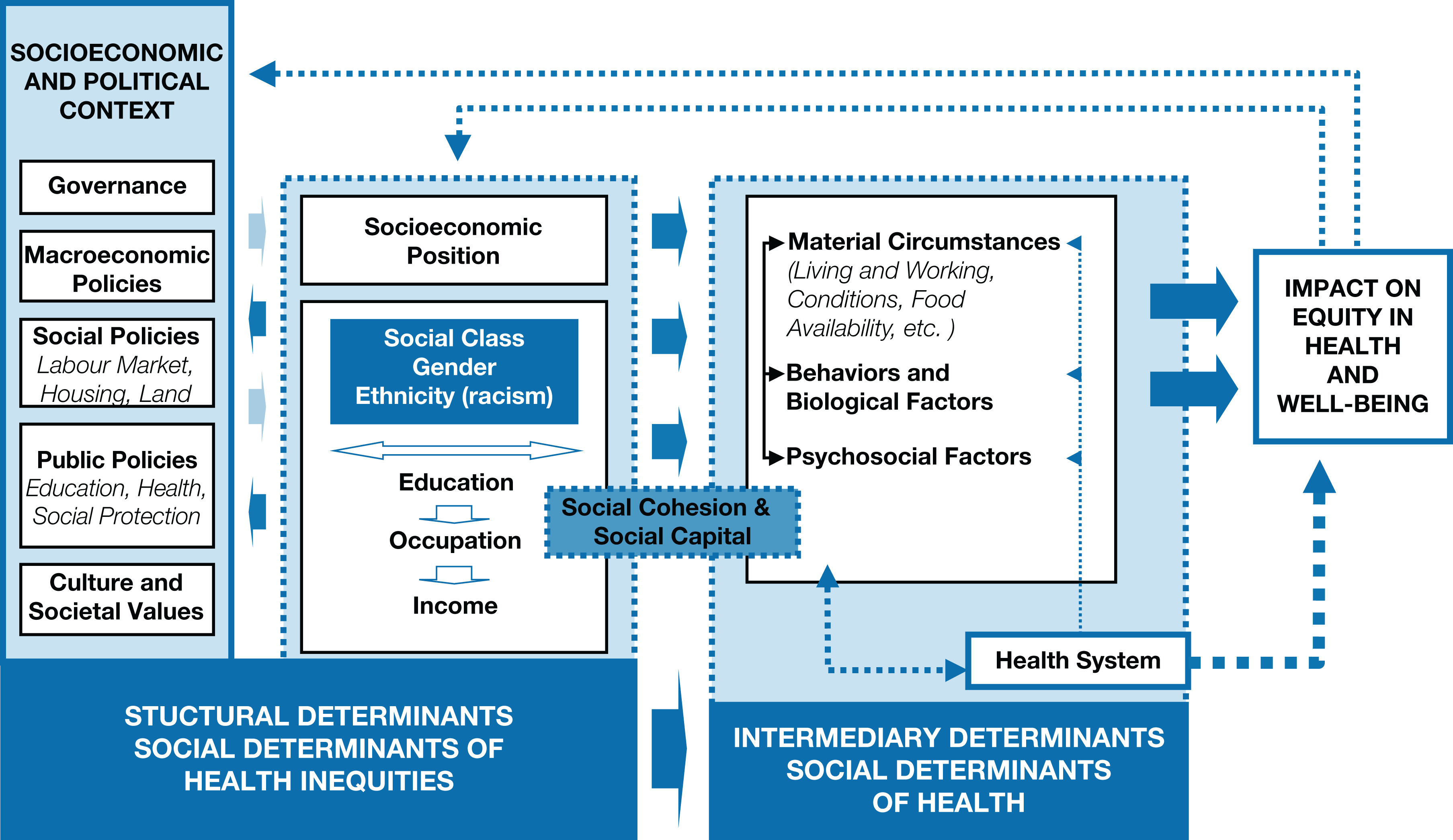
A conceptual framework for action on the social determinants of health, 2010. Data source: World Health Organization. 6 Used with permission. In this framework, structural determinants of health, including socioeconomic and political context and the person’s socioeconomic position, are considered upstream factors that influence the equity in health and well-being. Intermediary determinants of health, such as material circumstances, behaviors, and psychosocial factors, are considered downstream factors.
Although behavior, especially high-risk sexual behavior, is the final pathway to HIV/AIDS, it is closely linked to various SDHs. 11 -22 For example, one study found that young African American women from economically disadvantaged neighborhoods who reported a lack of food at home, homelessness, and low perceived education and employment prospects had 2.2 to 4.7 times higher odds than those without these risk factors for reporting multiple sex partners, risky sex partners (including older men and partners involved in gangs), substance use before sex, and exchange sex (ie, trading sex for goods and services). 23 Other evidence indicates that poverty and other structural factors create a risk environment that is conducive to HIV transmission and suboptimal engagement in HIV care among low-income African American people living with HIV. 24 -30 Research also suggests that improving education and affordable housing can reduce incidence rates of HIV and AIDS because low levels of education and unstable housing have been found to decrease social stability and increase HIV risk behaviors (eg, risky sex and drug use). 31 -34
Most studies addressing SDHs for HIV have focused on women 35,36 because of the vulnerability of many women to discriminatory social, economic, and political practices based on their sex. These studies reveal that interventions that strengthen women’s income, housing stability, and gender empowerment are associated with improved psychological well-being, economic productivity, and reduced HIV risk. 36,37 Interventions that address SDHs also have improved HIV outcomes for men. For example, an intervention with MSM, the Mpowerment Project, recognized that because young gay or bisexual men engage in unsafe sex for various reasons, focusing solely on one level of risk factors (eg, individual-level factors) would omit men who engage in unsafe sex for other reasons. By using a multilevel approach, the Mpowerment Project developed community-level and individual-level capacity building and empowerment to reduce HIV-related risk behaviors in multiple communities in the United States in the 1990s. 38,39 Similarly, interventions that address social and economic barriers may also lead to improvements in health. For example, for homeless and unstably housed people living with HIV, a randomized controlled trial conducted from 2004 to 2007 found that the receipt of stable housing reduced risk behavior, improved access to care, and increased adherence to medication regimens among people who received the intervention, compared with those who did not. 40
Improving access to care and enhancing the quality of care can also contribute to reducing disparities in the incidence of HIV. Racial/ethnic stereotypes are deeply embedded in American culture and, whether consciously or not, can adversely affect the care that providers give to their patients. 41 Interventions that address implicit bias and the cultural gaps between providers and patients can improve the quality of care and reduce racial/ethnic disparities in HIV outcomes. A 2007 study found no racial/ethnic disparities in the receipt of antiretroviral therapy, patient self-efficacy, and viral suppression when providers scored high on a novel measure of cultural competence. 42 Other evidence indicates that interventions can reduce implicit and explicit bias among providers and others. 43,44 The scarcity of health care providers from underrepresented racial/ethnic minority groups may also affect care. In 2012, only 3.8% of all practicing physicians were African American and 5.2% were Latino. 45
Social Determinants, HIV/AIDS, and CAPUS
An emerging body of scientific evidence suggests that addressing SDHs must be an essential part of a comprehensive response to HIV/AIDS. 36,46 -51 Public health experts recognize that shifting the focus from one that emphasizes only behavioral change to one that emphasizes SDHs could address key structural drivers of HIV/AIDS vulnerability. 36,51 A focus on SDHs could be the game changer needed to reframe the HIV/AIDS response at the national level and at last eradicate HIV/AIDS inequities. The premise of CAPUS was that all health-related behavior, including risk behaviors for HIV/AIDS, must be understood as a function of individuals within their environments, which either promote or decrease exposure to risk factors for infection. 1 The higher rates of morbidity and mortality for HIV/AIDS observed among racial/ethnic minority populations are, in part, a product of social and physical conditions that underlie patterns of behavior. 11 -31 CAPUS focused on the idea that HIV interventions that focus narrowly on individual behavior change and/or pharmaceutical interventions cannot effectively address the magnitude and complexity of disparities in HIV. 36,51 Accordingly, whenever feasible, SDHs need to be incorporated into behavioral and biomedical strategies to increase their likelihood of success, and a new generation of HIV interventions focused on the fundamental SDHs should be the centerpiece of efforts to address HIV-related disparities.
The premise of CAPUS was supported by scientific evidence indicating that policies across multiple sectors shape social conditions, which influence risk behaviors and, thus, increase vulnerability to HIV and affect population health and health equity. 19,52 It is therefore important to integrate the Health in All Policies approach to have the widest impact on SDHs and population health. This approach recognizes that every aspect of government and the economy has the potential to affect health and health equity, including finance, education, housing, employment, transportation, and health. 53,54
Economic studies also support the premise of CAPUS. Most interventions focused on SDHs that have been rigorously evaluated have been shown to be cost effective and to save society money in the long run. 55 For example, the Mpowerment Project resulted in savings of $700 000 to $900 000 during a 5-year period. It showed that the cost of HIV prevention using a comprehensive SDH approach to HIV was much lower than the cost of lifetime medical treatment of HIV. 38
Recommendations for Future Research
We recommend several priorities for future research. One recommendation is to better understand the dynamic nature of stigma and how stigmas linked to race/ethnicity (HIV itself, sexual orientation, transgender identity or expression, illicit drug use, sex work, incarceration, and immigration) can vary for the same individual across contexts and can interact with one another to affect racial/ethnic HIV-related disparities. Research also is needed to better understand how to build resilience and resistance in individuals and communities to protect them from the negative effects of these stigmas. 56
A second recommendation is to better understand the extent to which SDHs can contribute to reducing the racial/ethnic inequities in initiation, uptake, and adherence to preexposure prophylaxis (PrEP) against HIV/AIDS. 57 -59 In one study, medical students rated black MSM patients as more likely than white MSM patients to engage in increased unprotected sex if prescribed PrEP, which, in turn, was associated with medical students’ reduced willingness to prescribe PrEP to black MSM patients. 57 Future research could help identify how interventions that address SDHs can contribute to reducing racial/ethnic disparities in PrEP awareness, access, affordability, use, and provider bias.
A third recommendation is to maximize the impact of SDH interventions. 60 For example, research suggests that improving housing and neighborhood quality can reduce HIV risk, 36,40 but it is not clear which aspects of housing and neighborhood quality improvements lead to these reductions and the extent to which key components of comprehensive SDH interventions can be modified to achieve greater impact. Similarly, a firm empirical base is currently unavailable to determine which SDH strategies designed to reduce HIV/AIDS–related disparities are likely to have the greatest impact, which domains should be tackled first, and the extent to which features of interventions (eg, intensity and timing) can lead to differential effects. Future research should identify the relative costs and benefits of promising SDH interventions so that policy makers can fund those that are likely to have the greatest impact on HIV/AIDS.
A final recommendation, given the high risk of HIV/AIDS among MSM, is to develop and evaluate more SDH interventions for men and boys. A 2017 study of the biggest concerns of young adults (aged 18-24) in racial/ethnic minority groups who are at risk for HIV, including MSM, revealed that concerns about aggressive policing, high levels of community violence, and unstable housing led them to live with constant threat and fear, high levels of hopelessness, low perceived economic opportunity, and a desire to live in the moment given the uncertainty of the future. 61 Thus, interventions are needed to develop self-esteem, job readiness, and service-learning opportunities among members of this sociodemographic group.
Public Health Implications
Addressing the SDHs of HIV has the potential to reduce the risk of other major diseases in the United States. A 2017 report from the National Academies of Sciences, Engineering, and Medicine called for multiple strategies to create sustainable financial models to promote improved population health through a focus on SDHs. These strategies included raising awareness among the public and policy makers of the magnitude of the health challenge, the availability of an evidence base, and the shared benefits that would accrue to multiple sectors of society from such investments. 62
The growing recognition that health policy involves all sectors of society that have health consequences means that the health sector can work collaboratively with other sectors of society. 53,54 An emerging body of evidence suggests that tackling SDHs holds great promise for making strides in reducing HIV/AIDS–related disparities. 55,63 Implementing the Health in All Policies approach requires the involvement and coordination of several policy sectors to ensure policy coherence and achieve the overall objective of reducing health inequities through tackling SDHs. 63 This policymaking process by various stakeholders requires representation of the perspectives and contexts of those most affected by health inequities. Thus, the engagement of civil society and affected communities in particular is necessary. The SDH framework provides direction to tackle health inequities by promoting equitable social, economic, and environmental conditions to achieve optimal health and well-being for all. With political will, this “culture of health,” where everyone has the opportunity to make choices that lead to a healthy lifestyle, is achievable. 64
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.