
Abstract
There is a lack of nutritional programming and resources available for people living with HIV/AIDS (PLWHA) in Nova Scotia, Canada. This is problematic for several reasons, including that adequate food and nutrition knowledge is integrated to effective medical therapy and wellness for PLWHA. The aim of this research was to explore and describe the beliefs, values, and experiences of HIV-service providers involved programming for PLWHA in Nova Scotia. Using a post-structuralist lens, semi-structured interviews were conducted with nine service providers. Thematic analysis of interview transcripts identified four main themes: (1) recognizing the social determinants of health, (2) acknowledging and disrupting layered stigma, (3) understanding the commensality, and (4) navigating and utilizing networks of care. These findings suggest that those developing, delivering, and evaluating food and nutrition-related programming must engage in community-inclusive approaches that recognize the varied social determinants of health that shape the lived of PLWHA, leverage existing networks and resources, and actively disrupt layered stigma. Also, in agreement with existing evidence, participants stressed the value of communicating and supporting the practice of eating together (commensality) and cultivating networks of care.
Human immunodeficiency virus (HIV) is often defined by a host of comorbidities, including pneumonia, cancer, and other opportunistic infections. HIV can develop into acquired immunodeficiency syndrome (AIDS), which is directly associated with increased morbidity and mortality (Willig et al., 2018). With advances in care, including antiretroviral therapy, people living with HIV/AIDS (PLWHA) are now living longer, and experiencing increased quality of life, in comparison to previous decades (Trickey et al., 2017). Consequently, PLWHA are striving to (re)define their own wellness and quality of life.
Nutrition status has been identified as a key factor in wellness outcomes (Coyne-Meyers & Trombley, 2004; Raymond & Morrow, 2021); a status that can be impacted by a host of medical and social determinants of health including include income, education, and employment (Raymond & Morrow, 2021; Willig et al., 2018). Optimal nutrition status in combination with antiretroviral therapy is associated with immune system resilience, and therefore influences the progression of HIV to AIDS (Raymond & Morrow, 2021; Willig et al., 2018). Interactions between nutrients and antiretroviral therapy, however, are a common experience for PLWHA. These interactions can lower treatment efficacy and may cause additional or worsening signs and symptoms that can compromise the nutritional status of an individual (Coyne-Meyers & Trombley, 2004; Willig et al., 2018).
In both resource-poor and resource-rich settings, mortality rates are increased for PLWHA who are malnourished (Willig et al., 2018). In high resource settings, such as Canada and the United States, 49% to 71% of PLWHA experience food insecurity (Slater et al., 2015). PLWHA who have access to safe and nutritious foods experience reduced symptoms of illness, decreased risk of comorbidities, improved strength and adherence to antiretroviral therapy medications, and an improved quality of life (Willig et al., 2018). The economic status of PLWHA is influenced by HIV-related stigma that can impact ability to purchase nutritious foods (Logie et al., 2018). Stigma for PLWHA may manifest in the form of food insecurity, discrimination, and social exclusion, which drastically lowers their likeliness of accessing food, medical care, and social supports (Logie et al., 2018).
The Nova Scotia Advisory Commission on AIDS (NSACA, 2014) reports that services provided for PLWHA in Nova Scotia, Canada, are inaccessible and underfunded. Available programming lacks consideration of diet diversity, specifically those diets consumed due to personal, religious, or cultural reasons. Further barriers to participating in services included long waitlists for programs, stigma, and lack of services in rural areas (NSACA, 2014). As programming specific to the nutritional needs of food insecure PLWHA are essential access points for those seeking support (Koehn et al., 2020), there is a need to further investigate the experiences in program facilitation from those developing, providing, and evaluating programming for PLWHA. Through this research we aimed to explore the beliefs, values, and experiences of HIV/AIDS service providers offering programming for PLWHA in Nova Scotia to gain insights into the complexity of health promotion programs in Nova Scotia and how food and nutrition programming can be best designed for optimal benefits for PLWHA.
Methodology
Project Context
FoodNow is a multi-phased project focused on the nutrition and foods needs of PLWHA using integrative knowledge translation (Gagliardi et al., 2015). FoodNow takes a community-based approach to include PLWHA and service providers in the research directly (Green & Mercer, 2001). The overall objectives of our research are to explore current barriers and facilitators for participating in food and nutrition programming, engage in knowledge exchange and discussion with rights and title holders, collaborators, and end-users, and identify ways programming can be designed to improve the health of PLWHA in Nova Scotia.
Integrated into each phase of the FoodNOW project, is the research team’s commitment to the knowledge-to-action cycle (Graham et al., 2006). In a cyclical pattern, we evaluate outcomes, identify problems, assess barriers, adapt to local contexts, implement interventions, and begin again (Graham et al., 2006). Phase 1 was a scoping review that outlines the available programming for PLWHA across Canada (Mannette et al., 2022). Phase 2 involved the virtual food costing of a healthy diet for PLWHA within Canada. Virtual food costing used online supermarket food prices and simulated households (each with a PLWHA) to determine the cost of a basic nutritious diet for PLWHA in addition to other household expenses (Clarke et al., 2023). The current study is part of Phase 3 that explores qualitatively food and nutrition programming for PLWHA in Nova Scotia.
Conceptual Framework
A post-structuralist theoretical lens guided this research. Recognizing that experiences and identities are socially constructed (Scott, 1991), post-structuralism acknowledges that the way we understand and operate within the world is the result of the interrelationships between power relations, discourses, and knowledge (Foucault, 1977, 1978). Within this research, post-structuralism facilitated the critical exploration of the interconnected systems of social meanings, practices, and discourses of HIV and nutrition that shape food and nutrition health promotion and programs for PLWHA.
Within a post-structuralist theoretical lens, the results are influenced by the researchers (Darwin Holmes, 2020). We do not identify as people living with HIV and are therefore outsiders to the HIV/AIDS community. The authors acknowledge the societal constructs stemming from HIV-related discourses, such as the avoidance and isolation of PLWHA, and their privileged positions within these constructs as outsiders. The team consists of health researchers in the areas of dietetics, food studies, and health promotion. Several team members identify as, and work with, populations who have been historically marginalized.
Recruitment and Data Collection
Inclusion criteria for participation included currently working as a service provider in Nova Scotia, providing care, support, and/or resources to PLWHA. Participants were recruited through individual invitations to service providers via e-mail. Semi-structured interview questions were developed based on available literature reporting the needs of PLWHA and their service providers and designed using the post-structuralist lens of the research, with feedback integrated from service providers. The interview questions explored the experiences of HIV/AIDS service providers in facilitating programming within their organizations, with a particular focus on food and nutrition programming. In brief, participants were asked to describe barriers and facilitators to programming and how food and nutrition programming could be more effectively designed to improve health and wellbeing of PLWHA. Ethics clearance for this study was obtained from the university research ethics board at Mount Saint Vincent University.
Data Analysis
The interviews were transcribed verbatim and analyzed using thematic analysis as described by Braun and Clarke (2006). Thematic analysis is well aligned with many theoretical paradigms, including post-structuralism (Braun & Clarke, 2014). Within post-structural research, thematic analysis seeks to understand the socio-cultural contexts that constitute the experiences of individuals (Braun & Clarke, 2006); specifically for this study, food and nutrition programming.
Analysis of this qualitative research was guided by Richardson (2003), who noted that multiple angles of approach allow for the multidimensionality of the research to explore. Our angles of approach included the following: (1) interview transcripts and notes were analyzed, (2) data were independently coded by two trained reviewers, and (3) themes were finalized through a collaborative process with all co-authors. Any discrepancies were resolved between the researchers through repeated reviews of the data and discussion.
Results
Nine service providers were interviewed (see Table 1 for participant demographics). Participants held various roles, including 2SLGBTQIA+ program leaders, Indigenous (First Nations, Métis, Inuit) PLWHA community service providers, support personnel for harm reduction programs (e.g., safe drug-use and housing), coordinators for systems navigation, leaders in HIV policy development, and health care professionals involved in clinic programs specifically for PLWHA. Participants were located mainly in Halifax, while two were located outside the city in a rural area of the province. One service provider specified that while their program is based in Halifax, they do weekly rotating outreaches in several rural areas of the province. Through data gathered with participants, we identified four main themes to consider in designing effective food and nutrition programs within the Nova Scotian context where the service providers work.
Demographic Data of Service Providers (n = 9)
Theme 1: Recognizing the Social Determinants of Health
Many of the service providers highlighted that the social determinants of health, such as income and social protection, food security, housing with basic amenities, and social inclusion, greatly impact the specific needs of PLWHA who access programming in Nova Scotia. Participants noted that many of their clients self-identify within groups that have been historically marginalized and that face many complex issues, including racism, homophobia, ageism, lack of education, food insecurity, and poverty. This means that developing tailored food-and-nutrition-related programming is not simply about food and nutrition but also must recognize and address other social determinants of health. One participant noted that . . . People [accessing programming] are in very challenging situations and their needs are very complex . . . these problems are tricky and deep and we [service providers] don't have a bottomless pit of money, but we really need to start addressing our social determinants of health in a more meaningful way and not tool around the edges. (Participant 2)
Another service provider highlighted more specifically that housing insecurity and poverty are of great concern for the PLWHA whom access their services, stating, . . . I know that they [PLWHA] can have significant challenges . . . needing to take medication with food and not always having access to food. A lot of people [PLWHA] that I work with regularly are housing insecure or living in poverty. . . . There's only so much money for them [PLWHA] to spend, so we can't be teaching them [PLWHA] really expensive recipes, so we have to tailor the program based on people’s needs. (Participant 3)
This participant also emphasized the need for programming to be relevant to the targeted community, for example, ensuring participants can access the sources of nutrition that are recommended to them. It was echoed by almost all participants for “programming that can be tailored to cover folks’ experiences” (Participant 1) as key to offering food and nutrition programming for PLWHA. Service providers also observed that PLWHA who face housing insecurity and poverty are struggling with “competing priorities” (Participant 2) in meeting their needs, and value programming that helps fulfill basic needs, such as food provisions, hygiene supplies, and shelter, in lieu of nutritional education programming.
Theme 2: Acknowledging and Disrupting Layered Stigma
PLWHA have been historically stigmatized, which has incited fear of judgment while accessing health promotion programming (Logie et al., 2018). Participants noted that HIV-related stigma in Nova Scotia is still a very real concern and may impede PLWHA’s participation in programming. Thus, HIV-related stigma needs to be considered in order to be disrupted when designing food and nutrition programming. Participant 6 stated that HIV-related stigma in Nova Scotia is “definitely still real,” and went on to say that many service providers are beginning to integrate awareness of stigma into their programming, but the cumulative nature of stigma(s) creates a barrier that is difficult to erode. However, many participants recognized that HIV-related stigma is “layered”: Well stigma . . . It’s an awful beast, you know. Because it [stigma] causes people to feel reluctant to access services that they need. People fear being judged. Whether because they have an infection like HIV, which is highly stigmatized mostly because of how you get it, and any other parts of their social identities . . . like the layered stigma, right? So, it [layered stigma] adds all these different barriers [to accessing programming]. (Participant 2)
As Participant 2 noted, “layered stigma” is the cumulative stigma related to the various identities of PLWHA accessing programming. An example of “layered stigma” specific to Indigenous PLWHA was noted by Participant 7, In Canada, Indigenous people seeking healthcare are stigmatized for being Indigenous people seeking services, basically, right? So, you can't really untangle that [stigma] from Indigenous people living with HIV seeking services. I think that there's compounding factors there within the intersections of identities . . . (Participant 7)
In this quote, Indigeneity, racism, and stigma were all social determinants of health among PLWHA that were recognized as major influences on engagement and use of services.
Theme 3: Understanding Commensality
The act of sharing and eating food together is known as “commensality” (Danesi, 2018). Several participants recognized the communal and social connections associated with sharing food, otherwise known as commensality, as important for food and nutrition programming design. As one participant explained, . . . the biggest benefit [of food programming] is the relationship aspect of it, so there's definitely something to be said about offering food as just a kind gesture and a connection with people. So, when people come in and they're brand new here, and maybe they are a little anxious or uncertain . . . It's really nice to be able to say, “hey, do you want a snack?” It just kind of breaks the ice, and not to say that a granola bar would be a consolation prize if somebody is trying to get into housing . . . But, if somebody is having a bad day or you can’t help them with many things, we can always offer them a snack. (Participant 6)
Participants noted that many of their clients often feel isolated and believed food was a versatile tool for recruitment, engagement, and building relationships with PLWHA, especially with clients living with food insecurity and/or those seeking social connection(s). Due to its value and versatility, commensality was believed essential for food and nutrition programming.
A loss in the sharing and connection was felt while programs were offered online due to the COVID-19 pandemic, which prompted some participants to use novel methods of food provision programming, such as ordering food and meal delivery for each program participant. One participant mentioned, . . . when I do a lot of my programming online, we will do meals together. I had a little form people fill out and then I get them food delivered via Uber Eats or Skip the Dishes or something. Just because I know that, especially for younger people, a free meal, like having to not pay for one meal a week is a huge savings for them . . . the communal nature of food is something we forget, right? (. . .) The communal and social connection of food is hard to deny. And that [communal connection] is something that I think we [service providers] need to encourage . . . (Participant 4)
Participants also noted benefits and barriers to food delivery during the COVID-19 pandemic related to commensality and sociability. A few participants explained that programming offered virtually could not fully replicate connections and engagement with the community in comparison to in-person offerings. In addition, virtual programming was exclusive to PLWHA with access to reliable technology and internet connection. Some participants, however, did acknowledge the benefits of virtual programming in increasing outreach to PLWHA living in rural communities or with dependents, who would likely not have attended if programming was offered exclusively in-person.
Theme 4: Navigating and Utilizing Networks of Care
As most of the participants described a network of care in Nova Scotia exists and consists primarily of non-profit service providers and clinics, who “are very stretched” (Participant 2). Some participants noted that the availability of supportive programming in Nova Scotia can be inconsistent, primarily due to funding and associated restrictions. To ensure the PLWHA community has consistent access to programs that help with basic needs including food, most participants mentioned they often provide systems navigation of other programs, such as shelters, food provisions, government funding, and medication-coverage: We do a lot of systems navigation, helping a number of people [living with HIV/AIDS] connect to food banks in different parts of the province . . . and also connecting people to soup kitchens or breakfast programs. And we have a drop-in food program, it’s mostly in the form of snacks and nutrition supplement beverages like Ensure or Boost. . . . We get clients who are used to ASOs [AIDS Service Organizations] from bigger regions like Ontario and Quebec, and then find themselves here. (Participant 3)
As this participant noted, PLWHA arriving from other largely populated Canadian provinces such as Ontario or Quebec have expressed their disappointment and shock to service providers regarding the lack of supportive programming (e.g., food vouchers) available to them in Nova Scotia.
A few participants mentioned that they have co-developed a network of services across the province in attempt to provide consistent supportive programming to the community when resources run out: Organizations do band together to try to put things [support programs] together and support one another and link people to important services. But it's very challenging when there's limited funding for that [support programs], people [service providers] are very stretched, and the pandemic has just made it even more challenging. (Participant 2)
As many other participants noted, supportive programs for PLWHA are generally not the priority of provincial or federal funding. For a few participants, offering food-and-nutrition-related programming is only possible if additional funding and resources are available through local donations or private health care company funding: Unfortunately, Nova Scotia doesn’t provide a whole heck of a lot of funding overall, proportionately to what’s received from the federal government and federal government programs. . . . but direct service provision is not part of that [funding], and it's become more challenging to be eligible for federal funding under the new Community Action Fund. . . . there's not a lot of funding at their [service provider] discretion that can go towards [supportive] programs like that [support-related]. (Participant 2)
Food and nutrition program designers must recognize that, as this participant noted, funding for all HIV-related programming is challenging to secure and, therefore, they may need to navigate and utilizing the existing networks of care in Nova Scotia. Information about existing resources should also be available in food and nutrition programming. Some participants noted that food and nutrition support programming available in Nov Scotia can include free cell phones with prepaid minutes, food and meal provisions, and publicly available nutrition education materials to help with day-to-day expenses.
Discussion
Canada has implemented substantial efforts to slow down the spread of HIV, but there are still regions in which infection rates are high. One such area is Nova Scotia (Sinno et al., 2021). Nova Scotia is a small province in Canada, comprising only 2.6% of the Canadian population, according to the 2021 Census of Population (Government of Canada, 2022), In terms of HIV rates, as reported by Haddad et al. (2019), there was a 100% increase in HIV diagnoses between 2017 and 2018, from 15 new cases to 31, respectively in Nova Scotia. As Sinno et al. (2021) stated, “this increase is unparalleled by any other province or territory” (p. 158), and this trend seems to be continuing as the Nova Scotia Health Authority (2022) reported that an increase in people newly diagnosed with HIV in Nova Scotia occurred in 2022. Therefore, Nova Scotia has a need for programs that support the care of PLWHA, including the nutritional care of PLWHA.
The four themes we have highlighted are interconnected and overlap, as in Figure 1. The impact of the social determinants of health on participant engagement in programming is echoed in other Canadian research with PLWHA (Logie et al., 2018; Slater et al., 2015), indicating that tailored programming must consider assessment of the resources available to program participants. Our findings are consistent with reports from the work of Slater et al. (2015) based on their Canada-wide questionnaire of community-based food and nutrition service organizations for PLWHA. They found during their study that program gaps across the country included a need for increased food delivery to clients; new and/or expanded infrastructure (e.g., kitchens), and more staff dedicated to food programming exclusively (Slater et al., 2015).
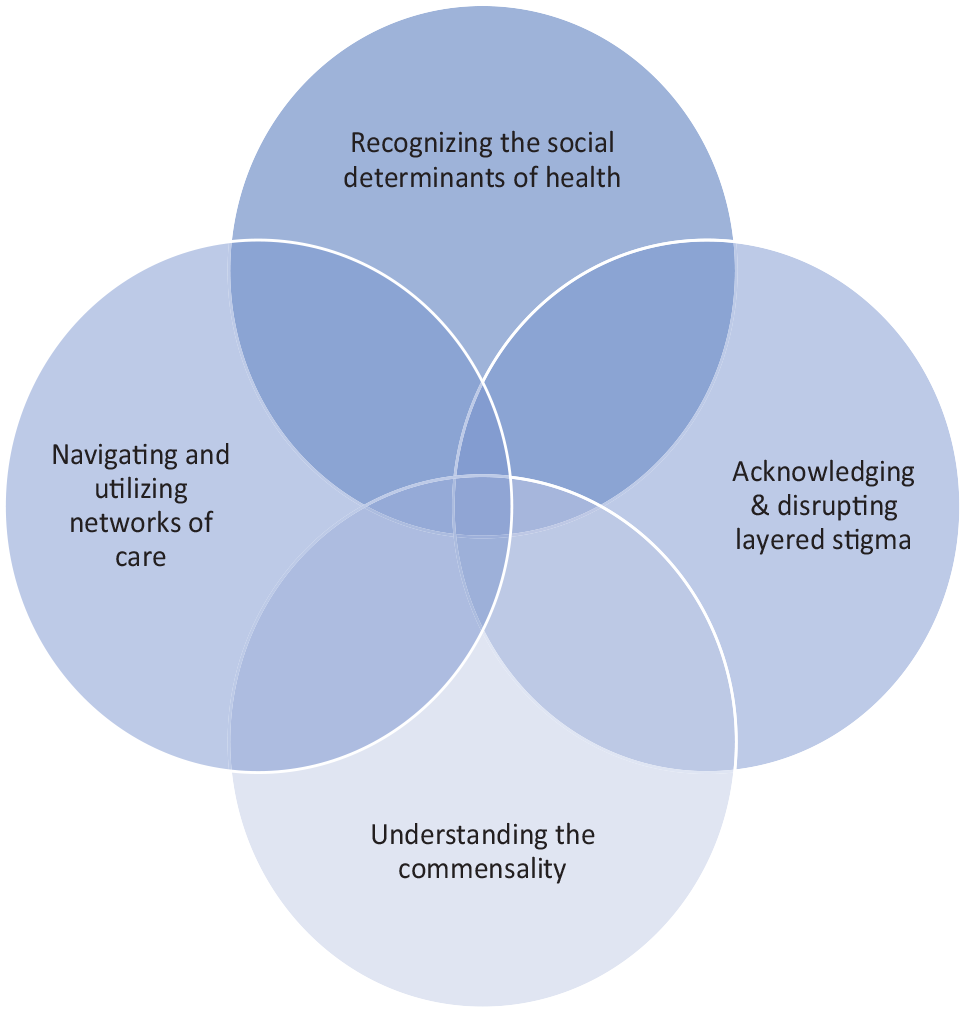
The Interconnected and Overlapping Themes From the Service Providers
HIV-related stigma has been linked to food insecurity and decreased access to social supports, which is particularly problematic for perpetuating cycles of food insecurity and HIV/AIDS (Weiser et al., 2011). Participants in this study noted the importance of addressing “layered stigma” within food and nutrition programming. Just as Danesi (2018) and Mintz and Du Bois (2002) note that sharing food can help people to better understand each other, create trust, reinforce relationships, and maintain safe spaces of belonging, our participants highlighted commensality as an important consideration for food-and-nutrition-related program design to break down barriers for PLWHA. Opportunities to develop relationships are of particular importance for PLWHA who have been historically isolated due to “layered stigma.” Food and nutrition programming designed to create social and safe spaces, to foster community, and to actively reduce stigma may encourage people to attend such programs and, in turn, positively influence the health of PLWHA.
Advancements in medications and therapies for PLWHA have changed the way people are living and aging with HIV (Boucher et al., 2019). Programming has been found to be unable to keep up with the support demands needed for people with chronic illnesses (Boucher et al., 2019), and the same may also be said for PLWHA in NS. As reported by the NSACA (2014), programming for PLWHA in Nova Scotia too often has long waitlists, struggles to addresses issues of stigma, displays inadequate cultural competence, and lacks funding for the training of service providers who are not HIV specialists.
Systems navigation of provincially available programming (or network of care) is currently the method in which PLWHA are receiving supportive programming. The NSACA (2014) recognizes that working together as a province to deliver the specialized programming that PLWHA need is beneficial as it can make best use of specialized/targeted programming offered. Lack of funding, however, is unfortunately most often the reason networks of care are being used in Nova Scotia (NSACA, 2014).
We note several considerations to this work for the reader to keep in mind. The sample size of this work may be considered by some researchers to be too small to provide generalizations, but we must remember that the aim of poststructural research is not to provide generalizations but to explore how the experiences of people are socially constructed (Scott, 1991). The concept of data saturation is not philosophically aligned with our research lens and is as Braun and Clarke (2021) noted is a construct of neopositivist thought. In other words, we believe that meaning is found in the interpretation of data not in the repetitive nature of data.
In this study, we sought to understand more fully the systems in which service provider in Nova Scotia, providing care, support, and/or resources to PLWHA operate and how such systems shape their work and food and nutrition programs. In other words, our study is contextual. This does not mean our results cannot be used by researchers, service providers, and policy makers in other places to examine the way food and nutrition programs for PLWHA are shaped in their areas. For example, although the networks of care may look different in Nova Scotia, service providers in other areas can examine their networks of care to see how they can contribute or be utilized to provide food and nutrition for their clients. We also note that the diversity within our sample is limited in both geography and representation. We acknowledge that some voices are missing from this discussion and suggest future studies could explore the differences between rural and urban organization or differences between organization in other Canadian provinces, as well as the experiences of the missing voices of this study.
Implications for Practice
Dietitians are trained to work with clients to change or modify some part of their diet, their eating behaviors, and their bodies. In a survey of dietitians in the United Kingdom, it was found that most dietitians perceived that communication skills for behavior change were critical for practice (Whitehead & Parkin, 2022). In an Australian study, dietitians reported that behavior change was fundamental to the practice of dietetics and saw the need for more education on the science of behavior change (Rigby et al., 2021). In Canada, Fraser and Brady (2018) reported that within dietetics education there is a prioritization of science-based knowledge and ways of knowing.
Many health promotion models focus on individual behavior changes and are rooted in motivational factors of behavior change. For example, the health promotion model as developed by Pender (1982), asserts that complex biopsychosocial factors motivate individuals toward health-enhancing behaviors (Alligood, 2017). Although Pender’s model of health promotion does recognize the key concept of social, cultural, and physical contexts in which people find themselves it still suggests that the “environment can be manipulated by the individual to create a positive context of cues and facilitators for health-enhancing behaviours” (Pender, 2011, p. 3). Such models often fail to fully recognize the systemic economic, political, and social factors (such as stigma) that can make behavior change next to impossible for some individuals. For example, in our previous work (Clarke et al., 2023), we determined that PLWHA living in Nova Scotia, both individuals and families, cannot not afford to buy healthy foods as outlined by the Canadian nutritious food basket. Behavior change for the individual becomes very difficult if there is no money to purchase healthy foods.
The interviews in this study provided knowledge and insight into the realities of available programming and resources for PLWHA, and themes identified offer ideas to improve current programming moving forward. “Upstream” or social, political, and economic changes are needed for effective health promoting nutritional and food programs for PLWHA. The service providers in this research recognized this as the discussed social determinants of health, the impact of stigma, and utilized existing (often under-funded and over-taxed) networks of care. Systematic change is needed within the governmental funding structure to better support the sustainable and meaningful implementation of these services. This study also points to the importance of building a sense of community within programming to reduce shame and stigma. Further, programming that is designed with social determinant of health at the forefront is necessary for the respectful inclusion of all voices toward disrupting stigma and creating system change. To implement the above, we recommend funding be allocated toward the effective creation and evaluation of a new food programming model(s) that considers the needs addressed throughout this study.
We also must begin to train dietitians to be able to create and implement programs that consider the themes discussed by our participants. Social justice advocacy, or the fair distribution of resources and responsibilities, that can help to address the root causes of health disparities, is missing from accredited, English-speaking dietitian training programs in Canada (Fraser & Brady, 2018). Therefore, dietetic educators need to understand not only how knowledge, relations of power, and social discourses shape nutritional health for PLWHA (as in our post-structuralist perspectives) but also need to be able to translate this understanding to inform health setting and community programs rooted in principles of individual-level behavior change in which many dietitians operate. We suggest that dietetic training that encourages students to understand the relationship of social justice advocacy and individual behavior change models could help dietitians plan and implement food and nutrition programs for PLWHA that incorporate the themes discussed by our participants.
With further research, our findings may be used to inform the development of tailored food and nutrition programming as observed by service providers who work most closely with this population group and can assist in the design and implementation of health promotion programs appropriate to the wants and needs of PLWHA in Nova Scotia and beyond.
Conclusion
Given the findings of this research, we have learned four key factors to take into consideration when developing food and nutrition programming for PLWHA in Nova Scotia. We recommend that service providers and those who fund programming assess the resources and identities in the communities they serve and consider the merit of commensality in program delivery. Addressing social determinants of health and “layered stigma” in programming is also critical for programming to be effective and fully reflect the diverse needs of PLWHA. Future research should include engaging directly with PLWHA, with an intentional focus on populations who have been historically marginalized including PLWHA who identify as Black, Indigenous, and other people of color, while exploring their experiences in accessing programs available in Nova Scotia.
Footnotes
Authors’ Note:
We would like to thank all the service providers and organizations for their partnership and guidance throughout this project, and assistance in participant recruitment. We would also like to thank Chelsey Purdy and Gloria Chinonso Acholonu for providing contributions as student researchers on this work. This work was funded by Research Nova Scotia (ResearchNS).