
Abstract
Objectives:
The objectives of this study were to (1) determine the degree of alignment between an existing public health curricula and disease intervention specialist (DIS) workforce training needs, (2) assess the appropriateness of public health education for DISs, and (3) identify existing curriculum gaps to inform future DIS training efforts.
Methods:
Using the iterative comparison analysis process of crosswalking, we compared DIS job tasks and knowledge competencies across a standard Council on Education for Public Health (CEPH)-accredited bachelor of science in public health (BSPH) and master of public health (MPH) program core curricula offered by the Georgia Southern University Jiann-Ping Hsu College of Public Health. Four researchers independently coded each DIS task and competency as addressed or not in the curriculum and then discussed all matches and non-matches between coders. Researchers consulted course instructors when necessary, and discussion between researchers continued until agreement was reached on coding.
Results:
The BSPH curriculum aligned with 75% of the DIS job tasks and 42% of the DIS knowledge competencies. The MPH core curriculum aligned with 55% of the job tasks and 40% of the DIS knowledge competencies. Seven job tasks and 9 knowledge competencies were considered unique to a DIS and would require on-the-job training.
Conclusions:
Findings suggest that an accredited public health academic program, grounded in CEPH competencies, could address multiple components of DIS educational preparation. Similar analyses should be conducted at other CEPH-accredited schools and programs of public health to account for variations in curriculum.
Keywords
Disease intervention specialists (DISs) conduct many tasks related to preventing the transmission of communicable diseases, such as HIV and other sexually transmitted infections (STIs). For example, DISs trace and then contact sexual partners of people diagnosed with STIs to ensure that they are evaluated and treated, thus reducing the likelihood of further transmission. 1 -3 DISs also perform field investigations, such as contacting people who test positive for HIV but do not return for posttest counseling, or identifying and contacting people with HIV who are not in care. 4,5 DISs are often based in state or local health departments, although an increasing number of DISs are in clinics, where they conduct interviews to obtain information on sexual partners and their locations. 6 The current DIS workforce in the United States, including community-based front-line workers and supervisors, is estimated to be 2063. 7 DIS work involves the use of skills typically found within 2 areas of concentration in public health training programs: (1) health education and promotion and (2) epidemiology.
DISs are an integral part of the public health workforce, and because of the evolving role they play, focused training and skill development are necessary. Challenges in pursuing improvements in DIS workforce training include determining where to start and how to focus efforts. In its 2017 Job Task Analysis and Test Specifications Report, the Public Health Accreditation Board identified the diverse experiential and educational backgrounds from which DISs enter the public health workforce as a barrier to developing national DIS certification criteria. 8 DIS training has historically relied on various nonstandardized approaches involving both formal education and on-the-job experience. Evaluating and, if needed, standardizing the educational curriculum for those pursuing a career as a DIS may be one starting point for addressing DIS workforce training deficiencies.
The 2003 Institute of Medicine report, Who Will Keep the Public Healthy? Educating Public Health Professionals for the 21st Century, recommended that academic public health programs embrace an ecological approach to curriculum development and educational delivery. 9 The authors noted that this approach, which involves an awareness that health and well-being are affected by the interactions among multiple determinants of health, should contribute to the development of a competent public health and personal health care workforce. Others have maintained that to effectively train the public health workforce, it is essential to engage in an intentional and systematic review of public health educational delivery, while also focusing on the emerging needs of the public health practice community. 10 -12 The call to action in the 2003 Institute of Medicine report highlighted the need for both the nation’s academic training programs and the public health practice–based community to promote a culture of continuous quality improvement and workforce development. 13,14
One way to evaluate whether academic public health training programs have the required content to effectively train a workforce is to conduct a gap analysis. 15 The goal of such an analysis is to identify gaps between educational curricula and necessary workforce knowledge and skills. It is an approach that results in the grounding of strategies and policies for workforce training in public health practice. Our objective was to conduct a gap analysis to determine and quantify the gaps between the public health training currently available in one accredited college of public health, and the job tasks and knowledge competencies required of a competent DIS workforce. Determining the degree of alignment between the content of public health curricula and the job tasks and knowledge competencies needed by the DIS workforce may inform future DIS education and training strategies and policies.
Methods
Our gap analysis involved 5 steps: (1) outlining and validating the scope and objectives of the gap analysis through consultation with a Public Health Accreditation Board representative, (2) becoming familiar with and mapping the DIS workforce job tasks and knowledge competencies specified by the Accreditation Board’s Job Task Analysis and Test Specifications Report 8 ; (3) reviewing course syllabi and materials from the Council on Education for Public Health (CEPH)–accredited Jiann-Ping Hsu College of Public Health curriculum, to become familiar with and map the skills and knowledge offered within its core curriculum; (4) identifying gaps between the Jiann-Ping Hsu College of Public Health curriculum content and DIS workforce job tasks and knowledge competencies by using a crosswalk methodology (in which we were able to observe sufficient commonality of items across the curriculum and task or competencies) 16 ; and (5) assigning to each identified gap 1 or more of 3 strategies (course, practicum, or on-the-job training) that could help align curricula with job tasks and/or knowledge competencies (Table 1). This research was reviewed by the Georgia Southern University Institutional Review Board and was approved as non–human subjects research.
Methodological steps in a gap analysis of core curricula for disease intervention specialist training
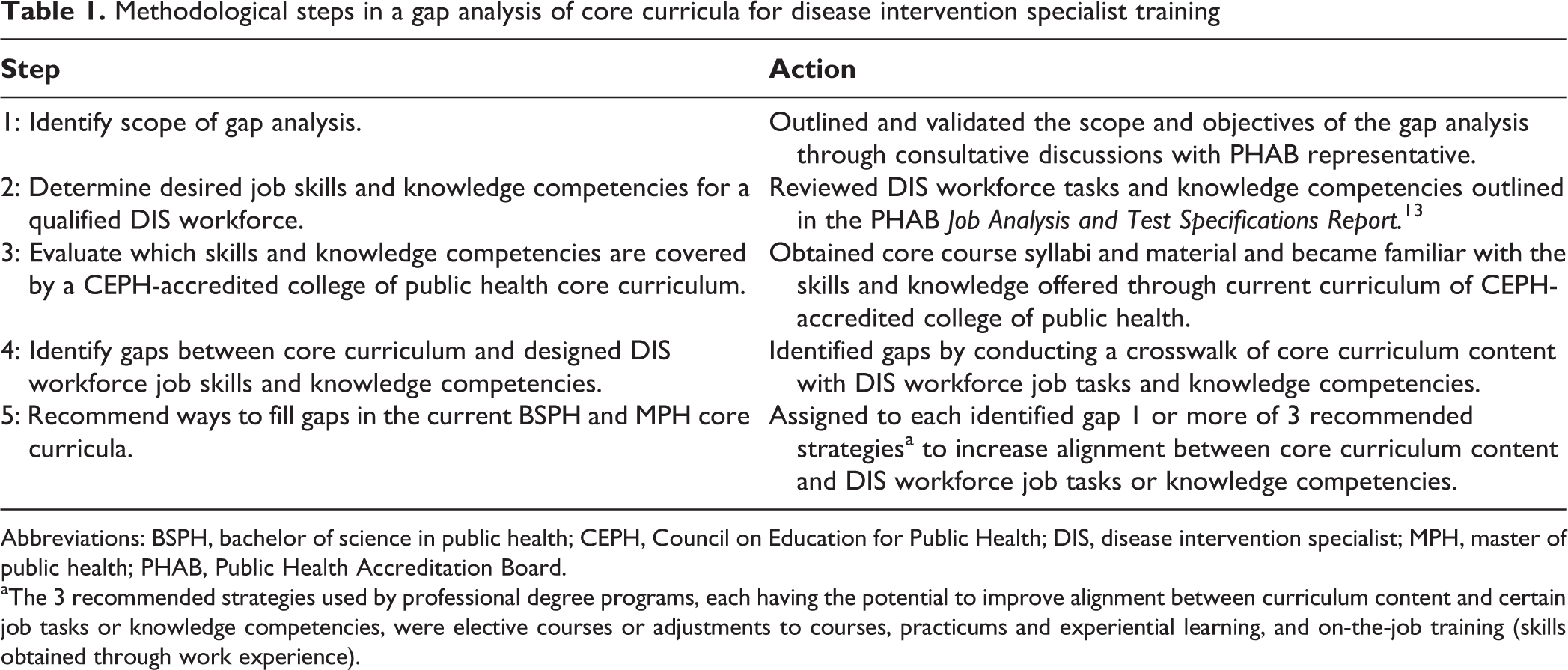
Abbreviations: BSPH, bachelor of science in public health; CEPH, Council on Education for Public Health; DIS, disease intervention specialist; MPH, master of public health; PHAB, Public Health Accreditation Board.
aThe 3 recommended strategies used by professional degree programs, each having the potential to improve alignment between curriculum content and certain job tasks or knowledge competencies, were elective courses or adjustments to courses, practicums and experiential learning, and on-the-job training (skills obtained through work experience).
In step 1, we worked in consultation with a representative from the Public Health Accreditation Board to create a plan for the analysis and ensure that all the documentation needed to conduct the analysis was available.
In step 2, we examined the Job Task Analysis Report to determine the job tasks and knowledge competencies needed for appropriately qualified DISs. We organized the data in the report into 2 broad categories: (1) job tasks (56 tasks within 9 domains) and (2) knowledge competencies (103 competencies within 10 domains).
In step 3, we determined which DIS job tasks and knowledge competencies were addressed in 2 academic public health training programs at Georgia Southern University Jiann-Ping Hsu College of Public Health. We collected information about course objectives, competencies, activities, and assignments for all courses listed in Table 2. First, we reviewed the syllabi for the core courses of the bachelor of science in public health (BSPH) degree program (with a major in health education and promotion). Second, we reviewed the syllabi for the core courses of the master of public health (MPH) degree program. The core courses of both degree programs address the foundational competencies required by CEPH for program accreditation.
Core curriculum coursesa for the health education and promotion BSPH degree and MPH degree programs at the Georgia Southern University Jiann-Ping Hsu College of Public Health
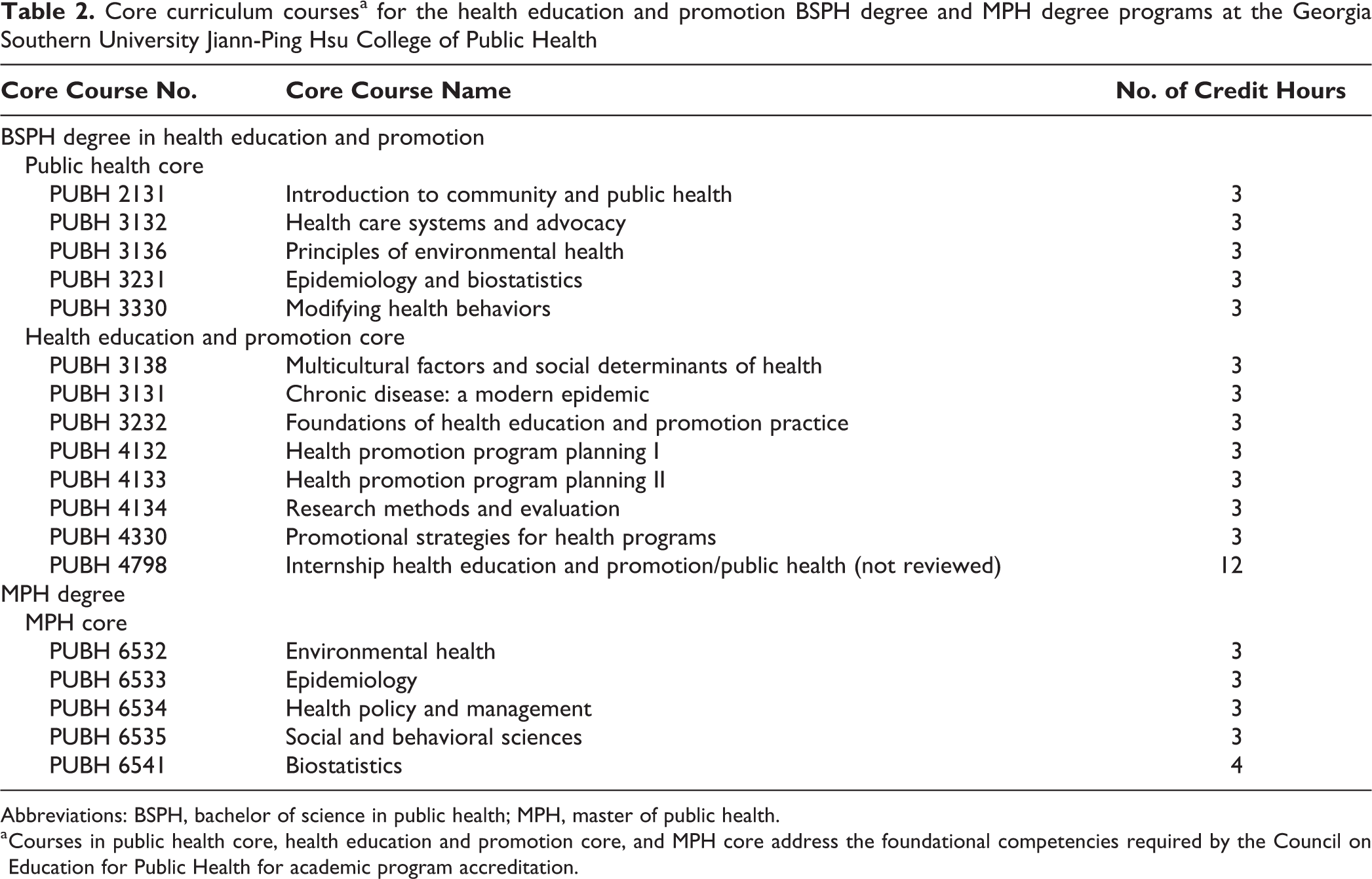
Abbreviations: BSPH, bachelor of science in public health; MPH, master of public health.
a Courses in public health core, health education and promotion core, and MPH core address the foundational competencies required by the Council on Education for Public Health for academic program accreditation.
In step 4, we performed a gap analysis by using methods articulated by Creswell. 17 We, the research team that conducted the mapping, included 4 university faculty members trained in both quantitative and qualitative analysis methods. We became familiar with all DIS job tasks and knowledge competencies, as well as with all core course content. During the gap analysis, 2 researchers performed the coding for job tasks and 2 researchers performed the coding for knowledge competencies. To mitigate the risk of “drifting” (ie, forcing a match between course content and job tasks or knowledge competencies when none existed), each set of researchers discussed and resolved any mapping disagreements. In addition to this iterative comparison process, we also made notes to justify matches, particularly when matching was not straightforward.
The gap analysis included the following elements: Independent mapping: Of the 4 researchers, 2 independently mapped the 56 DIS job tasks by cross-referencing them with BSPH core course content and then separately with MPH core course content. The other 2 researchers independently mapped the 103 DIS knowledge competencies with BSPH core course content and then separately with MPH core course content. Consensus mapping: Each pair of researchers then met and systematically compared their coding of each DIS task and knowledge competency to determine inter-rater agreement. If both researchers agreed on a match between a DIS job task or knowledge competency and course content, it was accepted. If they did not agree, they compared notes and resolved disagreements by discussing the reasoning for the coding (eg, which component of the course syllabus covered the job task or knowledge competency in question). When researchers disagreed, the course instructor resolved the disagreement. Gap identification: The team that had coded the DIS job tasks and the team that had coded the DIS knowledge competencies each grouped its results into 2 categories: job tasks and knowledge competencies aligned with the BSPH or MPH courses and those not aligned with the BSPH or MPH courses, the latter representing the gaps between course content and certain job tasks or knowledge competencies.
In step 5, the research team discussed and assigned to each identified gap 1 or more of 3 recommended strategies used by professional degree programs, each having the potential to improve the alignment between courses and certain job tasks or knowledge competencies. The 3 strategies were elective courses, practicums and experiential learning, and on-the-job training (ie, skills obtained through work experience). We recommended an elective course when alignment could be accomplished by the student taking a guided elective course or by the instructor or college infusing DIS-specific components (ie, online module, lecture, or activity) into the content of a current course in the curriculum. We recommended a practicum when the DIS job task or knowledge competency was too specific for a course and when alignment could be accomplished by the student seeking a practicum site where certain job tasks could be practiced or knowledge competencies could be learned. Finally, we recommended on-the-job training when alignment could be accomplished only by the student becoming a DIS worker and when we considered a course or practicum to be insufficient to achieve alignment.
Results
The health education and promotion BSPH core curriculum contained content that were aligned with 75% (42/56) of all job tasks in the 9 task domains and with 100% of the tasks within domains 2 (investigation activities), 4 (surveillance activities), 8 (case analysis), and 9 (outbreak response and emergency preparedness) (Table 3). The MPH core curriculum contained content or objectives that were aligned with 55% (31/56) of all job tasks and with 100% of the job tasks within domain 9. None of the course content in either curriculum aligned with the job tasks in domain 6 (clinical support services).
Alignmenta of 56 job tasks and 103 knowledge competenciesb for disease intervention specialists (DISs) with BSPHc and MPHd core curriculum course content at the Georgia Southern University Jiann-Ping Hsu College of Public Health
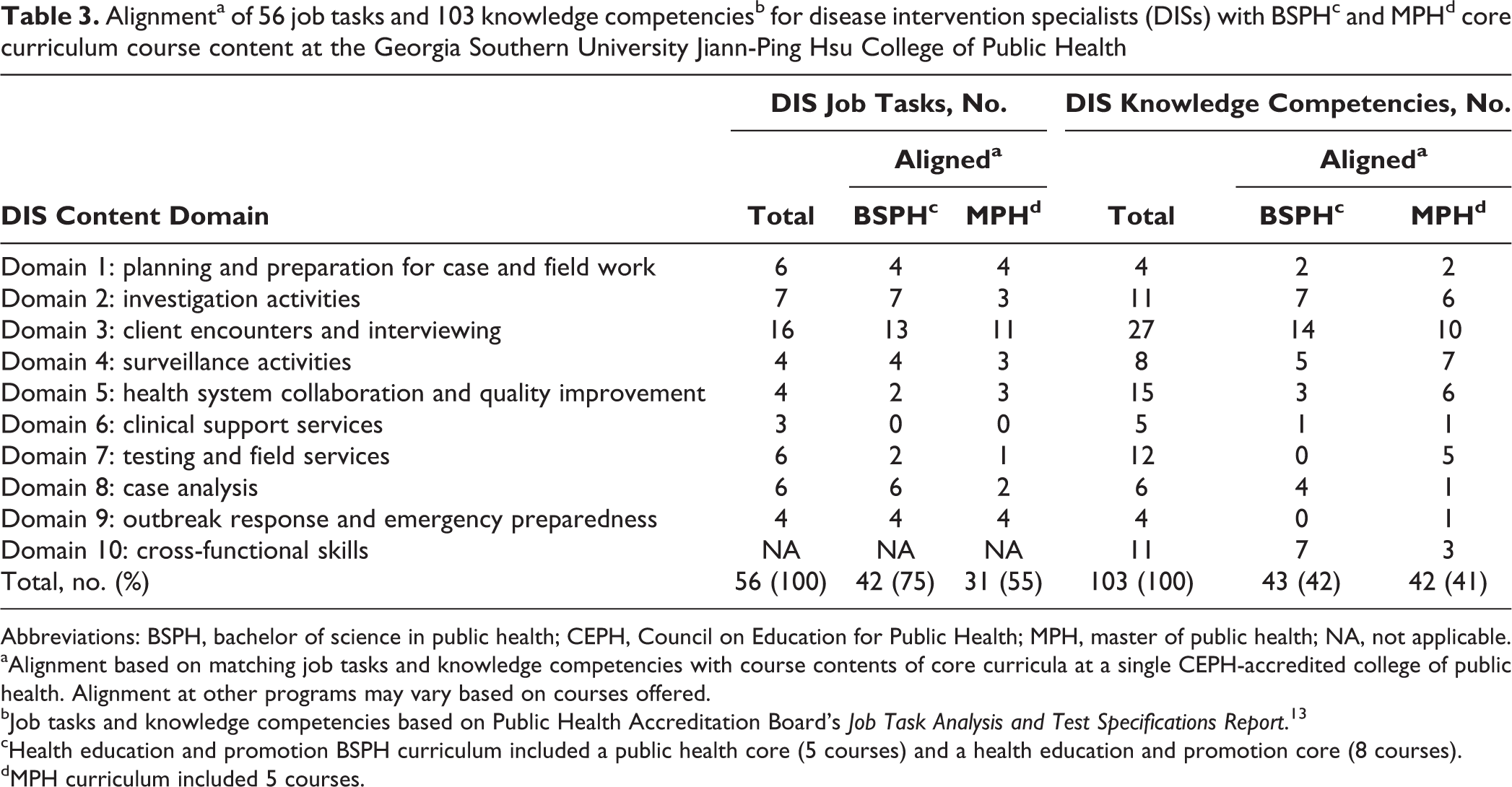
Abbreviations: BSPH, bachelor of science in public health; CEPH, Council on Education for Public Health; MPH, master of public health; NA, not applicable.
aAlignment based on matching job tasks and knowledge competencies with course contents of core curricula at a single CEPH-accredited college of public health. Alignment at other programs may vary based on courses offered.
bJob tasks and knowledge competencies based on Public Health Accreditation Board’s Job Task Analysis and Test Specifications Report. 13
cHealth education and promotion BSPH curriculum included a public health core (5 courses) and a health education and promotion core (8 courses).
dMPH curriculum included 5 courses.
Similarly, the course content and objectives in the health education and promotion BSPH core curricula were aligned with 43% (43/103) and the MPH core curricula with 41% (42/103) of the knowledge competencies in the 10 knowledge domains (Table 3). The course content in the BSPH core curriculum was not aligned with any of the knowledge competencies in domains 7 (testing and field services) or 9 (outbreak response and emergency preparedness).
Job Task Alignment Gaps
The MPH core curriculum content did not align with 25 job tasks, 16 of which were exclusive to the MPH curriculum (Table 4). The health education and promotion BSPH core curriculum content did not align with 14 job tasks, 4 of which were exclusive to the BSPH curriculum. Both the BSPH and MPH core curricula content did not align with another 10 job tasks. Of these 10 tasks, 7 were unique to work done by DISs. Highlights of the recommendations for addressing the gaps in job task alignment included the following:
Disease intervention specialist job tasksa not aligningb with core curriculum course contents of BSPHc and MPHd programs at a CEPH-accredited college of public health
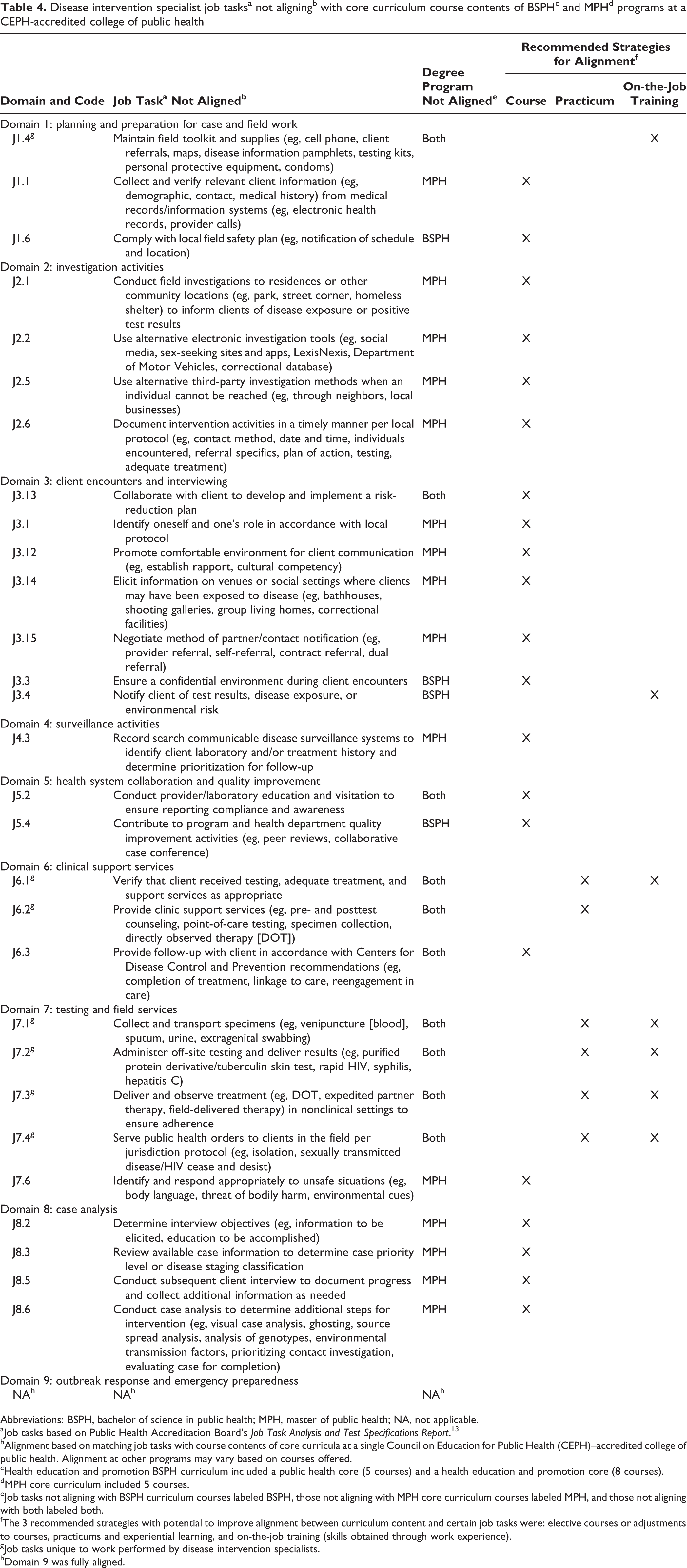
Abbreviations: BSPH, bachelor of science in public health; MPH, master of public health; NA, not applicable.
aJob tasks based on Public Health Accreditation Board’s Job Task Analysis and Test Specifications Report. 13
bAlignment based on matching job tasks with course contents of core curricula at a single Council on Education for Public Health (CEPH)–accredited college of public health. Alignment at other programs may vary based on courses offered.
cHealth education and promotion BSPH curriculum included a public health core (5 courses) and a health education and promotion core (8 courses).
dMPH core curriculum included 5 courses.
eJob tasks not aligning with BSPH curriculum courses labeled BSPH, those not aligning with MPH core curriculum courses labeled MPH, and those not aligning with both labeled both.
fThe 3 recommended strategies with potential to improve alignment between curriculum content and certain job tasks were: elective courses or adjustments to courses, practicums and experiential learning, and on-the-job training (skills obtained through work experience).
gJob tasks unique to work performed by disease intervention specialists.
hDomain 9 was fully aligned.
Elective courses or course adjustments could align the MPH curriculum with 18 additional job tasks and the BSPH curriculum with 6 additional job tasks.
Practicums (or experiential learning) could align the BSPH and MPH curricula with job task J6.2 (providing clinic support services).
Tailored practicums specific to student desire to train as a DIS, or on-the-job training as a DIS, could align the BSPH or MPH curricula with 8 job tasks unique to DIS work.
Knowledge Competency Alignment Gaps
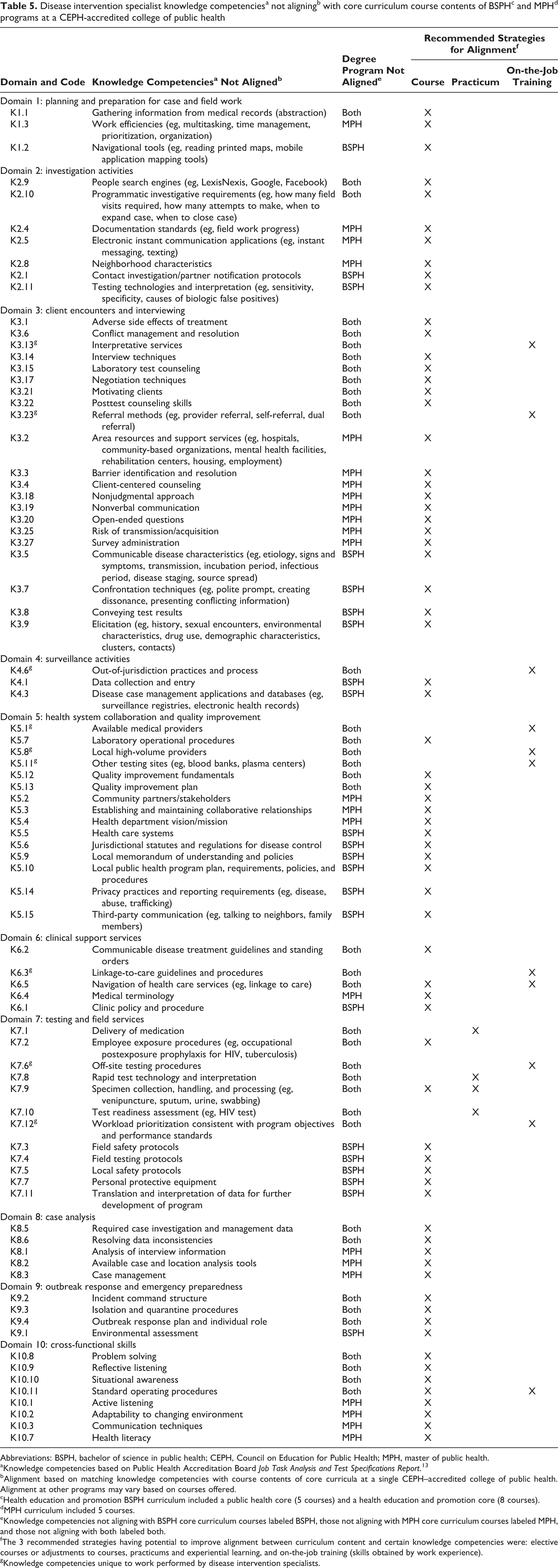
The MPH core and BSPH health education and promotion core curricula content had similar proportions of alignment with knowledge competencies (Table 5). The MPH curriculum did not align with 61 knowledge competencies, 23 of which were exclusive to the MPH curriculum. The BSPH curriculum content did not align with 60 knowledge competencies, 22 of which were exclusive to the BSPH curriculum. Both the BSPH and MPH core curricula content did not align with another 38 knowledge competencies. Of these, 9 were unique to work performed by DISs. Highlights of the recommendations for addressing the gaps in knowledge competency alignment included the following:
Disease intervention specialist knowledge competenciesa not aligningb with core curriculum course contents of BSPHc and MPHd programs at a CEPH-accredited college of public health
Abbreviations: BSPH, bachelor of science in public health; CEPH, Council on Education for Public Health; MPH, master of public health.
aKnowledge competencies based on Public Health Accreditation Board Job Task Analysis and Test Specifications Report. 13
bAlignment based on matching knowledge competencies with course contents of core curricula at a single CEPH–accredited college of public health. Alignment at other programs may vary based on courses offered.
cHealth education and promotion BSPH curriculum included a public health core (5 courses) and a health education and promotion core (8 courses).
dMPH curriculum included 5 courses.
eKnowledge competencies not aligning with BSPH core curriculum courses labeled BSPH, those not aligning with MPH core curriculum courses labeled MPH, and those not aligning with both labeled both.
fThe 3 recommended strategies having potential to improve alignment between curriculum content and certain knowledge competencies were: elective courses or adjustments to courses, practicums and experiential learning, and on-the-job training (skills obtained by work experience).
gKnowledge competencies unique to work performed by disease intervention specialists.
Elective courses or course adjustments could align the MPH curriculum with 49 additional knowledge competencies and the BSPH curriculum with 48 additional knowledge competencies.
Practicums could align both the MPH and BSPH curricula with 3 additional knowledge competencies: K7.1 (delivery of medication), K7.8 (rapid test technology and interpretation), and K7.10 (test readiness assessment).
Either elective courses or practicums could align both the MPH and BSPH curricula with knowledge competency K7.9 (specimen collection, handling, and processing).
On-the-job training as a DIS could align the BSPH or MPH curricula with the 9 knowledge competencies unique to DIS work.
Elective courses, practicums, or on-the-job training could improve alignment of the BSPH and MPH curricula with knowledge competencies K6.5 (navigation of health services), K7.9 (specimen collection, handling, and processing), and K10.11 (standard operating procedures). Whereas elective courses would be most likely to improve knowledge competency related to these items, practicums or on-the-job training would be more likely to improve actual skills.
Discussion
Our findings suggest a considerable degree of alignment between existing CEPH-affiliated public health educational core curricula and the job tasks and knowledge competencies required for robust DIS workforce training. However, our gap analysis also identified job tasks and knowledge competencies that need to be addressed in DIS workforce training but were not covered by the courses composing both the BSPH and the MPH core curricula. These gaps in DIS training represent potentially actionable information that may guide future public health education and training strategy and policy.
To begin with, public health academic administrators need to increase awareness within their programs of the importance of skills and knowledge specific to DIS job performance and how these might be more effectively incorporated into their training programs. This awareness should also be promoted at the affiliated public health credentialing, governing, and organizational levels. The CEPH might seek to develop an optional accreditation module for programs of public health wishing to meet a curriculum standard whereby graduates can become DIS-certified. The development of standardized nondegree certificate programs for DISs could also be offered by academic training programs. A standardized DIS curriculum model that provides a sample scope and sequence of courses and that can be replicated across public health training programs nationwide would be particularly beneficial. This curriculum should be clearly defined by a comprehensive set of evidence-based DIS workforce-specific learning objectives. It should use a clearly defined learner assessment approach, in which practice-based exercises and/or assignments would be integrated within learning environments, and assessment and evaluation strategies would include continuous quality improvement feedback cycles and be linked to the articulated competencies and learning objectives. Finally, this curriculum should be offered asynchronously or through appropriate distance-learning modalities, to maximize its reach to the intended workforce audience.
A potential barrier to meaningful change in the area of DIS training exists within the public health practice community. The general public health workforce is already stretched thin, as members seek to meet the 3 core functions of public health (assessment, policy development, and assurance). 18 Furthermore, as noted in the Public Health Accreditation Board’s Job Task Analysis Report, a substantial proportion of the current DIS workforce does not hold even a bachelor’s degree in public health. 8 Because of these potential barriers, the goal of meeting DIS workforce needs might be aided by promoting DIS-specific competencies through certificate or practice-based training programs. 19 Hence, a multidimensional approach will be necessary, providing DIS workforce training and professional development to current public health workers, while at the same time seeking to infuse DIS-specific curricula into the nation’s academic public health training programs.
Another challenge to bringing about change in DIS workforce development involves the difficulty of both identifying and operationalizing strategies that are likely to facilitate the desired change. 20,21 Our findings suggest ways in which DIS workforce quality can be improved in academic public health training programs. Indeed, accredited academic public health programs are well positioned to serve the educational needs of students at the bachelor and master levels. These programs regularly evaluate and assess their curricula, and as a result, new training activities and curricula are being introduced. 22 In addition, key national professional organizations, including the Centers for Disease Control and Prevention, the Public Health Accreditation Board, the National Association of County and City Health Officials, and the National Coalition of STD Directors, are investing resources in evaluating and promoting the development of the DIS workforce. 23 Local public health departments are also central to developing and engaging the DIS workforce, because this represents the workforce intersection with the community.
Ultimately, however, it is up to the public health practice community to implement changes in practice. Intentional, effective, and complete engagement by the practice community is necessary to strengthen the nation’s DIS workforce. Local health departments have a substantial DIS workforce already in place, with more than 2060 DISs nationwide. Efforts to reach out to local health department leaders with regard to DIS workforce development initiatives will be essential in promoting the uptake of DIS workforce standardization and quality improvement. The academic public health community will be unable to bring about the needed changes without the full support of those working on the front lines in local health departments. Strengthening the DIS workforce is more likely to be possible and sustainable with a public health practice–based commitment toward DIS workforce development.
Limitations
This gap analysis had several limitations. First, our findings were based on programs at 1 CEPH-accredited college of public health and, as such, may not be generalizable to all public health academic programs in the United States. The extent to which DIS-related job tasks and knowledge competencies were explored within individual academic public health programs may vary. Whereas some programs may offer courses that provide in-depth focus on the skills and knowledge directly related to DIS job performance, other programs may offer only a cursory examination of these items and provide a broad overview of the concepts, skills, and competencies needed in public health practice.
Conclusions
DISs currently arrive in their roles in public health practice from various educational and experiential backgrounds. Our findings suggest that BSPH and MPH core curricula at formal public health academic programs may not be fully aligned with the job skills and knowledge competencies needed by DISs to function at their full potential. Investigation into the alignment of job skills and knowledge competencies with core courses at other schools and programs of public health is warranted. Strategic core course adjustments or additions of elective courses, based on gap analyses, may be one way programs can improve alignment and provide a more solid educational foundation for the DIS workforce.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding to support this research was provided by the Public Health Accreditation Board (PHAB) under the authority of the Georgia Southern University Research & Service Foundation, Inc. The DIS Certification Project was supported through funding from the Centers for Disease Control and Prevention (CDC) through Cooperative Agreement CDC-RFA-OT13-130104CONT16. Contributing authors from Georgia Southern University were provided summer salary support for the conduct of this research. In addition, Kaye Bender, who contributed to the writing of this article, issued and approved the contractual agreement to support this commissioned research. This original research was supported by the foundational work of PSI Services, LLC, through a collaborative agreement between the PHAB, the National Association of County and City Health Officials, the National Coalition of STD Directors, and CDC.