
Abstract

Some of the nation’s greatest public health successes would not have been possible without policy change. The Centers for Disease Control and Prevention’s list of “Ten Great Public Health Achievements”—including motor vehicle safety, tobacco control, and maternal and infant health—all involved policy change. 1 Because of these public health achievements, the average life expectancy at birth for people living in the United States increased by more than 30 years, from 47.3 years in 1900 to 76.8 years in 2000. 2 The age-adjusted death rate in the United States continued to increase to 78.8 years in 2014. However, it decreased to 78.7 years in 2015 and then to 78.6 years in 2016. 2 This emerging trend is the result of numerous public health challenges, especially the opioid and obesity epidemics, which continue to burden society.
In this Commentary, we make the case for the central role of policy in mitigating America’s public health challenges. We first define policy, then propose principles that are essential for policy change and are based on the authors’ collective experiences, and conclude with implications for local health departments, academics, and the next generation of public health leaders.
Defining Policy
The term “policy” refers to a standard set of principles that guide a course of action. 3 -5 Public policies are established by the government, whereas private or institutional policies are created by organizations for institutional use. Many public policies are legally binding, meaning that individuals and institutions in the public and private sectors must comply with them. In contrast, policies created by private institutions do not carry the force of law; however, within an institution, compliance with such policies may be required (Table 1).
Examples of policy types, by government level of enactment and category
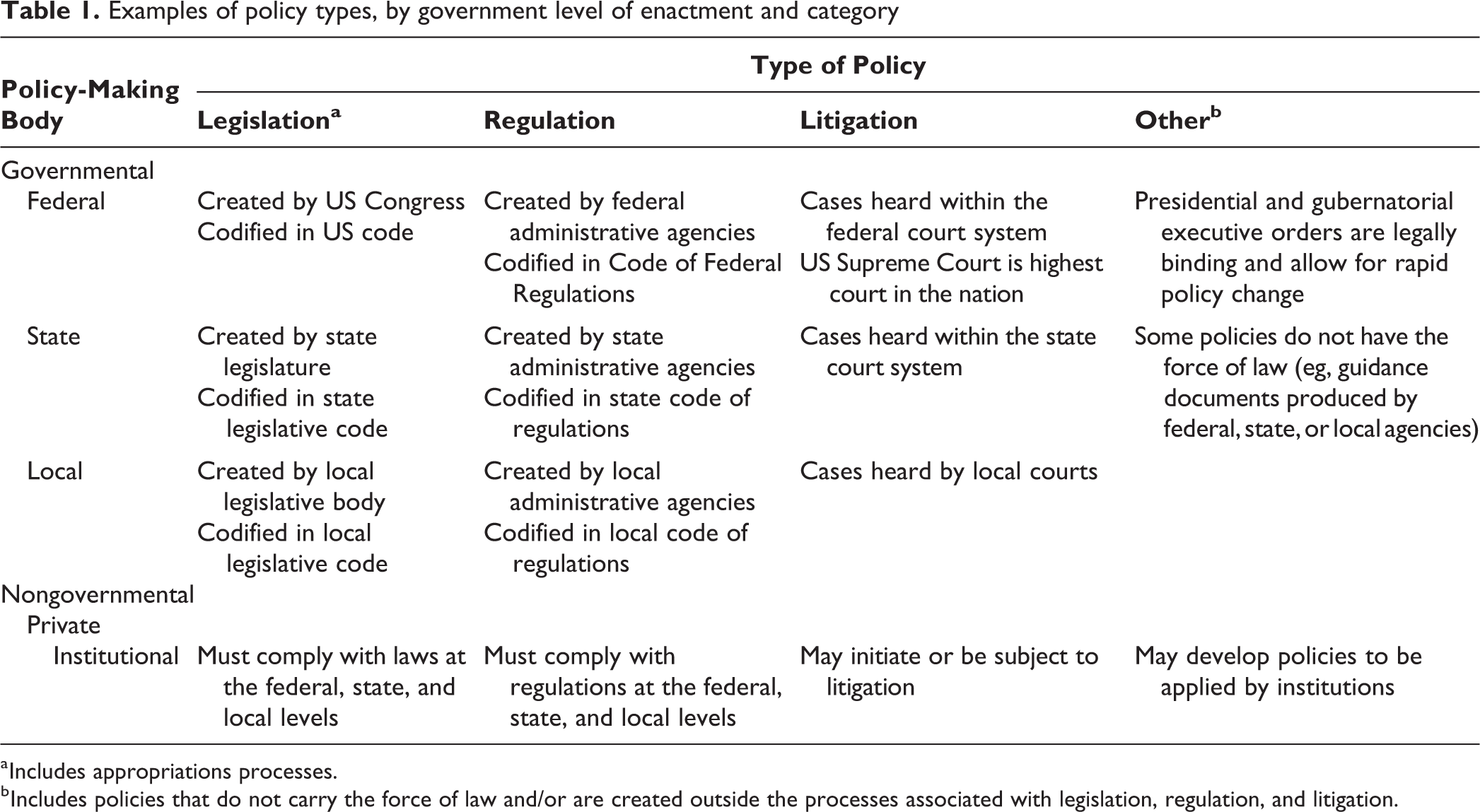
a Includes appropriations processes.
b Includes policies that do not carry the force of law and/or are created outside the processes associated with legislation, regulation, and litigation.
In the United States, public policies may be enacted by federal, state, or local governments. Typically, public policies created by a lower level of government (eg, local) must comport with policies created by a higher level of government (eg, state). In addition, in some instances, a higher level of government (eg, federal) may preempt, or prevent, a lower level of government (eg, state) from enacting policies in a particular area. 6 This process, known as “ceiling preemption,” may stifle policy innovation, particularly at the local level.
Legally binding public policies fall into 3 primary categories: legislation, regulation, and litigation. Legislation, or statutory law, is created by a legislative body comprising elected representatives (eg, from US Congress, state general assembly, or city council). Regulations, which are promulgated by federal, state, or local administrative agencies, typically add specificity to policies that are described broadly in legislation. Finally, litigation refers to the body of public policy created through judicial opinions. Other policy tools, such as presidential or gubernatorial executive orders, are legally binding and bypass traditional legislative or regulatory processes, allowing for more rapid policy change.
Of note, some public policies do not carry the force of law. Most often, these policies are guidance documents produced by administrative agencies. Although guidance cannot be enforced, the expectation is that it will be followed or will provide answers when the law is unclear.
Principles for Effective Public Health Policy Change
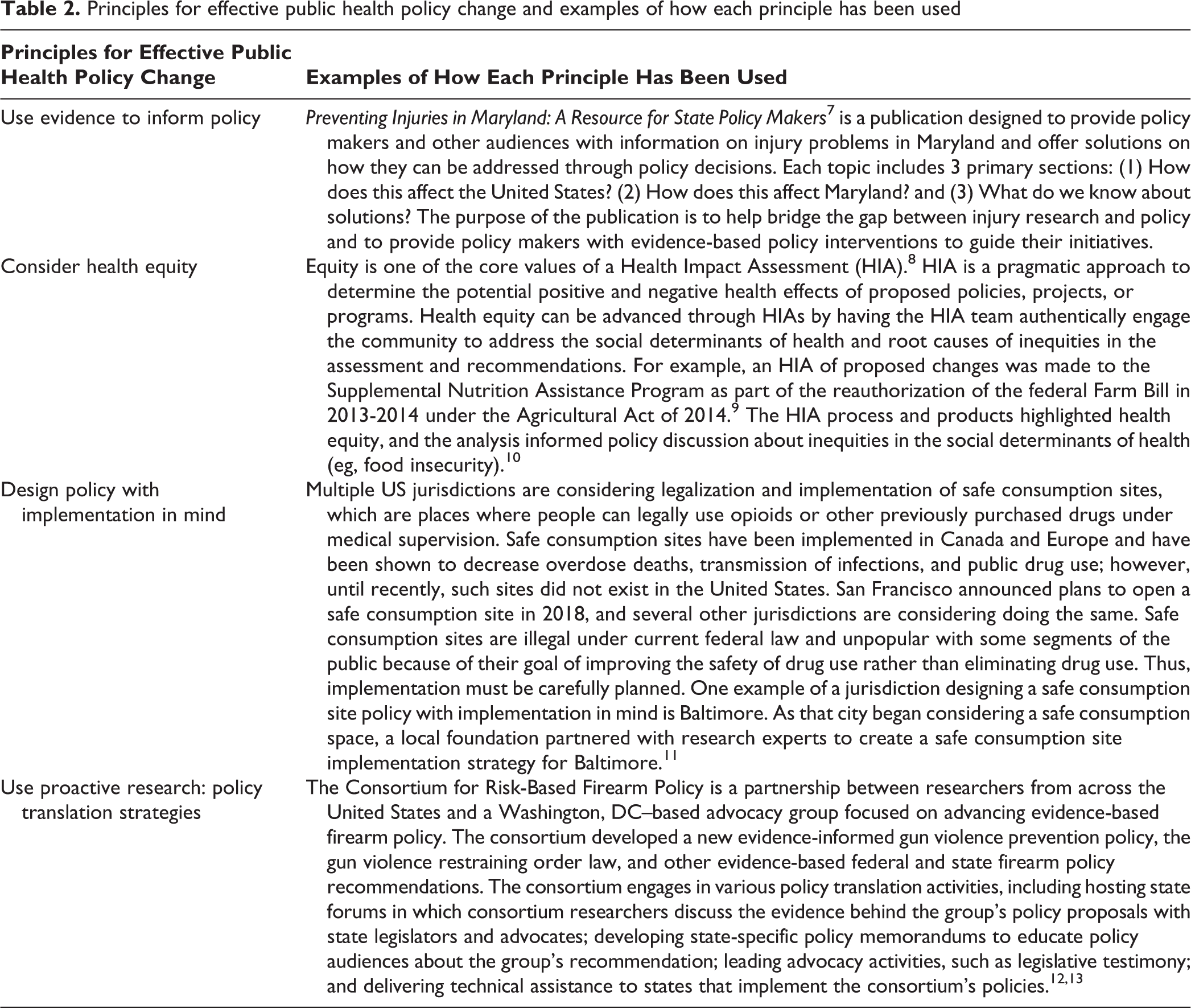
Effective policy change is more likely to improve health when key principles are considered. We outline 4 principles that we believe bolster effective public health policy change. We define public health policy as laws, regulations, plans, and actions that are undertaken to achieve public health goals in a society. These principles are based on the authors' collective public health policy experiences and are grounded in the policy sciences literature. These principles are listed, along with references and examples of experiences that informed them, in Table 2.
Principles for effective public health policy change and examples of how each principle has been used
1. Use Evidence to Inform Policy
Although policy formation is a complex process involving multiple factors, including feasibility considerations, stakeholder interests, and political values, 3 sound research evidence should serve as the public health community’s starting point when it designs and advocates for public health policy solutions. Policy design should be based on the best available research evidence, with an understanding that the strength of that evidence may vary across public health issues and change over time. 14 For emerging public health problems, research evidence in support of policy solutions may be limited. In these scenarios, research on related policy mechanisms from other fields or in nations outside the United States may help inform policy development. 15 All policies, but especially new policies, little-studied policies, or evidence-based policies that are tailored to meet the needs of various subpopulations, should include mechanisms for monitoring and evaluation to determine the policy’s effectiveness. 16,17 Evaluation results can be used to refine implementation and support policy scale-up in additional jurisdictions.
Numerous evidence-based policies address public health problems. For example, “The Community Guide” is a collection of evidence-based findings from the Community Preventive Services Task Force and is one source of information for these evidence-based policies. 18 With consistent implementation, these known evidence-based policies can lead to dramatic short-term and long-term improvements in public health.
2. Consider Health Equity
Health equity refers to every person having an opportunity to attain his or her highest level of health. 19 In formulating policy, considering health equity means “optimizing the conditions in which people are born, grow, live, work, learn, and age; working with other sectors to address the factors that influence health; and naming racism as a force in determining how these social determinants are distributed.” 20 For example, data support the important role that residential segregation of black and white people, because of racist housing policies, has played in health disparities by race in the United States, leading to higher rates of child poverty and adverse birth outcomes among black children than among white children. 21
Policies that address and dismantle these underlying political, economic, social, and physical determinants of health can advance health equity. 22 For example, when land development changes are proposed, planners and policy makers should consider how these changes may lead to gentrification and displacement of historically marginalized populations, which have implications for their health. 23 By considering health equity, questions such as how a policy will increase or decrease access and opportunity for communities of color, in addition to how a policy may lead to other unintended consequences, can also be raised. Equity considerations can also be included during policy implementation, evaluation, and monitoring, to ensure that equity is promoted through indicators that can document progress toward health equity–related goals (eg, percentage of policies that address the social determinants of health). 24
3. Design Policy With Implementation in Mind
Policy should be designed with implementation in mind. Too often, enactment of a new policy (eg, when a bill is signed into law) is seen as the end of the policy process. 25 Instead, it is only the beginning. Implementation determines the policy’s success or failure. Policies that include clear, concrete definitions of the target population and detailed regulations are more likely to be successfully implemented than policies that leave such criteria subject to interpretation. 26,27 For example, to be effectively implemented, a state law prohibiting the sale of sugar-sweetened beverages in schools should define which types of schools are subject to the law, criteria for defining a sugar-sweetened beverage, the date by which schools must comply with the law, and the sanctions that will be imposed on schools that do not comply with the law. These types of details are typically developed during the regulatory process, after enactment of federal, state, and local laws.
Implementation should be considered from the beginning of the policy design process. People who design policy should contemplate factors such as whether a new or existing agency will implement and enforce the policy, whether new personnel will need to be hired and/or whether existing personnel will need to be trained, and whether administrative changes (eg, creation of new eligibility forms or electronic monitoring systems) are needed. 28 -30 Policies that make minor changes to existing policies are simpler and quicker to implement than policies that make major changes to the status quo, and those designing public health policies should plan accordingly, in terms of both resource allocation and timing. 27,29 Full implementation of policies that enact new programs, for example, will take substantially longer than full implementation of policies that change only eligibility criteria for, or categories of, services covered by existing policies.
4. Use Proactive Research-Policy Translation Strategies
To increase translation of research into policy, proactive strategies that bridge the research and policy worlds to increase adoption and implementation of policies shown to be effective in research studies are needed. 16,31 Researchers and policy makers have unique skill sets and professional incentives. For example, researchers are skilled in producing research evidence, and the academic promotion process emphasizes peer-reviewed publications of research findings. In contrast, policy makers are skilled in policy development, analysis, political negotiation, and coalition building, and their professional incentives are focused on reelection. 32 -34 In addition, researchers have deep expertise in a narrowly defined field of study, whereas policy makers have working knowledge across an array of topics. Furthermore, although research can be slow, the policy process often moves quickly, with short windows of opportunity for new policies to be developed and enacted. For example, some state legislative sessions are as short as 30 days per year. 35 To advance evidence-based public health policy, research-policy translation models must bridge these differences. These models should include training for researchers about how to ask policy-relevant research questions, the steps of policy process, the politics of the policy process, and how to engage with policy makers. 16,36 -38
To substantially increase translation of evidence into policy, however, research-policy translation initiatives must go beyond these activities to include long-term coalition building and formal partnerships between key research and policy stakeholders (eg, academic–public health department partnerships 39,40 and national coalitions focused on advancing evidence-based policy). 41 An example of the coalition model of research-policy translation is the Consortium for Risk-Based Firearm Policy, a partnership between researchers from across the United States and an advocacy group based in Washington, DC, that focuses on advancing evidence-based firearm policy. 42 Since its formation in 2013, the consortium has developed an evidence-informed gun violence prevention policy, created a gun violence restraining order law, and conducted a range of activities—including hosting forums in which consortium researchers discuss the evidence with state legislators and advocates 42,43 —that contributed to the law’s passage in 8 states. 44
These types of formal research-policy translation models can address multiple barriers to enactment and implementation of evidence-based policy. Engagement of broad coalitions can help increase stakeholders’ recognition of the value of policy change and facilitate partnerships between advocates and policy makers adept in formulating political strategy. In addition, these types of models can help to identify gaps in the evidence base of public health policy issues and, by strengthening partnerships between researchers and policy makers, inform the development of policy-relevant research to fill those gaps.
Implications for Public Health
Various actors play important roles in applying these principles to the design and implementation of evidence-based public health policy. Public health departments are responsible for numerous local and state public health policies. For these public health professionals, applying these principles involves engaging with stakeholders from other sectors (eg, transportation and planning) in other salient government agencies to promote strong cross-sector partnerships. Decisions made in sectors outside of public health and health care, such as education, transportation, and criminal justice, strongly influence health and well-being. 45 Thus, efforts to improve public health through policy change must involve decision makers and stakeholders from these other sectors. In the United States, more communities than before are adopting multisector approaches, and local and state health departments are initiating much of this activity. 46 Tools such as Health Impact Assessments (HIAs) are being used to identify potential public health effects of decisions proposed by other sectors (Table 2). An HIA is a practical approach to determine the potential, and often overlooked, health effects of proposed policies, projects, or programs from nonhealth sectors, as well as provide practical recommendations to minimize risks and improve health. 47 Involving these other sectors in decisions that influence the determinants of health can also address underlying inequities and present an opportunity for health departments to consider health equity. 8
For academic practitioners, advancing policy change requires that academics not only generate policy-relevant research, but also translate and disseminate findings to practitioners, advocates, and policy makers. Having open communication channels between academics and public health practitioners provides opportunities for practitioners to share the types of data that are useful for policy debates and advocacy efforts, and it helps ensure that academics are asking the right questions needed to generate policy-relevant results. Some faculty are reluctant to engage in these translational and policy engagement activities because these activities are often not evaluated as part of their promotion process. Having institutional supports that recognize policy engagement and translational activities as part of scholarship and consider these activities during the faculty promotion process could bolster faculty participation in policy change activities. 48
Academics also have the important role of training future public health leaders to amplify public health policy change. Policy development is one of the core functions of public health 49 ; however, public health professionals have cited policy development as one of the areas in which training is needed. 50 Future leaders need to be trained in policy sciences, including policy analysis, communication, implementation, evaluation, and translational research, along with the politics of the policy process. In addition to these policy competencies, training in health equity and research translation will further prepare future leaders to engage in effective public health policy change.
Policy change can help address current and future public health issues in the United States. The 4 principles we outlined should undergird all policy efforts to optimize their impact.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following funding with respect to the research, authorship, and/or publication of this article: This article was produced with the support of the Bloomberg American Health Initiative, which is funded by a grant from the Bloomberg Philanthropies.