
Abstract
A growing body of literature uses the concept of core components to better understand small-scale programmatic interventions. Instead of interventions being viewed as unitary “black boxes,” interventions are viewed as configurations of core components, which are the parts of interventions that carry their causal potential and therefore need to be reproduced with fidelity to produce the intended effect. To date, the concept of core components has not been as widely applied to public health policy interventions as it has to programmatic interventions. The purpose of this topical review is to familiarize public health practitioners and policy makers with the concept of core components as applied to public health policy interventions. Raising the profile of core component thinking can foster mindful adaptation and implementation of public health policy interventions while encouraging further research to enhance the supporting evidence base. We present 3 types of multilevel interactions in which the core components of a public health policy intervention produce effects at the population level by (1) seeking to directly affect individual behavior, (2) facilitating adoption of programmatic interventions by intermediaries, and (3) encouraging intermediaries to take action that can shape changes in upstream drivers of population health. Changing the unit of analysis from whole policies to core components can provide a basis for understanding how policies work and for facilitating novel evidence-generating strategies and rapid evidence reviews that can inform future adaptation efforts.
Public health policy interventions may be distinguished from programmatic interventions by their broad reach, attention to upstream drivers, and reliance on the regulatory and administrative powers of the state, all of which seek to affect systematic changes or shape contexts in ways that make healthy decisions the “default.” 1 Public health policy interventions afford public health practitioners and decision makers considerable opportunities to improve the health of their communities because such interventions generally “require less individual effort and have the greatest population impact.” 1 History is replete with examples of public health policies, such as those related to water and sanitation infrastructure, as important contributors to the impressive increase in life expectancy and productivity during the 20th century.2-7 To reap the potential effects of public health policy interventions, it is important that the interventions be based on or informed by evidence. 8 The Institute of Medicine, now the National Academy of Medicine, and others have identified evidence-based policy development, along with assessment and assurance, as an essential component of public health practice.9,10
Yet, current gold standard research and evaluation approaches (eg, randomized controlled trials, quasi-experiments) are not always well suited to the often multicomponent nature (ie, involving combinations of interventions) and multilevel nature (eg, working simultaneously at the individual, household, community, and national levels) of public health policy interventions. 11 As observed by Brownson et al, in policy “we seldom have a single ‘intervention,’ but rather a ‘blending of several interventions.’” 12 Not surprising, in public health policy, the supply of gold standard studies on population-level interventions is small relative to the number of such studies on programmatic interventions. 13
The scarcity of evidence creates a dilemma for evidence-minded policy makers. On one hand, policy makers could wait for evidence about a policy intervention to accumulate; however, waiting for evidence risks missing a policy window to address a serious health condition.14,15 On the other hand, policy makers could adapt evidence about policy interventions that share some but not all of a favored policy’s characteristics. Yet, studies typically offer little guidance about which aspects of policy interventions are necessary—and therefore must be implemented with high fidelity—as opposed to those aspects that can be adapted to fit the context. Because of these limitations and to make evidence more functional for practical application, we, with a growing number of authors, suggest shifting the unit of analysis from whole policies to the core components of which they consist.6,15-18 Identifying the core components of policy interventions could promote evidence-based policy making, akin to how defining programmatic core components has facilitated evidence-based program development.6,12,15-18
Programmatic core components are “the parts, features, attributes, or characteristics of a program that a range of research techniques show influence its success when implemented effectively,” 19 show reliable effects across contexts, and need to be reproduced with some degree of fidelity to produce the intended effect.19 -21 Programmatic core components provide a set of evidence-based “priors,” thus reducing the need to start de novo in developing and evaluating each new public health programmatic intervention. Existing work on core components has mostly focused on changing individual behavior, and little of the literature has addressed what is needed to promote large-scale effects. 18 Furthermore, authors use different terminology to describe the same—or similar—concepts.
The purpose of this topical review is to familiarize public health practitioners and policy makers with the concept of core components as applied to public health policy interventions. Raising the profile of “core component thinking” can foster mindful adaptation and implementation of public health policy interventions while encouraging further research to enhance the supporting evidence base. First, using key terms related to core components (Table), we review how core components work. We next describe how core component concepts can be applied to multilevel policy interventions, and we provide illustrations based on 3 types of interactions. We conclude by discussing implications for public health policy practice and research.
Key terms related to core components of evidence-based public health policy a
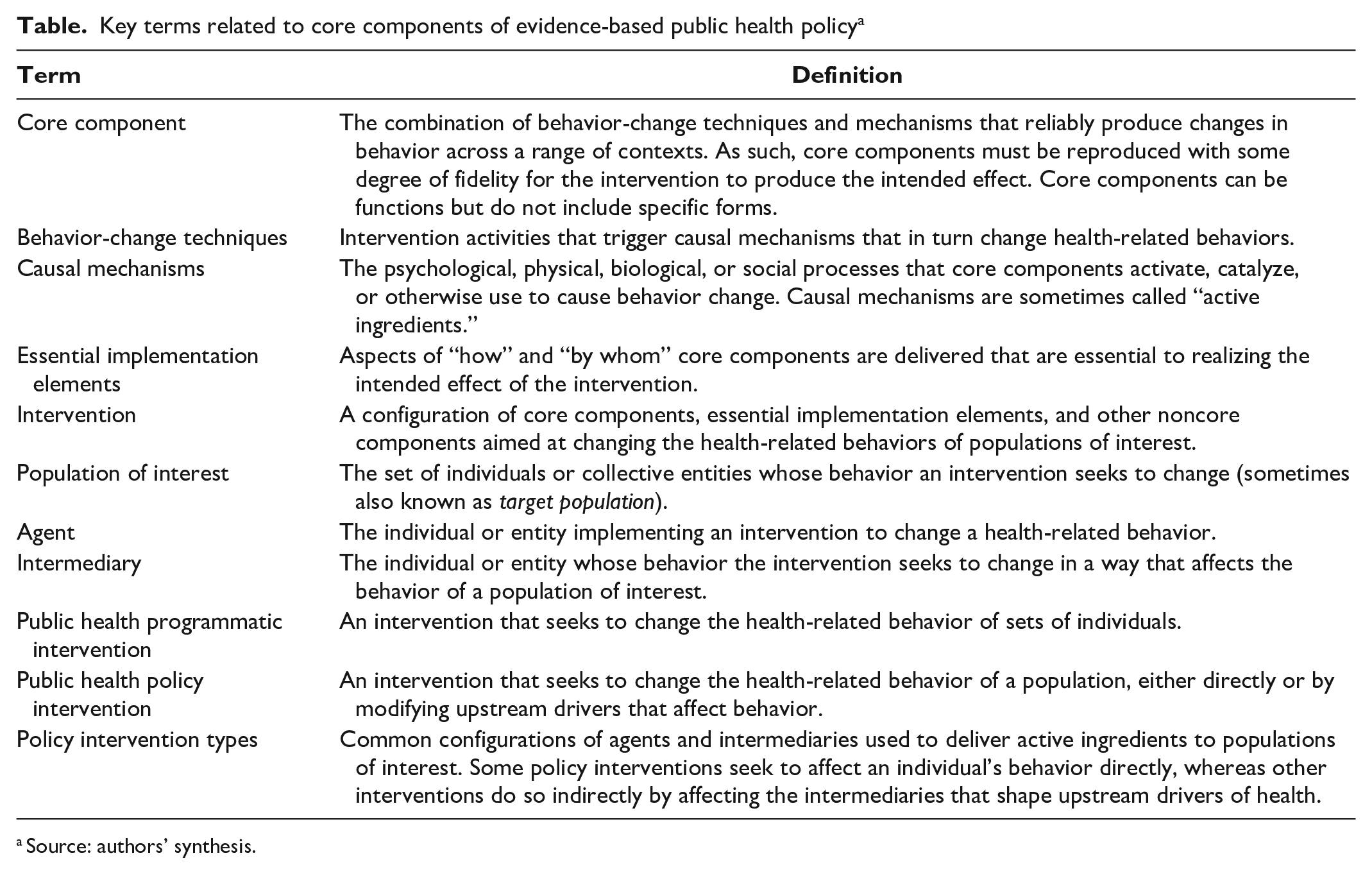
Source: authors’ synthesis.
This activity was reviewed by the Centers for Disease Control and Prevention and was conducted consistent with applicable federal law and institutional policy (see eg, 45 CFR part 46; 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq). Human participant protection was not required because this work did not involve human participants.
How Core Components Work
Core components of effective public health programmatic and policy interventions are those fundamental pieces that induce what works in the intervention to realize the expected outcome. 19 Connell et al provided one of the most systematic accounts of core components. 22 In particular, the authors assembled evidence to describe core components in terms of how behavior-change techniques trigger underlying causal mechanisms that in turn create changes in health-related behavior (Figure 1). Drawing on a literature review and expert elicitation, Connell et al identified 51 behavior-change techniques that can be paired with 20 causal mechanisms. For example, the technique of “goal setting” (ie, the process of identifying and committing to specific behavioral targets) triggers underlying causal mechanisms related to acquiring skills, perceived needs or deficits, social learning, normative beliefs, and others. Similarly, Perez Jolles et al distinguished core functions (“the core purposes of the change process that the health intervention seeks to facilitate”) from core forms (the specific strategies or activities “needed to carry out the core functions”). 23 Fidelity is sought and assessed for core functions but not for core forms, which “may be customized to local contexts.” 23 Although the specific concepts are used meaningfully, the implications are similar to the framing presented previously—that is, that the effectiveness of interventions often lies not in their detailed activities but in more general attributes (whether described as functions or as pairings of causal mechanisms and behavior-change techniques). Given the distinctions between general attributes and detailed activities, evidence-building and evaluation efforts that distinguish the two likely would yield more informative results.
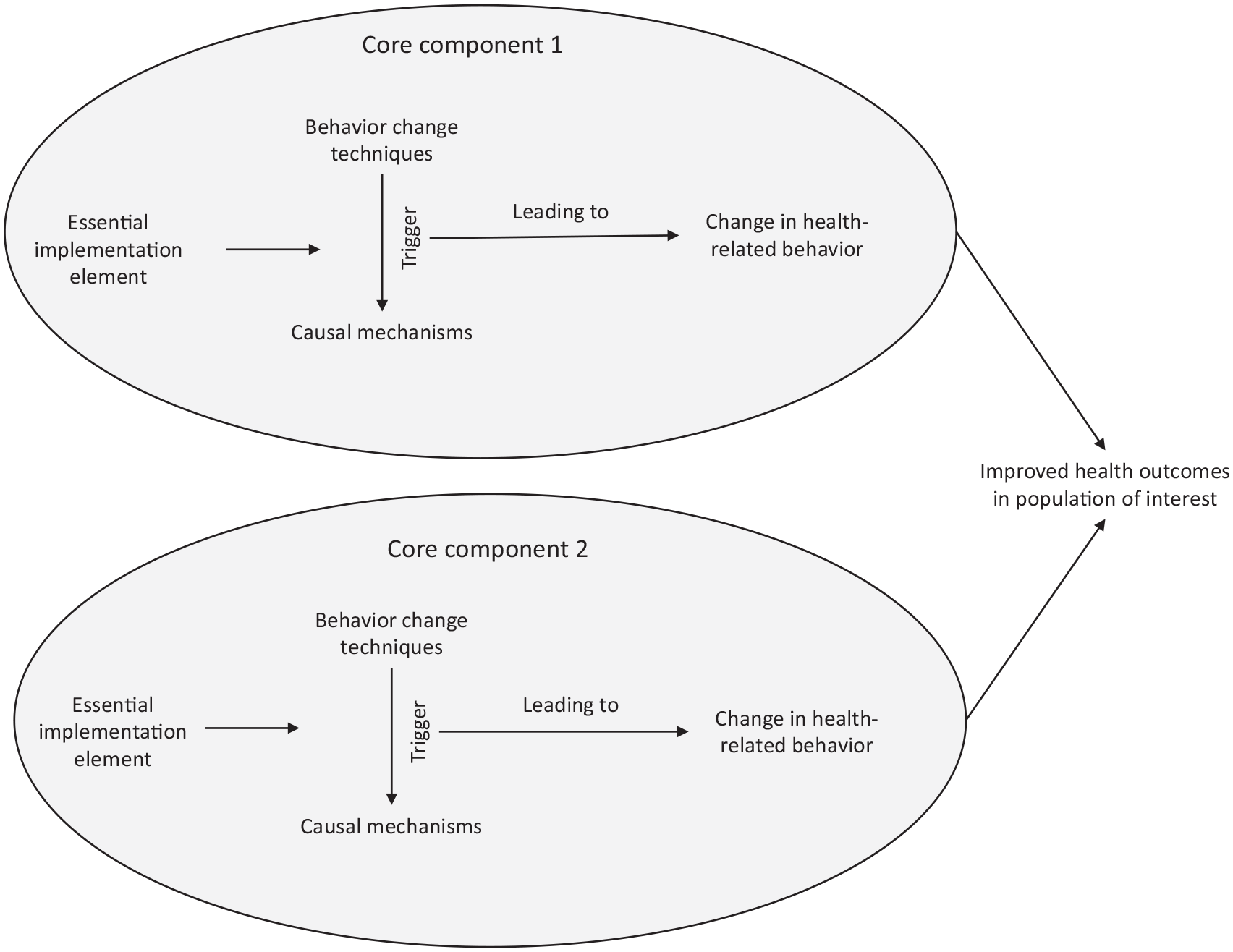
Inner workings of core components. Core components comprise behavior-change techniques that trigger causal mechanisms that lead to changes in health-related behaviors. Essential implementation elements can support and enable that pathway. Source: authors’ synthesis.
Core components can include essential implementation elements—that is, requirements about how programmatic or policy interventions are delivered and who delivers them (Figure 1). 17 For example, a public health message about an infectious disease risk might be more effective if delivered in consultation with culturally and linguistically competent community partners rather than by one-size-fits-all language and messaging partners. 24 In addition, interventions can be configurations of multiple core components, each of which pairs triggering activities, mechanisms, and behaviors. 25
How Core Components Can Be Useful
Approaching policy interventions from a core components mindset can have multiple benefits for multiple audiences. For a given situation, intervention designers may select and combine core components (supplemented by noncore components, where necessary). In turn, implementers of public health policy interventions can use core components to distinguish which parts of an intervention need to be implemented with fidelity versus which parts can be adapted to fit a specific context. Finally, evaluators of interventions can use core components to better understand how interventions work. Perkinson et al proposed a “traffic light” framework for understanding how changes to an intervention can affect core components. 6 In this framework, “green light” adaptations are those that support or amplify core components, and “red light” adaptations are those that omit or greatly curtail core components. As Perkinson et al observed, providing culturally relevant examples to illustrate the core messages of a violence prevention program might be a green light adaptation, whereas omitting key message points or adding contradictory message points might be a red light adaptation. “Yellow light” adaptations fall somewhere in between and often require judgment. 6
How Core Components Can Be Applied to Broad-Scale Public Health Policy Interventions
The history of public health suggests that achieving broad-based changes in health-related behavior often requires coordinated action to create conditions that foster healthy choices.1,8 Therefore, implementing programmatic core components in some contexts is a substantial accomplishment, although implementation of programmatic core components alone may not be enough to have a population-level effect. In describing the role of public health nurses, Keller et al noted that interventions that affect health at a population level involve combinations of individual-, community-, and systems-focused practices (ie, “changes [in] organizations, policies, laws, and power structures”). 4 As an example, the authors pointed to efforts to reduce domestic abuse during pregnancy, including media campaigns to change public attitudes and policies designed to institutionalize screening across a range of clinical and social service settings. 4
Effects at the population level therefore often require not only the aggregate, collective efforts of large numbers of people but also actions on the part of those in a position to have an effect on norms and structures. 26 The question is, thus, whether thinking in terms of policy core components can apply to efforts to change the behavior of agents at the meso (institutional) and macro (societal) levels of systems, in addition to the behavior of individuals.
How Interactions of Agents, Intermediaries, and Individuals Can Affect Population-Level Behavior
Schneider and Ingram’s discussion of the concepts of “agents” and “intermediaries” is useful in capturing action at multiple levels of systems. 27 Agents are the institutions and organizations responsible for taking actions that activate or implement the core components of an intervention that is intended to affect the behavior of the population of interest. The agents of public health interventions are often departments of public health. Other governmental agencies have been increasingly recognized as agents of public health interventions by ensuring, for example, clean air and water (eg, departments of environmental protection) and safe spaces in which to exercise and play (eg, public safety, city planning). Agents also include third-party actors in the nonprofit or private sector, such as nonprofit food banks that receive federal funding to provide emergency food assistance to low-income people who are experiencing short-term hunger. 28
An intermediary is an individual or organization that operates as a member of the population of interest for the first part of the intervention and then as an agent. For example, liquor store owners are held liable by legal drinking age policies for selling alcohol to minors, which in turn encourages them to check identification and take other measures to reduce sales to minors.29,30
How Agents, Intermediaries, and Individuals Interact to Create Population-Level Behavior Change
Large variations exist in how policy makers, agents, and intermediaries at numerous levels interact to use core components. We present 3 types of interactions that represent some but not all of this variation; these interaction types can provide a basis for application and for additional research and analysis. The described interactions include situations in which public health policy interventions (1) seek to directly affect individual behavior, (2) facilitate adoption of programmatic interventions by intermediaries, and (3) encourage intermediaries to take actions that result in changes in upstream drivers of population health (Figure 2).
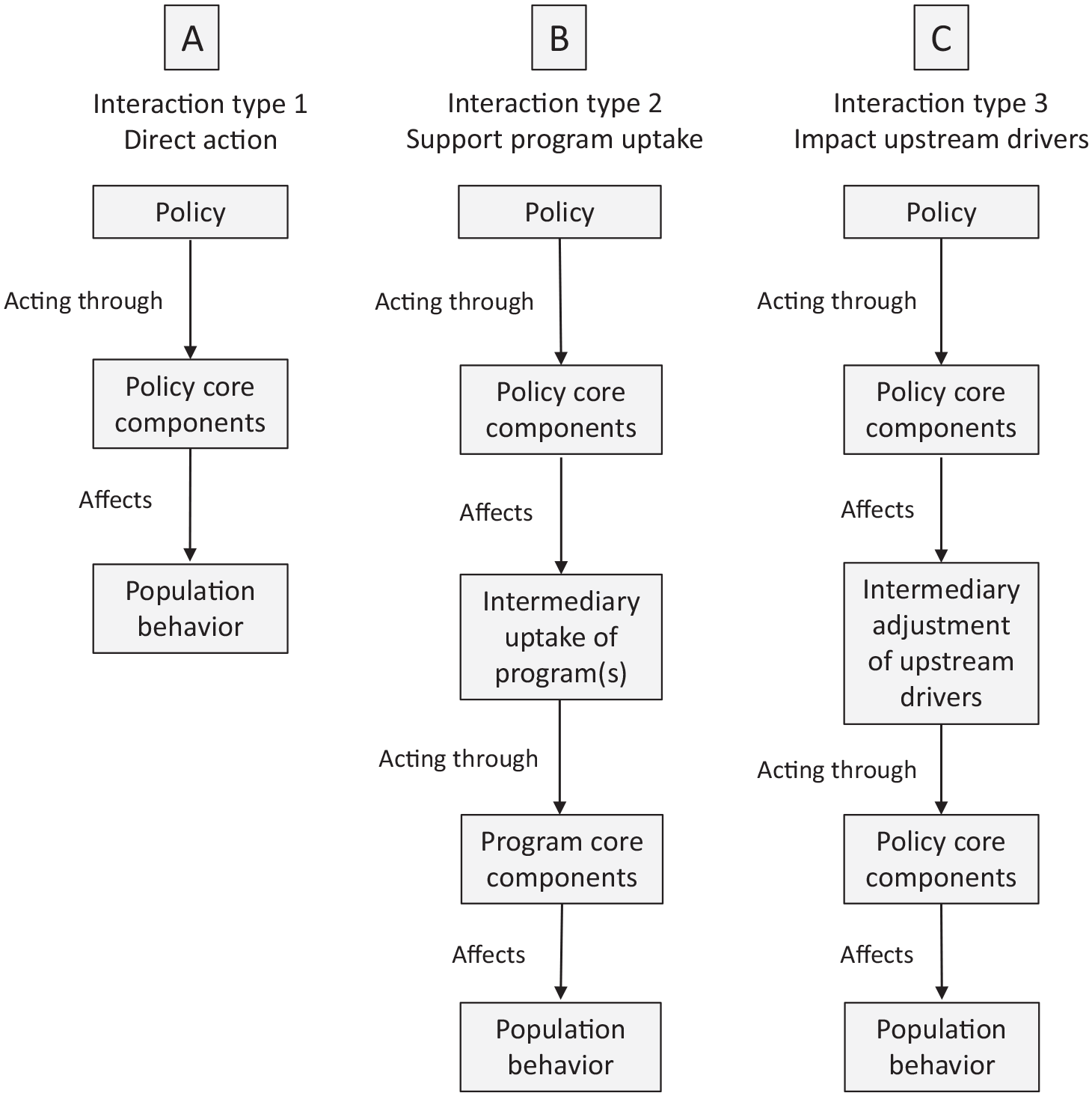
Multilevel nature of a public health policy intervention, showing 3 candidate types. Source: authors’ synthesis.
Type 1: Policy Core Components That Directly Deliver Benefits
Some public health policies involve core components that leverage mechanisms to change individual or household behavior, with little or no role for intermediaries. These policies use core components that differ little from those used by programmatic interventions, except that policy core components use the unique authorities and implementation apparatus of government to ensure broad uptake (Figure 2A).
An example is the Earned Income Tax Credit (EITC), which encourages workforce participation among low-income households. The EITC is also a good illustration of a public health policy intervention that comes from outside traditional public health agencies. The population of interest is working families living below the federal poverty threshold; in general, this population experiences lower life expectancy and higher morbidity than populations living above the federal poverty threshold.2,31
The EITC’s core components use incentives to drive individual and household behavior change, specifically by creating an incentive for people with low income to join the labor force or increase their work hours. This economic incentive is necessary because many low-wage jobs do not cover costs of living, and workers, particularly single mothers, drop out of the workforce. Increased workforce participation in turn leads to increases in lifetime average earnings and Social Security retirement benefits, improvements in educational outcomes, decreases in risky health behavior, and improvements in health outcomes (eg, birth weight, allostatic load, subjective well-being, adverse childhood events) among EITC recipients and their children.32-34
The EITC’s potential for broad impact comes from use of the income tax code and associated administrative and enforcement infrastructure, which reach nearly all adult citizens in a political jurisdiction. Without a tax code or other policy apparatus capable of near-universal reach, it is difficult to imagine how the individual-level core components of the EITC could be implemented at a population level. 34
Type 2: Policy Core Components That Encourage Adoption of Health-Promoting Programmatic Interventions
Public health policy interventions can use policy core components to encourage, induce, or support intermediaries to adopt and implement evidence-based programmatic interventions; these interventions use individual-level core components to improve health-related behaviors among populations of interest 35 (Figure 2B). An example is the group of policies that reduce liability for bystanders who use automatic external defibrillators (AEDs) on people experiencing out-of-hospital cardiac arrest. The ultimate agents of this policy are bystanders using AEDs. Their ability to use AEDs, however, depends on the actions of intermediaries, which include property owners who decide whether to purchase and install AEDs and the judges and juries whose discretion to impose awards for damages against those using AEDs is limited by laws such as the immunity law in Ohio. 36 The programmatic core components trigger mechanisms that are physiologic (ie, the AED’s ability to deliver appropriate electronic pulses to the heart), logistical (ie, the AED’s ability to reduce time to treatment), and informational (ie, the automated instructions provided by AEDs to guide bystanders through their use). In contrast, the core components of the liability policies include a mix of legal factors (ie, limitations on judges’ discretion to award damages) and perceptual factors (ie, changes in potential bystanders’ and property owners’ perceived risk of legal liability). Thus, the ultimate effect of the policy comes through the multilevel combination of liability policy core components, AED technology, and individual-level behavioral factors.
Type 3: Policy Core Components That Induce Intermediaries to Adjust Upstream Drivers of Health
A third type of interaction comprises public health policy interventions that first use policy core components to affect the actions of intermediaries that adjust upstream drivers; then, in the context of adjusted upstream drivers, intermediaries operate as agents and act through policy core components to affect population behavior (Figure 2C). This type of interaction differs from type 2, in which policy core components are used to support and facilitate the uptake of programmatic interventions and, therefore, intermediaries, when acting as agents, use “program” core components to affect behavior at the population level. An example of type 3 is the use of licensing or zoning policies (policy core components) that affect the decisions of alcohol vendors (intermediaries) about where to position themselves in a community (adjustment of the upstream driver). The intermediaries’ decision on location, in turn, is affected by policies governing community alcohol outlet density (ie, the number of places in a given area that can legally sell alcohol), which operate through additional policy core components to then affect population behavior and health (by affecting the overall availability of alcohol in a community). 37 Other examples of type 3 interactions that use core component thinking include local planning and zoning commissions, which make decisions that affect the price and availability of housing and green spaces and the walkability of neighborhoods; local water boards, which affect the price and quality of water provided by distribution systems; and employers, who affect the availability of health insurance and paid leave for their employees. In other examples of type 3 interactions, the policy core components involve altering decision-making structures to encourage health-promoting policy decisions, such as the use of health impact assessments when planning public infrastructure investments.37,38 Other examples might include core components emerging from Health in All Policies approaches 39 or community health needs assessment initiatives. 40
Advancing the Analysis and Use of Policy Core Components: Next Steps
Our 3 examples show how policy core components can interact with programmatic core components to shape changes in population-level behavior. Fully realizing the promise of core components, however, will require generalizing beyond examples and establishing research strategies.
Efforts to advance core component thinking for public health policy interventions could draw on existing literature on policy tools. For example, Salamon provided a broad typology (a grouping of things by how they are similar) that included tools such as direct provision of government benefits, economic and social regulation, tax subsidies, loan guarantees, and creation of governmental or quasi-governmental corporations. 28 Similar typologies have been provided by Schneider and Ingram, Linders and Peters, and Hood and Margetts.41-43 For the most part, however, these typologies remain general in nature, with relatively little effort to link policy core components to individual-level behavior and decision-making. A notable exception is the behavior-change wheel from Michie et al, which sketches out how various policy tools (eg, fiscal measures, service provision, regulation) might promote the adoption and spread of intervention types (eg, modeling, enablement, training). These intervention types thus shape individual behavior through one’s capabilities, opportunities, and motivations—a framing similar to our type 1 interaction. 35 Yet, as we maintain, programmatic and policy core components often interact at multiple levels to produce population-level behavior change (type 2 and 3 interactions).
Moreover, existing frameworks provide few explicit links to theories and evidence bases that illuminate the behavior of agents and intermediaries, not just individuals. We suggest that understanding agent and intermediary behavior requires more focus on scientific literature on organizational behavior, industrial organization, public administration, political science, and other fields with a more meso or macro focus. Thus, where previous work on core components focused on individual behavior change, future work on policy core components can focus on strategies to shape the behavior of organizations and institutions. For example, building evidence about incentives can include studies of how incentives affect the collective behavior of firms and other organizations. Incentive “signals” may be mediated through organizational rules, routines, authority structures, communities of practice, and patterns of interorganizational cooperation and competition.44 -48 Storr et al provided a real-world example, describing the processes of evidence synthesis and expert consensus leading to the identification of 8 core components of infection prevention and control policies for hospitals and national organizations. 49
On the basis of these observations, we offer 3 research strategies that could advance our collective thinking on policy core components: (1) identification of reliable approaches and rigorous techniques to break down policies into their components, (2) creation of tools to assist in differentiating between policy core components and noncore components, and (3) exploration of which policy core components are effective in shaping population health outcomes.
Public Health Implications
More practically, thinking in terms of core components by policy makers would involve a shift in the unit of analysis of evidence-based public health policy. Instead of policy makers viewing policy interventions as unitary “black boxes,” policy interventions could be viewed as configurations of core components—a perspective that captures the tendency for public health policies to be multicomponent in nature. Core components are currently viewed as those elements that must be maintained with little or no change to realize the intervention’s intended effect. Thinking in terms of policy core components can in turn help public health practitioners understand how interventions can produce changes at the population level, usually through multilevel interactions among agents.
Decision makers seeking to conceptualize public health policy interventions as multilevel configurations of core components can help address the paucity of evidence on policy interventions by placing the focus on accumulating and reviewing evidence of the most important parts of the interventions. Filling this evidence gap is the basic logic of proposals for rapid reviews of public health policy interventions, such as those proposed by Barbero et al, which begin by identifying core components, evaluating each component against criteria related to effectiveness and evidence quality, and then synthesizing the 2 parts to generate an overall impact rating.15,16 Advancing these applications of “policy core component thinking” can position decision makers to increase their understanding of what features of proposed policies are likely to work, under what circumstances they will work, or how they will work.
However, core components are viewed as a complement, not a substitute, to the traditional holistic approaches to evidence. An important limitation of the core components approach is that the overall effects of interventions are often nonadditive. That is, the effects of one core component may depend on the other core components in the intervention and how well each core component performs. Thus, evidence assessments of policy interventions based on core components alone may miss or at least understate “zero factors”—that is, situations in which the failure of any single component may render the others to be ineffective.50,51 As a result, by interpreting evidence reviews based on core components as judgments of potential or likely effectiveness, policy makers can plan for a careful, ongoing evaluation and monitoring of policy interventions as they are being developed and scaled up. Because research on programmatic core components to identify reliable and valid techniques is still in a nascent stage, policy practitioners can learn from that field as research progresses. Moreover, we suggest that adhering to our proposed research strategies can help address this limitation—first by identifying how to break down policies into their discrete components, followed by separating core components from noncore components, and finally by studying which core components improve health outcomes.
Policy makers, researchers, and practitioners have an opportunity to deepen their understanding of not just which policy interventions work but what elements and features may work and how they work. This expanded knowledge base can therefore provide more explicit guidance on how to adapt policy intervention components to new or different populations and contexts. In this topical review, we show the relevance of core components to public health policy interventions and how research and practice on the topic might proceed.
Footnotes
Acknowledgements
The authors thank Sangita M. Baxi, MAS, Pardee RAND Graduate School, RAND Corporation, for her contribution to the research related to this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not represent the official position or policy of, or implied endorsement by, the Centers for Disease Control and Prevention, US Department of Health and Human Services, or US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a contract (Concepts in Public Health Policy Analysis; Nos. GS10F0275P and 75D30121P10093) between the RAND Corporation and the Centers for Disease Control and Prevention of the US Department of Health and Human Services.