
Abstract
Substance use and mental health disorders can result in disability, death, and economic cost. In the United States, rates of death from suicide, drug overdose, and chronic liver disease (a marker for alcohol abuse) have been rising for the past 15 years. Good public health surveillance for these disorders, their consequences, and their risk factors is crucially important for their prevention and control, but surveillance has not been conducted consistently in the states. In 2015, the Council of State and Territorial Epidemiologists convened a workgroup to develop a set of uniformly defined surveillance indicators that could be used by state and local health departments to monitor these disorders and to compare their occurrence in various jurisdictions. This report briefly describes the indicators and outlines the process used to develop them.
Keywords
In the United States, mental health and substance use disorders continue to be a major cause of mortality. In contrast to reductions in mortality from many other causes (eg, infectious diseases and most tobacco-related conditions), rates from suicide, drug overdose, and chronic liver disease (a marker for alcohol abuse) have risen during the past 15 years. 1 -3 The US age-adjusted suicide rate for all ages increased from 10.5 per 100 000 population in 1999 to 12.9 per 100 000 population in 2014. Rate increases per 100 000 population were higher for non-Hispanic white people (from 12.0 in 1999 to 16.4 in 2014) than for people in other racial/ethnic groups. Drug overdose deaths are now a national epidemic and have been called by the director of the Centers for Disease Control and Prevention (CDC) “the public health crisis of our time.” 4 US age-adjusted death rates per 100 000 population from opioid overdose rose from 2.5 in 2000 to 9.0 in 2014. The age-adjusted death rate per 100 000 population for heroin-related drug poisoning nearly tripled from 2010 (1.0) to 2014 (3.4). 1
Chronic liver disease and cirrhosis (both largely the result of excessive alcohol use) are a part of rising mortality. The overall US age-adjusted death rate per 100 000 population from chronic liver disease and cirrhosis rose from 9.6 in 1999 to 10.2 in 2013. Age-specific rates during the same period, however, increased substantially among adults aged 45-64 (from 17.4 to 20.1 for adults aged 45-54 and from 23.7 to 30.4 for adults aged 55-64). CDC estimated that in 2013, 29 000 deaths were attributable to alcohol, a substantial increase from 25 500 in 2010. The overall 2013 death rate from alcohol-related causes was 9.2 per 100 000 population; the highest rate (25.3) was among adults aged 55-64. Of these deaths, 74% were among men and 86% were among non-Hispanic white people. 1
These alarming death rates from drug overdose and from mental health disorders do not, however, fully describe the total impact of these disorders on society.
5
-9
A statement from a 2016 Surgeon General’s report on alcohol, drugs, and health could apply easily to mental health disorders: The accumulated costs to the individual, the family, and the community are staggering and arise as a consequence of many direct and indirect effects, including compromised physical and mental health, increased spread of infectious disease, loss of productivity, reduced quality of life, increased crime and violence, increased motor vehicle crashes, abuse and neglect of children, and health care costs.
5
The economic effects of these disorders also are substantial. In 2006, an estimated $57.8 billion was spent in the United States on care for mental illness, similar to the amount spent on cancer treatment. 6 A 2014 literature review of the clinical and economic burden of prescription opioid use among people in the United States found that in 8 studies of prescription opioid abusers with private health insurance, the mean annual excess health care costs for opioid abusers (compared with those of a matched control group of nonabusers) ranged from $14 054 to $20 546. 10 According to one study, excessive drinking cost the United States $249 billion in 2010, which translated to $2.05 per drink. Most of these costs were the result of reduced workplace productivity, increased crime, and the cost of treating health problems caused by excessive drinking. 9
To prevent and control these disorders and their effect, public health agencies must have high-quality, timely information on their incidence, prevalence, risk factors, and consequences. Such information is obtained through the methods of public health surveillance. To conduct surveillance effectively, agencies must have an effective, practical set of surveillance indicators. By adopting a surveillance indicator for a particular disease condition, the Council of State and Territorial Epidemiologists (CSTE) signals that an agreement has been reached among public health agencies that (1) the condition is important to put under surveillance; (2) federal, state, local, territorial, and tribal public health agencies should establish surveillance for that condition using specified data sources, time intervals, ways of subdividing the population, and definitions of events to be counted; (3) agencies should share the collected data with CDC; and (4) summaries of the data should be made public on a regular schedule. The condition (ie, the thing being monitored) can be a death from a disease, an incident case of a disease, an episode of health care for a disease, a health-related behavior or risk factor, an adverse exposure (eg, to poor air quality or cigarette smoke), or levels of hazardous substances in the environment that are continuously measured. Surveillance indicators allow for monitoring a condition over time in a uniform way, thus making it easier for disease control program managers to design and evaluate prevention and control programs. Uniform indicators also allow rates of various conditions to be compared among jurisdictions.
CSTE undertook the project described in this article to produce and implement a set of public health surveillance indicators for mental health and substance use for use by state and local health departments. The project will add national standardization to measurement of the determinants and impact of drug abuse and mental illness at a state and local level, in support of prevention and control programs. The project was undertaken with an understanding that the domains of mental health and substance use overlap and that multiple steps exist on the pathway from behavior through health impact to severe illness and death.
Background
CSTE has been involved with adopting and maintaining surveillance indicators for decades. Since the 1950s, CSTE has led the adoption and maintenance of a set of nationally notifiable conditions for (mostly) infectious diseases that are tracked by CDC’s National Notifiable Diseases Surveillance System. CSTE, along with its partners, has also worked to establish indicators for noninfectious diseases. Following the approach first laid out by Meriwether, 11 CSTE’s adoption of noninfectious disease surveillance indicators started with tobacco use in 1996, followed by occupational health (1996), chronic disease (1998), maternal and child health (1998), injuries (1999), poisonings (2000), environmental health (2001), and oral health (2002); subsequent updates occurred in most domains (eg, chronic disease in 2013, oral health in 2015). This experience with other noninfectious diseases proves useful for establishing surveillance indicators for substance use and mental health disorders.
CSTE has been concerned with monitoring substance use and mental health disorders for many years. In 2007, CSTE established the Substance Abuse Subcommittee in partnership with the US Department of Health and Human Services’ Substance Abuse and Mental Health Services Administration (SAMHSA) and key CDC programs. In June 2017, this CSTE subcommittee updated its name to the Substance Use and Mental Health Subcommittee (SU/MH Subcommittee) to emphasize the independent importance of mental health and substance use issues, as well as their overlap. This subcommittee coordinates epidemiologic support within CSTE for state, local, tribal, and territorial prevention and intervention efforts related to these topics. To do this, the subcommittee oversees work being done on these topics by other CSTE subcommittees (ie, Alcohol and Other Drugs Indicators, Overdose, Prescription Drug Monitoring Program, Alcohol, Marijuana, and Mental Health). All of these subcommittees are chaired by CSTE-member epidemiologists working at the state or local level.
CSTE’s formal work on substance use and mental health surveillance indicators began in 2015 when the SU/MH Subcommittee convened a Substance Abuse and Mental Health Surveillance Indicator Workgroup comprising experts in the epidemiology of substance use and mental health conditions. Workgroup members represented 10 state or local public health and/or federal agencies across the United States. The workgroup was charged with (1) determining the surveillance needs of state, local, territorial, and tribal public health agencies in the domains of substance abuse and mental health and (2) developing a set of CSTE surveillance indicators in these domains, including case definitions for reporting, to be voted on by the CSTE membership at the 2016 annual meeting. This report describes the history, methods, and results of the process for developing national surveillance indicators in these domains.
Methods
The Substance Abuse and Mental Health Surveillance Indicator Workgroup met monthly via telephone from June through December 2015 to discuss, select, and develop a set of indicators in these domains. Workgroup members attended a total of 7 conference calls and one 2-day in-person meeting. During that time, the workgroup completed the following steps: Step 1. Identified the scope of the health domains to be included (eg, should use of tobacco and health consequences of such use be included in the scope?) Step 2. Identified broad topic areas for inclusion (eg, depression, suicide, overall mental health, use of various drugs with abuse potential, alcohol use) Step 3. Identified indicators developed by other groups that might be used directly or as models for indicators to be chosen for this project Step 4. Narrowed the topic areas the workgroup wanted to address into brief descriptions of indicators for inclusion (eg, incidence of emergency department visits for self-harm; prevalence of serious mental illness as defined by SAMHSA’s National Survey on Drug Use and Health [NSDUH]
12
; prevalence of current use of various drugs with abuse potential, from NSDUH; volume of narcotic drugs sold per capita by state; and hospitalization rates for nonfatal drug overdoses) Step 5. Finalized a set of indicators with rationales and definitions in a standard CSTE format
In step 1 (scope), the workgroup decided not to include tobacco-related indicators because a rich set of such indicators is already included in the CDC chronic disease surveillance indicator set. 13 The workgroup decided to include suicides due to all causes, including those due to drug overdose. The workgroup deemed specific surveillance for certain other serious and important mental health disorders (eg, schizophrenia) or for developmental disorders (eg, autism) to be out of scope. This was because consensus surveillance methods for these other conditions do not yet exist, nor do consistent data sources that could be used for their surveillance. In step 2, the workgroup identified a set of broad topic areas in which to develop surveillance indicators.
In step 3, the workgroup identified and assessed more than 50 brief descriptions of indicators for possible inclusion, from many of these sources and from input by workgroup members. SAMHSA, Healthy People 2020, the National Institute on Drug Abuse, the CSTE Chronic Disease Steering Committee, and the Safe States Alliance had all developed lists of indicators for various purposes. For example, SAMHSA had sponsored the development of a set of measures under the heading State Epidemiologic Data System. 14 Although this system is no longer active, the workgroup included the components of that system in its list of candidate indicators. SAMHSA publishes an extensive series of annual state and national reports—for example, various state estimate reports and the Behavioral Health Barometers 15,16 —that draw on the agency’s own rich data resources, including NSDUH. 12 The workgroup considered topics addressed in SAMHSA’s family of reports for inclusion.
The US Department of Health and Human Services Healthy People 2020 17 objectives are measurable and supported by well-defined data sources that jurisdictions can use to measure progress toward target outcomes. These objectives are a rich source of potential surveillance indicators. Several states have published surveillance summary documents for behavioral or mental health disorders, 18,19 and the workgroup reviewed these documents to identify potential indicators.
CSTE’s previously adopted chronic disease surveillance indicators 13 and the Safe States/CDC State Injury Indicators 20 include items related to alcohol, overall mental health, drug overdose fatality, and suicide attempts, some or all of which could be adopted as part of the eventual set of drug use and mental health indicators.
The workgroup went through 3 rounds of prioritization, using a modified Delphi method,
21
to identify indicators for the final set. Workgroup members considered the following criteria to aid in choosing surveillance indicators for substance use and mental health for inclusion in the recommended set. The workgroup suggested to its members that the presence of 1 or more of the following factors should increase a candidate indicator’s priority in the ranking process: The indicator quantifies the occurrence of a clinically severe condition, with a high risk of hospitalization or death (severity). The condition occurs commonly and contributes to overall morbidity or mortality (frequency). The condition is responsible for substantial economic impact, either in cost of medical care or in lost productivity and years of life (economic impact). The condition is preventable, with a feasible method for preventing or controlling the condition or its consequences (preventability). Information based on population-based surveillance for the condition is needed to support planning or evaluation of disease prevention and control activities (planning and evaluation).
For step 4, the workgroup reviewed the approximately 20 indicator topics that resulted from the review and prioritization process at an in-person meeting in Chicago, Illinois, on October 19-20, 2015. At that meeting, the workgroup divided into 2 groups—one to address substance use issues and the other to address mental health issues—and then came together to prioritize indicators across both domains. During the in-person workgroup process, some candidate indicators were moved to a developmental status (for possible inclusion in later iterations of the set of indicators), some were split, some were consolidated, and 2 indicators were added, resulting in a set of 18 indicators (some with multiple subindicators).
The workgroup developed definitions for each indicator in 3 ways: (1) where there was an existing indicator definition in the CSTE chronic disease 13 or injury surveillance indicator 20 sets, the definition from that source was adopted; (2) where there was a draft indicator in development by a CSTE workgroup, that definition was adopted; and (3) for new indicators, the workgroup developed an indicator definition de novo. These definitions for each indicator addressed the demographic group to be covered in surveillance reports about the indicator, the definition of the numerator and the denominator (if the indicator was a proportion or rate), further specification of the measure (eg, crude or age-adjusted rate), the period of time for which the data were to be reported, the data resource to be used, stratification variables, background and significance for the indicator, limitations of the indicator and of the data source from which it was derived, how to access the data, and related Healthy People 2020 objectives and CSTE surveillance indicators (Table).
Descriptions of substance abuse and mental health surveillance indicators adopted by Council of State and Territorial Epidemiologists, 2016
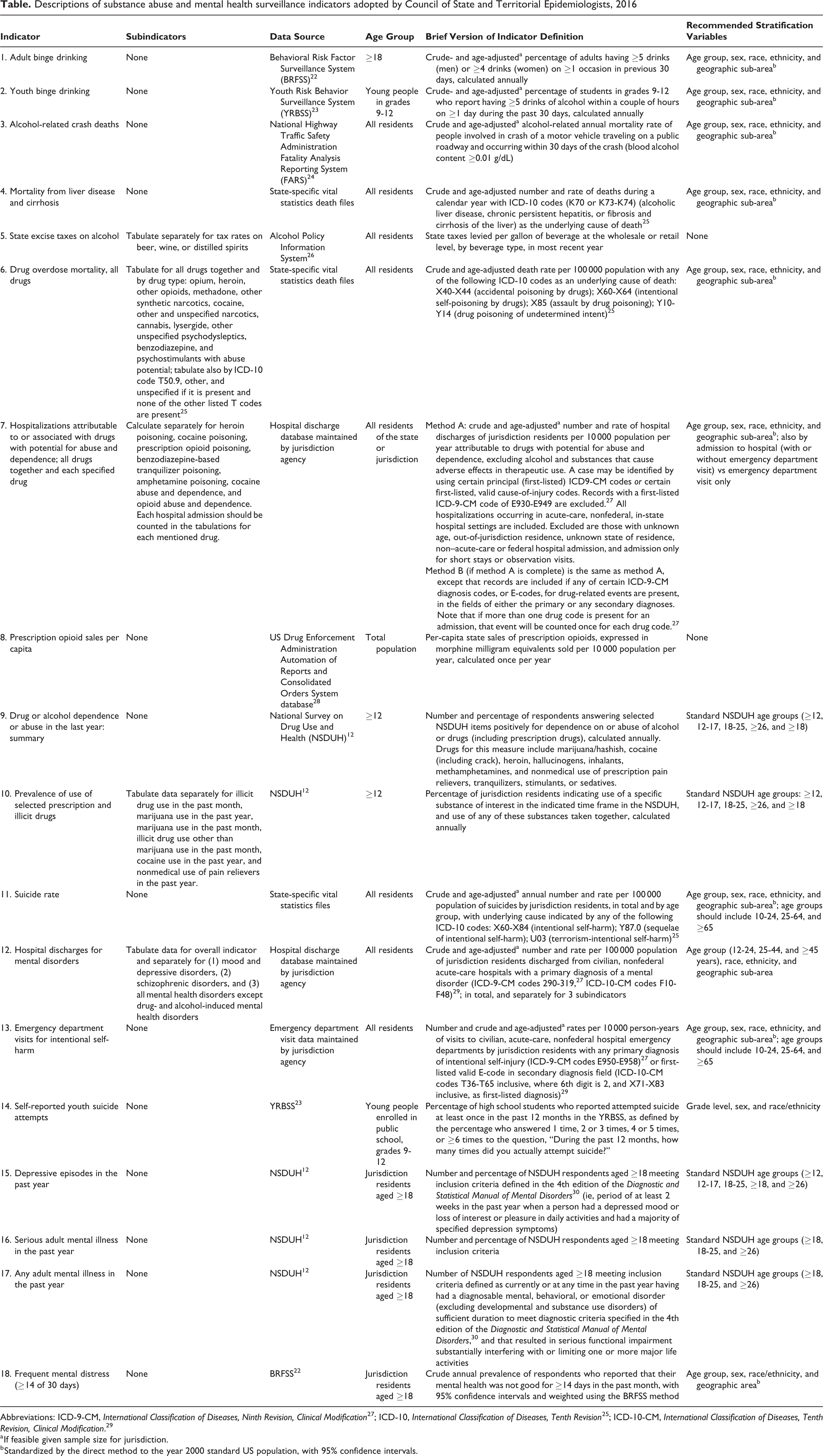
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification 27 ; ICD-10, International Classification of Diseases, Tenth Revision 25 ; ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification. 29
a If feasible given sample size for jurisdiction.
b Standardized by the direct method to the year 2000 standard US population, with 95% confidence intervals.
The workgroup attempted to include equal numbers of indicators in the substance use and mental health domains. The workgroup also included indicators in each domain that reflected the entire natural history of the relevant condition, from the policy environment (eg, alcoholic beverage taxes) through preclinical stages (eg, number of monthly days of poor mental health, frequency of binge drinking or of marijuana use), and morbidity (eg, hospitalizations for mental health disorders or drug abuse) to mortality (eg, suicide, alcohol-related causes). Of these indicators, 4 were derived from death records collected by vital statistics departments, 3 were derived from hospital discharge and emergency department visit data sets, 2 were derived from the Behavioral Risk Factor Surveillance System, 2 were derived from the Youth Risk Behavior Surveillance System, 5 were based on published NSDUH data, 1 was based on the US Drug Enforcement Agency’s Automation of Reports and Consolidated Orders System database of prescription opioid sales, and 1 was based on the National Institute of Alcohol Abuse and Alcoholism’s Alcohol Policy Information System. Of these indicators, 2 represented determinants of behavior, 6 represented behaviors or early manifestations of disease, 6 represented morbidity related to these behaviors, and 4 represented mortality that was the end-point of these behaviors and disease processes.
CSTE staff members took the brief indicator descriptions from the Chicago meeting and drafted complete indicator definitions in a standard format. In step 5, the workgroup reviewed, revised, and eventually approved the indicator definitions.
Recommendations
A representative of the workgroup presented full descriptions of the 18 indicators, including their definitions (Table), as a position statement 31 at the CSTE annual meeting in June 2016. CSTE posted complete indicator definitions on its website as part of a white paper on surveillance indicators for substance abuse and mental health. 32 The CSTE position statement recommending the 18 selected indicators was approved by vote of CSTE at its 2016 annual meeting in Anchorage, Alaska, which in effect constituted a recommendation from CSTE to state and local health departments to use these 18 indicators to measure and monitor substance abuse and mental health in their jurisdictions. Data collection and analysis may be conducted primarily by state or local staff members, by federal staff members, or collaboratively. CSTE monitors the implementation of position statements.
In addition to the recommended indicators, the workgroup identified several topics for future consideration 31 and referred them to various ongoing CSTE SU/MH subcommittees and workgroups for consideration and possible future development: state-level parity for mental health clinical care provided by third-party payers; characteristics of state Prescription Drug Monitoring Programs; all-cause alcohol-attributable mortality; hospital discharge rate for alcohol-related events; alcohol-related emergency department visits based on hospital discharge data; rapid drug overdose mortality for all drugs, using electronic death registration capabilities; emergency department visits attributable to or associated with all drugs through syndromic surveillance data systems; and additional indicators related to use and adverse health effects of marijuana, to monitor effects of decriminalization of marijuana use.
Public Health Practice Implications
In early 2017, CSTE selected 4 states (Michigan, Minnesota, New Mexico, and North Carolina) to field-test the implementation of these surveillance indicators. Results from the 4 pilot states were presented at the CSTE annual conference in Boise, Idaho, in June 2017. The SU/MH subcommittee reviewed recommendations from the 4 field-test states and made small technical revisions and clarifications to the methods for the 18 indicators, without changing their substance. These revisions were incorporated into a second version of the recommendations, which was released in early 2018. 33 In March 2018, CSTE launched a second round of pilots; 10 states and 5 local health departments were selected to provide state- and county-level data. This second pilot will be completed by July 2018. CSTE intends to continue to support national implementation of the indicators to achieve standardized surveillance of these key behavioral health indicators.
Footnotes
Acknowledgments
The authors thank the following people from the CSTE Substance Abuse and Mental Health Surveillance Indicator Workgroup for their commitment and dedication to developing the recommended surveillance indicators for substance abuse and mental health: Alejandro Azofeifa, PhD, and Patrick High, PhD, SAMHSA; James W. Davis, MA, and Luigi Garcia Saavedra, MPH, New Mexico Department of Health; Hal Johnson, MPH, Hal Johnson Consulting; Thomas Largo, MPH, Michigan Department of Health and Human Services; Denise Paone, EdD, and Ellenie Tuazon, MPH, New York City Department of Health and Mental Hygiene; Jessica Reno, MPH, University of New Mexico; Jennifer Sabel, PhD, Washington State Department of Health; Cathy Saiki, MS, and Steve Wirtz, PhD, California Department of Health; Svetla Slavova, PhD, Kentucky Injury Prevention and Research Center; and Toby Yak, MPH, Iowa Department of Public Health. The authors also thank Rob Lyerla, PhD, MGIS, SAMHSA; Donna F. Stroup, PhD, MSc, Data for Solutions, Inc; and Nidal A-Z Kram, CSTE, for their contributions to this project and the report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Recommended Surveillance Indicators for Substance Abuse and Mental Health project was supported by SAMHSA (agreement #14-OA-22-20-206). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the New Mexico Department of Health, the University of Florida, SAMHSA, or CSTE.