
Abstract
Objective:
The objective of our study was to assess meningococcal ACWY (MenACWY) vaccine uptake among men who have sex with men (MSM) during an ongoing, invasive meningococcal disease outbreak in Southern California. This research was important to inform future vaccination uptake interventions for this high-priority population.
Methods:
We conducted venue-based sampling to recruit and enroll MSM living in Los Angeles County, California, from December 2016 through February 2017. We conducted bivariate and multivariable analyses to evaluate associations between MenACWY vaccine uptake and other predetermined factors.
Results:
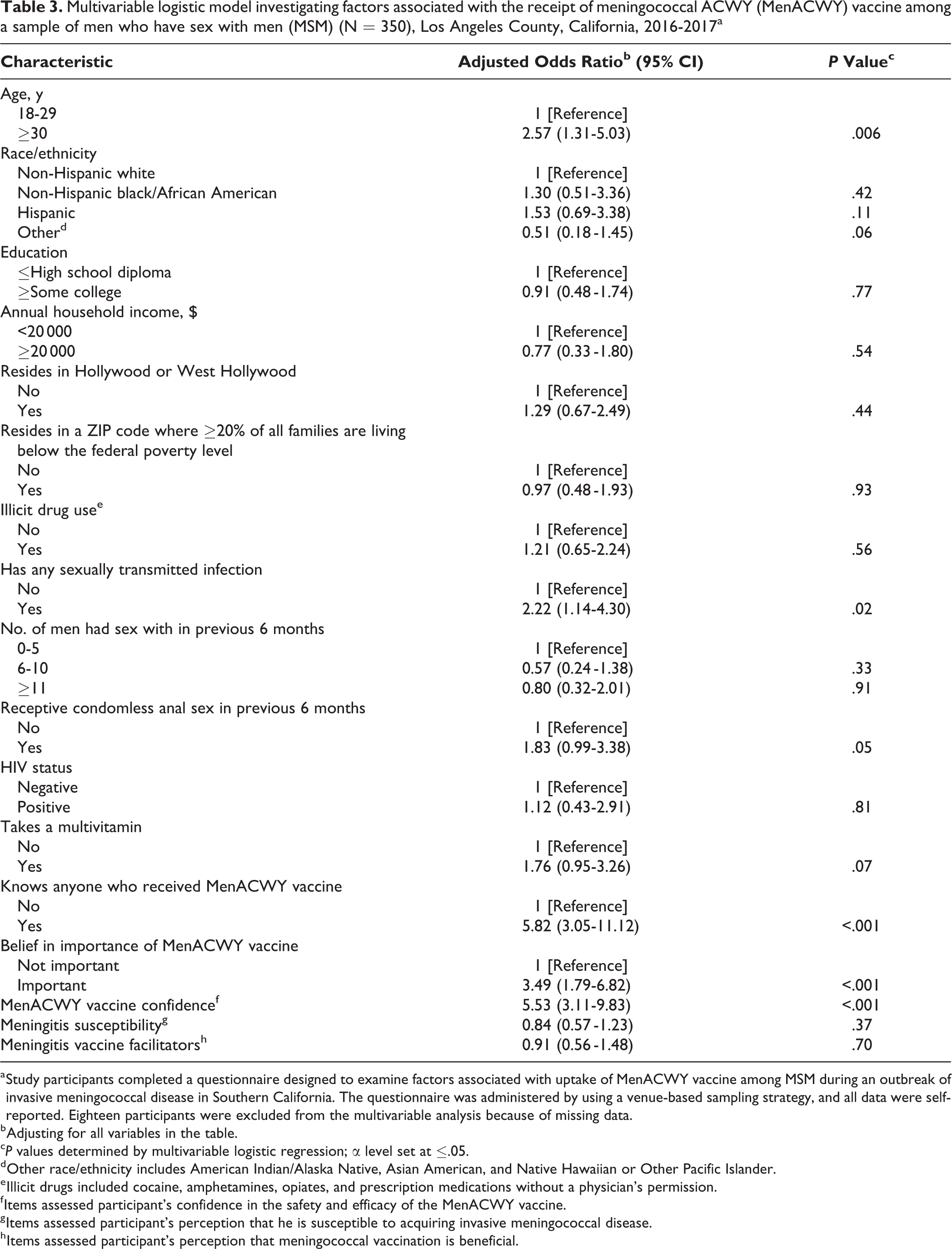
Of 368 participants, 138 (37.5%) reported receiving the MenACWY vaccine. In multivariable analyses, older age (adjusted odds ratio [aOR] = 2.57; 95% confidence interval [CI], 1.31-5.03), previous diagnosis of a sexually transmitted infection (aOR = 2.22; 95% CI, 1.14-4.30), belief that MenACWY vaccine is important (aOR = 3.49; 95% CI, 1.79-6.82), confidence in the MenACWY vaccine (aOR = 5.53; 95% CI, 3.11-9.83), and knowing someone who had been vaccinated (aOR = 5.82; 95% CI, 3.05-11.12) were significantly associated with MenACWY vaccine uptake.
Conclusions:
Our findings reflect low uptake of the recommended MenACWY vaccine among MSM after a local outbreak, despite public health efforts. In addition to ongoing, widespread campaigns to inform MSM about local outbreaks and vaccination recommendations, MSM may be responsive to direct outreach from peers who have been vaccinated.
Keywords
Reports of invasive meningococcal disease (IMD) outbreaks in the United States and worldwide have been published since the mid-1990s, 1 -3 including outbreaks in communities of men who have sex with men (MSM). 4 IMD is characterized by a sudden clinical onset of high fever, headache, nausea, vomiting, rash, stiff neck, and confusion that can lead to meningococcal meningitis and/or meningococcal septicemia. If not treated, these infections can be deadly in a matter of hours. The mortality rate of IMD is high (approximately 10%-30% of people infected with IMD die), and IMD can result in loss of limbs, loss of hearing, and damage to the central nervous system and kidneys. 5,6
From March 2016 through July 2017, an outbreak of 31 cases of IMD, primarily among MSM, occurred in Southern California. 7,8 Five of the 31 cases were people living with HIV/AIDS (PLWHA). 7 In response to this outbreak, the California Department of Public Health issued a health advisory in August 2016 recommending 2 doses of meningococcal ACWY (MenACWY) vaccine for adult PLWHA and 1 dose of MenACWY vaccine for all MSM not living with HIV/AIDS in Southern California. 9 This recommendation was a change from a previous MenACWY vaccination recommendation for MSM, which applied to MSM who had close or intimate contact with multiple partners or sought partners through the use of social networking applications, particularly MSM who shared cigarettes or marijuana, or used illegal drugs. 10
At a meeting in June 2016, the Advisory Committee on Immunization Practices (ACIP) recommended a 2-dose primary series of the MenACWY vaccine, with doses 2 months apart, followed by a booster vaccine every 5 years for all HIV-infected people aged ≥2 months. 11 -13 This recommendation was published in Morbidity and Mortality Weekly Report in November 2016. 11 Despite wide dissemination of updated recommendations, health care providers attending to PLWHA may not have been knowledgeable about them. 14,15 Differences in adult immunization recommendations according to certain patient demographic characteristics (eg, age, comorbidities) and confusion about contraindications and precautions may also have created informational barriers for health care providers. 16 -18 In addition to the challenges of keeping abreast of immunization recommendations, not all providers use recommended immunization schedules. In one survey, only 60% of physicians and 56% of physician assistants, nurse practitioners, and registered nurses reported using official guidelines as their source of information about adult immunizations. 19 Informational barriers also impede patient receipt of immunizations; the rate of receipt for the second dose of the MenACWY vaccine was low (26.6%) among PLWHA as of December 2015, 20 possibly because of a lack of awareness about the necessity of a second dose or the misperception that CD4 counts will decrease and viral loads will increase after vaccination. 21,22
Delays in reporting, low participation rates among adults, limited sociodemographic information, and incomplete data in state immunization registries make it difficult to discern rates of MenACWY vaccine coverage among MSM. 23,24 Fewer than half of adults in California have 1 or more vaccination records in the California Immunization Registry, a centralized state registry of vaccination records submitted by vaccination service providers (eg, physicians, pharmacists), and sexual orientation data are not collected for people who are included. 23 Few surveys assessing vaccination coverage among MSM have been conducted in California, and none attempted to quantify coverage beyond a specific vaccine type or limited geographic region. 18,25 -27 Therefore, comprehensive vaccination coverage among MSM in Southern California is not known. The objective of our study was to describe MenACWY vaccine uptake among MSM, including MSM living with HIV, in Los Angeles County, California. This information could help to detect potential gaps in uptake that could result in an underimmunized cluster in Los Angeles County and identify factors associated with underimmunization. 28
Methods
Theoretical Framework
To examine factors that may contribute to MenACWY vaccine uptake among MSM, we used a socioecological framework for empirical investigation of multiple levels of influence. 29 From a conceptual standpoint, immunization decision making is informed by a series of events driven by an entire ecological system, which includes direct and indirect influencers. This model specifies 3 levels of behavioral dynamics: individual, social/contextual, and structural. The individual level refers to factors, such as perception of disease vulnerability, that are specific to the individual. The social/contextual level involves immunization decision-making support from peers and other people with whom an individual has a socially close relationship. Interactions at this level are theorized to have a strong effect on an individual’s health decision making because of social network dynamics. The structural level represents policies and recommendations affecting MSM’s health interests locally (eg, local or regional recommendations for meningococcal immunization in the context of an outbreak). 29 By identifying influences on the MenACWY vaccination behavior of MSM, we sought to uncover the socioecological factors that could be shaped into useful vaccine promotion interventions for MSM in Southern California.
Study Design and Sample
From December 2016 through February 2017 (the study period), we executed a rapid-response venue-based sampling strategy to gather survey data from MSM in selected venues in Los Angeles County. This method has been successful in obtaining similar representative samples in serial cross-sectional studies, such as the National HIV Behavioral Surveillance survey.
30,31
Our venue sample included 146 locations, including clinics, community-based organizations, AIDS service organizations, specialized businesses serving the LGBTQ (lesbian, gay, bisexual, transgender, queer/questioning) community, bathhouses, stores, bars, clubs, recreational areas and facilities, and restaurants and coffee shops. We developed this list based on previous work by the first author (I.W.H.) with MSM in Los Angeles County and guidance from a standing community advisory board consisting of representatives from the community-based agencies with whom the Southern California HIV/AIDS Policy Research Centers collaborate. We collected data in 4-hour blocks in the morning and early afternoon (10
Recruiters asked a brief series of 7 standardized questions to men who expressed interest in the survey and recorded responses on an iPad to assess their eligibility. Men were eligible to enroll if they met the following criteria: (1) were aged ≥18, (2) were assigned male sex at birth, (3) identified as male, (4) reported having sex with men in the past 3 months, (5) resided in Los Angeles County, (6) spoke English or Spanish, and (7) were able to provide informed consent. Eligible participants were invited to take a 15- to 30-minute survey (mean, 17.7 minutes), which was conducted by trained interviewers on iPads outside of the venue. Participants received a $50 cash incentive for participating. The UCLA North General Institutional Review Board reviewed and approved the study before survey implementation.
Survey Instrument and Measurement
We developed the consent form, the series of questions for assessing participant eligibility, and the survey instrument in English and Spanish by using forward-backward translation. The Flesch Reading Ease scale (62.9) and Flesch-Kincaid grade (7.1) were acceptable, corresponding to a sixth- to eighth-grade level. 32 The readability of materials was in the standard range (between “fairly easy” and “fairly difficult”) according to the Flesch Readability Chart. 33 To assess vaccination status, we asked respondents, “Quadrivalent meningococcal vaccination is a vaccination that protects against 4 types of meningitis; have you received quadrivalent meningococcal vaccination?” Participants could respond yes, no, or “not sure.” Our analysis included participants who responded yes or no to this item and excluded those who responded “not sure.”
We collected data on sociodemographic characteristics, including age (18-29, ≥30), race/ethnicity (non-Hispanic white, non-Hispanic black/African American, Hispanic, and other), health insurance (yes/no), highest level of education completed (≤high school diploma, ≥some college), employment status (employed full time, other), and annual household income (<$20 000, ≥$20 000). To classify participants by race/ethnicity, we first asked about ethnicity (Hispanic or non-Hispanic) and then asked about race using US Census categories (non-Hispanic white, non-Hispanic black/African American, Hispanic, and other, which included American Indian/Alaska Native, Asian American, and Native Hawaiian or Other Pacific Islander).
We also collected data on individual risk and protective factors, including data on marijuana use, illicit substance use (eg, cocaine, amphetamines, opiates, prescription drugs without a physician’s permission), sexual behavior (eg, condomless anal sex), HIV status, diagnoses of sexually transmitted infections (STIs), and multivitamin use. The questionnaire also included items designed to measure psychosocial indicators of attitudes and perceptions about immunization decision making. One item asked participants to indicate whether MenACWY vaccination was important to them (yes/no), and another asked if participants knew anyone who had received MenACWY vaccination (yes/no).
The survey assessed the following 3 psychosocial categories on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree) 34 : (1) barriers to receiving the MenACWY vaccine (6 items), (2) perceived susceptibility of acquiring meningococcal disease (4 items), and (3) perceived benefits of MenACWY vaccination (4 items). Items assessing barriers to receiving the MenACWY vaccine included “I don’t have time to get vaccinated.” Items assessing perceived meningococcal disease susceptibility included “I am not at risk for getting infected with meningococcal disease” (reverse coded). Items assessing perceived benefits of MenACWY vaccination included “Getting vaccinated against meningococcal disease would be a good way to protect the health of my sex partner(s).” We also assessed participants’ confidence in the safety and efficacy of the MenACWY vaccine. We averaged the ratings of items in each category to create raw summary scores.
At the social/contextual level, we assessed the extent of participant engagement in social media and the number of platforms they were active on, with items such as “How often do you use social networking websites like Facebook, Twitter, Pinterest, or Instagram?” and “How many Twitter followers do you have?” In addition, we assessed the social norms and social influence of vaccination behavior. The social norms category included items such as “Most people I know are being vaccinated.” The social influence category included 5 items such as “I often persuade others to get vaccinated.” We measured the previously mentioned items by using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). 34
At the structural level, to account for meningococcal disease awareness campaigns that had occurred in Hollywood and West Hollywood, we used participants’ ZIP codes to determine residence in these targeted areas. We assessed neighborhood-level poverty by whether a participant lived in a ZIP code where ≥20% of all families lived below the federal poverty level. 35
Statistical Analysis
We evaluated characteristic differences between men who reported having received the MenACWY vaccine and men who reported not receiving the vaccine by using cross-tabulations and descriptive analyses in SAS/STAT version 9.3. 36 We conducted an exploratory factor analysis to identify factors associated with immunization decisions and assessed the internal consistency of each factor. We averaged the ratings of items that were measured on a 5-point Likert scale to create raw summary scores for each category. We determined that a Cronbach α reliability estimate of ≥0.60 would support the reliability of each factor associated with MenACWY vaccine uptake. 37 We conducted bivariate and multivariable correlations to assess associations between individual, social/contextual, and structural factors and MenACWY vaccine uptake. We used Pearson χ2 tests and Wilcoxon signed-rank tests to analyze associations between sets of the outcome variable and socioecological factors. We set significance at α = .10 for the bivariate level because this step was exploratory; in the multivariable models, we set significance at α ≤ .05. We entered significant correlates of MenACWY vaccination at the bivariate level and variables consistent with our conceptual framework into a multivariable model predicting MenACWY vaccination. The multivariable logistic regression analysis evaluated the association between independent variables and the dependent variable (ie, MenACWY vaccination) while adjusting for covariates.
Results
We approached approximately 2250 men to participate in the study. Our overall response rate was 69.4% (520 eligible respondents of 749 screened). Of these 520 participants, 368 responded yes or no to the question assessing MenACWY vaccination, and 152 were not sure about whether they had received the vaccine and were excluded from further analysis.
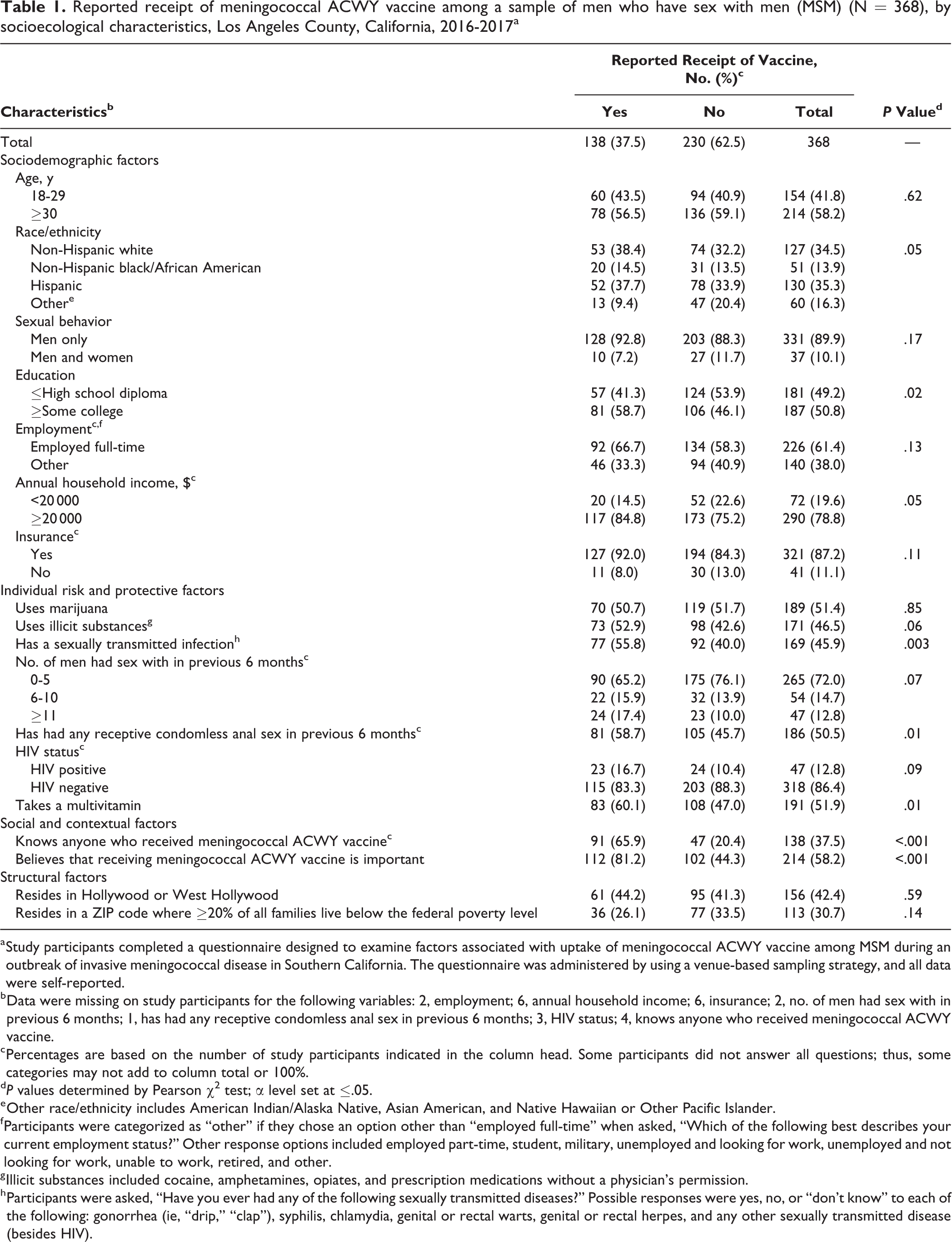
Participants were young (mean [standard deviation (SD)], 34.2 [10.4] years) and racially/ethnically diverse. Of the 368 participants, 127 (34.5%) identified as non-Hispanic white, 51 (13.9%) as non-Hispanic black/African American, 130 (35.3%) as Hispanic, and 60 (16.3%) as other (Table 1). Of the 368 participants, 187 (50.8%) were college educated, 72 (19.6%) made <$20 000 annually, 321 (87.2%) had health insurance, 156 (42.4%) resided in either Hollywood or West Hollywood, and 113 (30.7%) lived in areas where ≥20% of all families lived below the federal poverty level. Of the 368 participants, 331 (89.9%) reported sex with men only; 101 (27.5%) reported ≥6 sexual partners in the previous 6 months, 186 (50.5%) reported condomless anal sex in the previous 6 months, and 47 (12.8%) were HIV-positive.
Reported receipt of meningococcal ACWY vaccine among a sample of men who have sex with men (MSM) (N = 368), by socioecological characteristics, Los Angeles County, California, 2016-2017a
a Study participants completed a questionnaire designed to examine factors associated with uptake of meningococcal ACWY vaccine among MSM during an outbreak of invasive meningococcal disease in Southern California. The questionnaire was administered by using a venue-based sampling strategy, and all data were self-reported.
b Data were missing on study participants for the following variables: 2, employment; 6, annual household income; 6, insurance; 2, no. of men had sex with in previous 6 months; 1, has had any receptive condomless anal sex in previous 6 months; 3, HIV status; 4, knows anyone who received meningococcal ACWY vaccine.
c Percentages are based on the number of study participants indicated in the column head. Some participants did not answer all questions; thus, some categories may not add to column total or 100%.
dP values determined by Pearson χ2 test; α level set at ≤.05.
e Other race/ethnicity includes American Indian/Alaska Native, Asian American, and Native Hawaiian or Other Pacific Islander.
f Participants were categorized as “other” if they chose an option other than “employed full-time” when asked, “Which of the following best describes your current employment status?” Other response options included employed part-time, student, military, unemployed and looking for work, unemployed and not looking for work, unable to work, retired, and other.
g Illicit substances included cocaine, amphetamines, opiates, and prescription medications without a physician’s permission.
h Participants were asked, “Have you ever had any of the following sexually transmitted diseases?” Possible responses were yes, no, or “don’t know” to each of the following: gonorrhea (ie, “drip,” “clap”), syphilis, chlamydia, genital or rectal warts, genital or rectal herpes, and any other sexually transmitted disease (besides HIV).
Among the 368 participants, only 138 (37.5%) reported receiving the MenACWY vaccine. Among the 47 HIV-positive participants, 23 (48.9%) reported receiving the vaccine; of the 23 HIV-positive MSM who had been vaccinated, 19 (82.6%) reported receiving the vaccine in the previous 6 months. However, only 16 of the 23 (69.6%) HIV-positive participants who had been vaccinated reported completing the recommended 2-dose schedule, or 34.0% of all 47 HIV-positive MSM in our sample. Among the 318 HIV-negative participants, 115 (36.2%) reported receiving the MenACWY vaccine; of the 115 HIV-negative participants who had been vaccinated, 59 (51.3%) reported being vaccinated within the previous 6 months.
Bivariate and Multivariable Results
Compared with the percentage of participants who reported not receiving the MenACWY vaccine (106/230, 46.1%), a greater percentage (81/138, 58.7%) of participants who reported receiving the vaccine had some college or more (P = .02) (Table 1). Compared with fewer than half (92/230, 40.0%) of those who reported not receiving the MenACWY vaccination, more than half (77/138, 55.8%) of participants who reported receiving the vaccine had been diagnosed with an STI (P = .003).
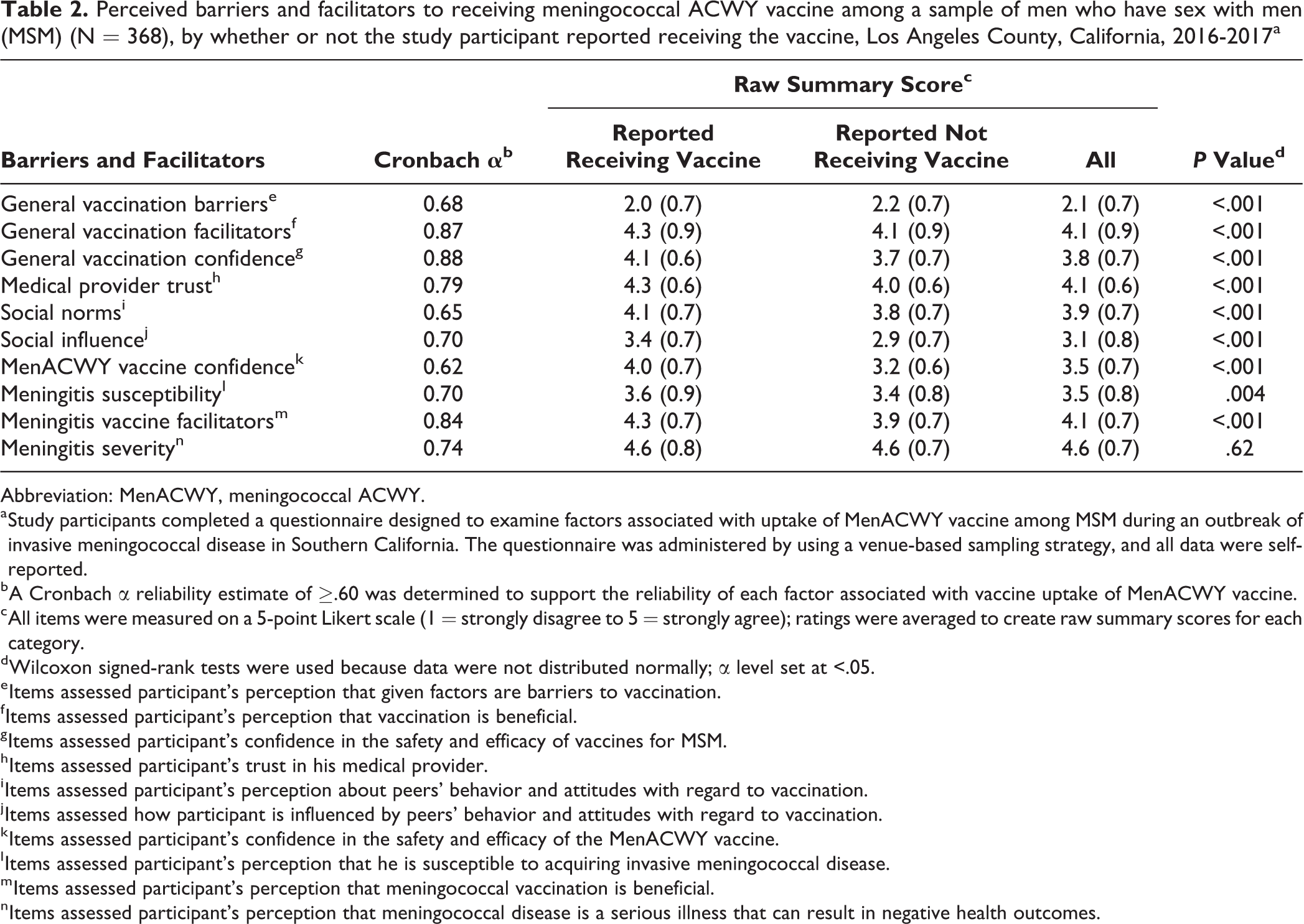
In the bivariate analysis of perceived facilitators and barriers to vaccination, participants who reported receiving the MenACWY vaccine had significantly lower scores (mean [SD] score = 2.0 [0.7]) on the items assessing barriers to receiving the vaccine compared with those who reported not receiving the vaccine (mean [SD] score = 2.2 [0.7]) (P < .001) (Table 2). Participants who reported receiving the MenACWY vaccine had significantly higher scores (mean [SD] score = 3.6 [0.9]) on the items assessing susceptibility to meningococcal disease (P = .004) than participants who reported not receiving the vaccine (mean [SD] score = 3.4 [0.8]).
Perceived barriers and facilitators to receiving meningococcal ACWY vaccine among a sample of men who have sex with men (MSM) (N = 368), by whether or not the study participant reported receiving the vaccine, Los Angeles County, California, 2016-2017a
Abbreviation: MenACWY, meningococcal ACWY.
a Study participants completed a questionnaire designed to examine factors associated with uptake of MenACWY vaccine among MSM during an outbreak of invasive meningococcal disease in Southern California. The questionnaire was administered by using a venue-based sampling strategy, and all data were self-reported.
b A Cronbach α reliability estimate of ≥.60 was determined to support the reliability of each factor associated with vaccine uptake of MenACWY vaccine.
c All items were measured on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree); ratings were averaged to create raw summary scores for each category.
d Wilcoxon signed-rank tests were used because data were not distributed normally; α level set at <.05.
e Items assessed participant’s perception that given factors are barriers to vaccination.
f Items assessed participant’s perception that vaccination is beneficial.
g Items assessed participant’s confidence in the safety and efficacy of vaccines for MSM.
h Items assessed participant’s trust in his medical provider.
i Items assessed participant’s perception about peers’ behavior and attitudes with regard to vaccination.
j Items assessed how participant is influenced by peers’ behavior and attitudes with regard to vaccination.
k Items assessed participant’s confidence in the safety and efficacy of the MenACWY vaccine.
l Items assessed participant’s perception that he is susceptible to acquiring invasive meningococcal disease.
m Items assessed participant’s perception that meningococcal vaccination is beneficial.
n Items assessed participant’s perception that meningococcal disease is a serious illness that can result in negative health outcomes.
In our multivariable model, age ≥30 (adjusted odds ratio [aOR] = 2.57; 95% confidence interval [CI], 1.31-5.03), a diagnosis of an STI (aOR = 2.22; 95% CI, 1.14-4.30), knowing anyone who had received the MenACWY vaccine (aOR = 5.82; 95% CI, 3.05-11.12), believing MenACWY vaccination was important (aOR = 3.49; 95% CI, 1.79-6.82), and having confidence in the MenACWY vaccine (aOR = 5.53; 95% CI, 3.11-9.83) were significantly associated with MenACWY vaccine uptake (Table 3).
Multivariable logistic model investigating factors associated with the receipt of meningococcal ACWY (MenACWY) vaccine among a sample of men who have sex with men (MSM) (N = 350), Los Angeles County, California, 2016-2017a
a Study participants completed a questionnaire designed to examine factors associated with uptake of MenACWY vaccine among MSM during an outbreak of invasive meningococcal disease in Southern California. The questionnaire was administered by using a venue-based sampling strategy, and all data were self-reported. Eighteen participants were excluded from the multivariable analysis because of missing data.
b Adjusting for all variables in the table.
cP values determined by multivariable logistic regression; α level set at ≤.05.
d Other race/ethnicity includes American Indian/Alaska Native, Asian American, and Native Hawaiian or Other Pacific Islander.
e Illicit drugs included cocaine, amphetamines, opiates, and prescription medications without a physician’s permission.
f Items assessed participant’s confidence in the safety and efficacy of the MenACWY vaccine.
g Items assessed participant’s perception that he is susceptible to acquiring invasive meningococcal disease.
h Items assessed participant’s perception that meningococcal vaccination is beneficial.
Discussion
Our study is among the first to examine MenACWY vaccination coverage in a sample of MSM in Southern California during an IMD outbreak. Despite recommendations by the California Department of Public Health and the Los Angeles County Department of Public Health, vaccination in response to this outbreak among HIV-negative and HIV-positive MSM in our sample was low. Currently, data on sexual practices or sexual orientation are not linked with data on vaccination in immunization registries, making our work especially important for understanding MenACWY vaccination coverage among MSM. 38,39 Recent IMD outbreaks have primarily affected MSM in Chicago, New York, Toronto, and Miami; coordinated efforts to improve immunization surveillance among MSM will enable better tracking of MenACWY vaccine uptake to assess local immunization rates across the country. 8,39,40
In accordance with our theoretical framework, we identified several individual-level factors associated with reported receipt of the MenACWY vaccine. We found that older age was associated with greater MenACWY vaccine uptake. This finding is consistent with findings from other studies that showed older MSM (aged ≥26) tended to have higher uptake of health-promoting behaviors, such as HIV testing 41 and pre-exposure prophylaxis, 42 than younger MSM (aged ≤25). Given recommended meningitis vaccination schedules, it is surprising that older age was associated with greater vaccination uptake. ACIP recommends MenACWY vaccination for all adolescents aged 11-18, with vaccination occurring at age 11 or 12 and a booster at age 16. 43 Another study reported increases in ≥1 MenACWY vaccine dose among boys and girls aged 13-17, from 76.6% in 2013 to 79.3% in 2014, 44 whereas the overall uptake among men aged 18-29 in our sample was 43.5%. Gay and bisexual adolescents may be more willing to adhere to vaccination guidelines as they roll out, given that many of them are included in groups for which MenACWY vaccination is recommended: first-year college students living in residence halls and military recruits. 45
Compared with MSM who reported not receiving the MenACWY vaccine, MSM who reported receiving the MenACWY vaccine were more likely to have a diagnosis of an STI. Other studies have found that recent diagnosis of an STI is a risk factor for meningococcal disease. 46 This finding, along with greater percentages of MenACWY vaccine uptake among MSM reporting receptive condomless anal sex (although not significant), suggests that those most at risk for meningitis may be more likely to be reached by IMD prevention messaging. Health providers who see MSM for STI treatment may be attuned to their susceptibility for other infectious diseases, including IMD, and prompt vaccination. 47,48 Future interventions to increase MenACWY vaccine uptake among MSM during outbreaks could ask STI clinics to disseminate vaccines to MSM.
Participants who reported receiving the MenACWY vaccine had a higher prevalence of HIV than did participants who reported not receiving the vaccine. However, this difference was not significant in our multivariable analysis. Of 23 HIV-positive MSM who received ≥1 dose of the MenACWY vaccine, 16 (70%) received a second dose. Thus, only 34% (16/47) of HIV-positive MSM in our sample had followed the 2016 ACIP recommendation of 2 MenACWY vaccine doses at the time of our survey. 11 However, some of these participants might not have been candidates for the second dose because the recommended interval between doses is 2 months. Interestingly, 83% (19/23) of vaccinated HIV-positive MSM (compared with 53% [59/115] of vaccinated HIV-negative MSM) had been vaccinated in the previous 6 months. The high percentage of HIV-positive participants who had been vaccinated in the previous 6 months suggests that PLWHA may be adhering to the 2016 ACIP recommendations targeting PLWHA. However, much work remains to be done to educate providers and patients, including disseminating comprehensive information about IMD, MenACWY vaccination, and appropriate dosing schedules. 39 This work is especially important for HIV-positive MSM, for whom 2 doses are required to achieve maximum vaccine efficacy.
MSM’s perceived susceptibility of acquiring meningococcal disease, belief in the importance of the MenACWY vaccine, and confidence in the MenACWY vaccine were associated with MenACWY vaccine uptake. These findings are in line with theoretical models of health behavior that emphasize susceptibility to disease as a key driver of behavior. 49 Public health education efforts may be enhanced by messages that emphasize personal health risks, the safety and efficacy of the MenACWY vaccine, and the importance of meningococcal vaccines for men’s health in jurisdictions with IMD outbreaks. During IMD outbreaks, public health practitioners must be especially attuned to these individual-level factors. During the 2012 Los Angeles IMD outbreak, high-risk MSM (ie, those who have close/intimate contact with multiple partners, those who visit bars or clubs, and those who smoke or use illegal drugs) were recommended to receive the vaccine. 6 During the 2016-2017 outbreak, the recommendation was broadened to all MSM, regardless of risk behaviors. 9 Although high-risk MSM have had years to respond to recommendations, MSM who do not engage in high-risk behaviors may hesitate to get vaccinated because of the recency of the recommendation change. Social marketing campaigns that emphasize vaccine recommendations in the context of an outbreak, along with additional information on individual risk assessment, may be useful.
In our multivariable model, the strongest predictor of MenACWY vaccine uptake was knowing anyone who had received the MenACWY vaccine. Health risk and protective behaviors tend to cluster within networks. 50 Because our data were cross-sectional, we could not determine the processes of selection and influence. It is conceivable that similar values on immunization and health behavior among peers made participants who had received the MenACWY vaccine more likely than participants who had not received the vaccine to know someone who had been vaccinated. It is also conceivable that people who get vaccinated and tell their friends cause greater MenACWY vaccine uptake in their networks. In Los Angeles County, outbreak messaging relied on social marketing strategies (eg, outdoor advertising) and advisories issued by LGBTQ-specific health care providers. Our findings indicated that network-based interventions may be particularly effective in increasing MenACWY vaccine uptake among MSM. Future interventions can recruit popular opinion leaders (ie, MSM who have been vaccinated and are influential among their peers) to promote MenACWY vaccination among MSM. Strong recommendations for MenACWY vaccination by health care providers who specialize in HIV care are needed routinely and during IMD outbreaks.
Limitations
Our study had several limitations. First, we excluded MSM aged <18 and MSM who did not attend LGBTQ-identified venues, so we cannot generalize our results to MSM who do not fit these criteria. Second, several sources of bias limited the ability of self-reported vaccination decisions to represent actual vaccination behavior, including recall, response, and social desirability bias. We included only those who responded yes or no to the question assessing MenACWY vaccination, thereby excluding those who were unsure about their vaccination status. Because our study was a rapid response to the unfolding events of the IMD outbreak, we could not verify vaccination status through a third party; therefore, we decided to exclude those who were unsure about having received the MenACWY vaccine. Future studies should seek to verify immunization status in collaboration with health care providers or with data from the California Immunization Registry. Third, our data were cross-sectional, and we could not make causal inferences.
Fourth, although we used venue-based sampling, a strategy that would theoretically result in generalizability, this sample may not be representative of all MSM in Los Angeles County. For example, although the sample was racially and ethnically diverse, most respondents were employed, insured, and well educated, and lived in areas not characterized by poverty (ie, in ZIP codes in which ≥20% of all families lived below the federal poverty level). When we compared the racial/ethnic distribution in our sample with the distribution found in probability samples of MSM in California (51.6% white, 5.1% black/African American, 35.0% Hispanic, and 8.3% other), 51 the distributions were somewhat similar, except that our sample had fewer non-Hispanic white men and more non-Hispanic black/African American men. Although other characteristics of our sample were somewhat similar to those in probability samples of MSM in California, 51 we cannot generalize our results to all MSM in California.
Conclusions
Given the heightened risk of IMD during an outbreak that primarily affected MSM, participants in our sample were not adequately protected against IMD. Our study offers important insights into the correlates of MenACWY vaccine uptake among MSM in Los Angeles County. Most HIV-positive MSM who reported receiving the MenACWY vaccine received ≥1 dose within the 6 months before participating in our study questionnaire, suggesting that public health and community stakeholder efforts influenced uptake during the outbreak. This result may also demonstrate that the health advisory issued by the California Department of Public Health that urged PLWHA to get vaccinated was successful. 52
Research on subgroups of MSM in nontraditional settings and/or those who are socially or geographically isolated in Southern California would help to inform vaccination outreach campaigns. Incorporating vaccination measures into population-based research, such as the National Health Interview Survey and the California Health Interview Survey, is also warranted to improve immunization surveillance among MSM. Future interventions should focus on getting HIV-positive men to complete the 2-dose MenACWY vaccine series. Education efforts targeting HIV care providers may be useful in reaching HIV-positive MSM. Greater challenges exist in improving MenACWY vaccination coverage among HIV-negative MSM during outbreaks. Vaccination promotion efforts must prioritize education and use tailored promotion strategies to reach this population. Failure to address the barriers and challenges that inhibit MSM from receiving MenACWY vaccine will likely result in more preventable deaths and lifelong impairments from IMD among MSM.
Footnotes
Acknowledgments
We express our gratitude to all participants in this study, to our data-collection team from the Luskin School of Public Affairs, and to other researchers who provided critical input into this article. We also thank Laurel Fowler, Michelle Parra, Franklin Pratt, and Kathleen Sanchez from the Los Angeles County Department of Public Health Immunization Program and Adam Cohen from the AIDS Healthcare Foundation for their valuable contributions. Finally, we thank the staff members of partner venues for their support during the implementation of this study. Our venue partners included 24 Hour Fitness, Akbar, Andrew Christian, APAIT, APLA Health, Circus of Books, Faultline, Fiesta Cantina, FLEX Spa, Gold’s Gym, Gold Coast Bar, GYM Sportsbar, Hamburger Mary’s, Los Angeles LGBT Youth Center, Micky’s, Mother Lode, New Jalisco Bar, Rage, Redline, Revolver Video Bar, Starbucks, and The Bullet Bar.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted by the Southern California HIV/AIDS Policy Research Centers, through a generous grant from the University of California HIV/AIDS Research Program (grant no. RP15-LA-007). Additional support was provided by the UCLA Center for HIV, Identification, Prevention, and Treatment Services funded by the National Institute of Mental Health (grant no. P30MH058107).